
Abstract
Background:
The clinical course of patients with lung metastases of differentiated thyroid carcinoma (DTC) vary, and cancer-specific survival (CSS) can be associated with tumor burden. This study evaluated the growth kinetics of lung metastases from DTC using serial chest computed tomography for Response Evaluation Criteria in Solid Tumors assessment and its prognostic implications.
Methods:
Forty-four patients with macronodular lung metastases (≥1 cm) of DTC were included. The time intervals to disease progression of lung metastases were measured and compared to CSS rates.
Results:
On the basis of the time to progression, 15 (34%), 17 (39%), and 12 (27%) patients were classified into the slow (≥3 years), moderate (1–3 years), and rapid groups (<1 year), respectively. The growth kinetics of lung metastases exhibited a linear pattern in the three groups. The doubling time of tumor burden was 1.8 years (R 2 = 0.973, p = 0.013) in the rapid group, and the estimated doubling time of the tumor burden in the moderate and slow groups was 5.9 years and 19.3 years, respectively. No independent variable predicted the growth kinetics of lung metastases. In multivariate analysis, disease progression within the first year was an independent predictor of CSS (hazard ratio = 8.6; p = 0.003).
Conclusions:
This is the first study to demonstrate objectively that tumor growth kinetics within the first year are an independent predictor of CSS in patients with macronodular lung metastases. Performing chest computed tomography at least twice a year in the early phase of the disease in patients with macronodular lung metastases may be helpful for identifying high-risk patients who are eligible for treatment with tyrosine kinase inhibitors.
Introduction
P
Response Evaluation Criteria in Solid Tumors (RECIST) have been applied to assess the tumor responses of patients with lung metastases of DTC after RAIT (9,10,12,16). Two recent Phase III trials of sorafenib and lenvatinib defined progressive RAI-refractory DTC as disease progression according to the RECIST after RAIT within 16 months and 12 months, respectively (14,15). RECIST defines objective tumor response based on the change in tumor burden, and tumor response according to RECIST is a prognostic factor for survival (17,18). Serial assessment of the metastatic tumor size and development of new metastatic lesions is an important component in the evaluation of tumor burden (17,18). Therefore, the frequency of repeated imaging evaluation during treatment should be adapted according to the tumor growth kinetics (17,18). More frequent assessment should be considered in patients with rapid progression, and less frequent imaging performed in patients with slow progression (2). Thus, identifying tumor growth kinetics of lung metastases in serial radiographic imaging is needed to guide the intensity of surveillance and timing of sorafenib or lenvatinib treatment.
This study evaluated the growth kinetics of lung metastases by using serial chest computed tomography (CT) scans per RECIST v1.1 and the doubling time of tumor burden in DTC patients with macronodular lung metastases. It also evaluated CSS according to the growth kinetics of lung metastases and the prognostic implication of rapidly increased tumor burden in the early periods after diagnosis of lung metastases. To the authors' knowledge, this is the first study to demonstrate tumor kinetics by axial scanning in patients with DTC. The findings will provide objective, evidence-based guidance for DTC patients with macronodular lung metastases for determining the frequency of radiographic imaging and early identification of high-risk patients eligible for TKI therapy.
Materials and Methods
Patients
The electronic medical records were reviewed of patients with DTC who underwent total thyroidectomy followed by high-dose RAIT between 1995 and 2013 at the Asan Medical Center, Seoul, Korea. Initially, 75 patients were included with measurable lung metastases of DTC, which were ≥1.0 cm in chest CT scans. Thirty-one patients were excluded for the following reasons: <18 years old, no available follow-up chest CT scan, and treatment with surgical excision or systemic chemotherapy for lung lesions. Finally, 44 patients were included with macronodular lung metastases of DTC. The study protocol was approved by the Institutional Review Board of the Asan Medical Center, Seoul, Korea.
Diagnosis of lung metastases
Synchronous lung metastasis was diagnosed in 18 patients, and metachronous lung metastasis was detected in the remaining 26 patients during a median follow-up of 9.5 years (interquartile ranges [IQR] 6.1–12.7). The diagnosis of lung metastases was based on clinical assessments, including the presence of RAI uptake in the lungs on diagnostic or therapeutic 131I whole-body scan (WBS), chest CT, and/or pathological findings of lung metastases. Chest CT was performed by using various scanners—Somatom Definition, Sensation-16 (Siemens Medical Systems, Forchheim, Germany), Lightspeed Volume CT, Discovery HD 750 (GE Healthcare, Milwaukee, WI, USA)—with 120 kVp, 30–200 mAs. Images were reconstructed using the sharp reconstruction algorithm with thicknesses of 2.5–3.0 mm. All CT scans were obtained in the supine position at full inspiration. Retrospective radiologic review was performed by two experienced radiologists (S.M.L. and J.H.L.).
Treatment and follow-up protocols
Patients for whom lung metastases were not detected before initial RAIT received 2.77–5.55 GBq (75–150 mCi) of 131I for remnant ablation therapy according to the initial staging. A high dose of 131I (7.4 GBq, 200 mCi) was administered to patients who were diagnosed as having lung metastases of DTC. Usually, repeated high-dose RAIT was performed at 12-month intervals until abnormal RAI uptake disappeared in post-therapeutic or diagnostic WBS. The physicians also determined treatment with additional RAIT considering the cumulative RAI doses or other clinical situations. Patients underwent RAIT after thyroxine (T4) withdrawal for five to six weeks, and low-iodine diet for two weeks. Serum thyrotropin (TSH), free T4, stimulated thyroglobulin (Tg), and anti-Tg antibody (TgAb) levels were measured, as previously described (19). Stimulated Tg levels were defined as Tg levels after T4 withdrawal with TSH levels >30 mIU/L. RAI avidity was defined as visible RAI uptake on WBS, and RAI non-avid metastases were defined as without RAI uptake or with uptake in <10% of lung nodules, as in a previous study (12). Patients were administered L-thyroxine to suppress serum TSH levels and followed up regularly with physical examinations, thyroid function tests, and serum Tg/TgAb measurements every three to six months, as previously described (19). Serum Tg doubling time (Tg-DT) was calculated only in patients with negative serum TgAb levels <100 IU/mL. Serum Tg levels with L-thyroxine suppressive therapy were used for the calculation of Tg-DT. Additional diagnostic imaging tests, such as chest X-ray and chest CT, were performed every 6–12 months.
Definition of disease progression
Structural disease response or progression was classified according to RECIST v1.1 (17). Target lesions were selected on the basis of their longest diameter and measured repeatedly by follow-up chest CT. When more than one measurable lesion was present at baseline in the lungs, up to two lesions were identified as target lesions, and the sum of the longest diameter for all target lesions was defined as the baseline tumor size.
Complete response (CR) was defined as no visible lesions in radiologic images. Taking the baseline diameter as reference, partial response (PR) was defined as at least a 30% decrease in the sum diameter of target lesions. Progressive disease (PD) was defined as at least 20% increase in the sum diameter of target lesions, with an absolute increase of sum diameter of at least 5 mm. The appearance of one or more new lesions was also considered as disease progression. Stable disease (SD) was defined as being neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD (17).
Classification of patients with macronodular lung metastases according to tumor growth kinetics
DTC patients with macronodular lung metastases were classified into three groups according to the tumor growth kinetics defined by RECIST in serial chest CT: (i) rapid group, who had PD less than a year after diagnosis of lung metastases; (ii) moderate group, who had PD between one and three years after diagnosis of lung metastases; and (iii) slow group, who had PD three or more years after diagnosis of lung metastases.
Statistical analysis
All statistical analyses were performed by using R v3.1.0 (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline characteristics of patients with macronodular lung metastases of DTC
Baseline characteristics of the 44 patients are listed in Table 1. The median age when diagnosed with lung metastases was 60.9 years old (IQR 51.7–66.4 years), and 20 (45%) patients were male. Thirty-one (70%) patients had papillary thyroid cancer (PTC), and 13 (30%) patients had follicular thyroid cancer (FTC). The median primary tumor size was 3.3 cm (IQR 2.5–4.7 cm). Cervical lymph node (LN) metastases, lymphovascular invasion, and extrathyroidal extension were present in 70%, 48%, and 70% of patients, respectively. Eighteen (41%) of 44 patients had RAI-avid lung metastases. The median dose of initial RAI was 5.6 GBq (150 mCi), and the median dose of cumulative RAI was 14.8 GBq (400 mCi). The median level of initial sTg in patients with negative serum TgAb was 47.4 ng/mL (IQR 12.0–401.0 ng/mL). The median largest diameter of lung metastases in the initial chest CT scan was 1.3 cm (IQR 1.0–1.8 cm).
Continuous variables are presented as the median with interquartile range. Categorical variables are presented as numbers with percentages.
RAI avidity at the diagnosis of lung metastases
PTC, papillary thyroid cancer; FTC, follicular thyroid cancer; RAI, radioactive iodine; sTg, stimulated thyroglobulin.
Tumor growth kinetics and doubling time of lung metastases in serial chest CT
The changes in tumor growth kinetics of lung metastases during a median 6.3 years (IQR 4.3–8.4 years) of follow-up were classified as slow (Fig. 1A), moderate (Fig. 1B), and rapid (Fig. 1C). Fifteen (34%) patients were in the slow group (≥3 years). Seventeen (39%) patients and 12 (27%) patients were classified into the moderate (1–3 years) and rapid (<1 year) groups, respectively (Table 2). The median tumor sizes, as measured by the sum of diameters of target lung lesions, were 1.2 cm (range 1.0–4.1 cm) on baseline chest CT scan and 2.5 cm (range 0.8–5.9 cm) on the last chest CT scan. The metastatic tumor size decreased in only two patients in the slow group.
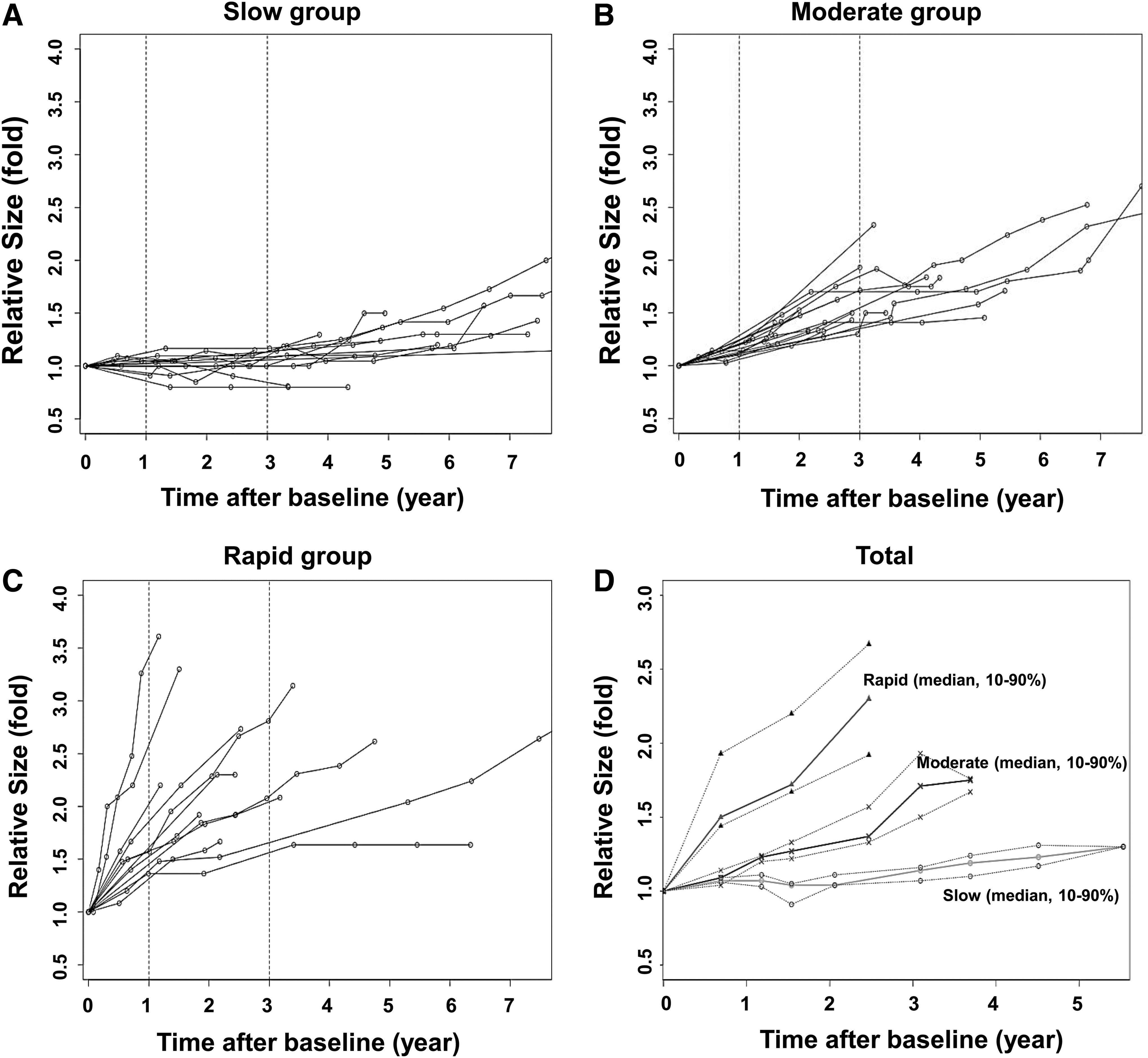
The change in relative tumor size measured by the sum of the diameters of target lung lesions over time in patients with macronodular lung metastases of differentiated thyroid carcinoma (DTC). (
Continuous variables are presented as the median with interquartile range. Categorical variables are presented as numbers with percentages.
RAI avidity at the diagnosis of lung metastases.
Patients having raised anti-Tg antibody were excluded from the Tg analyses.
p-Value is estimated by the Kruskal–Wallis test.
p-Value is estimated by the chi-square test.
p-Value is estimated by the trend analysis.
LN, lymph node; Tg-DT, Tg doubling-time.
The time trend of metastatic tumor growth exhibited linear kinetics in each group (R 2 = 0.973, p = 0.013, in the rapid group; R 2 = 0.951, p < 0.001, in the moderate group; and R 2 = 0.912, p < 0.001, in the slow group; Fig. 1D). The median doubling time of the sum of the longest diameters for all target lesions in the rapid group was 1.8 years ([80% CI 1.1–6.2]; Fig. 1). The estimated doubling time of the tumor burden based on the curves was 5.9 years [80% CI 4.9–7.9] in the moderate group and 19.3 years [80% CI 15.6–25.8] in the slow group.
Comparison of patients according to the metastatic tumor growth kinetics
There was no significant difference in age at diagnosis of lung metastases between the groups. The proportion of male patients was significantly higher in the rapid group (83%) than in the slow (33%) or moderate (29%) groups (p = 0.008). There were no significant differences in pathological subtype, primary tumor size, cervical LN metastasis, lymphovascular invasion, or extrathyroidal extension between the three groups. Additionally, there were no significant differences in RAI avidity, initial RAI dose, cumulative RAI dose, initial value of serum sTg, Tg-DT, or initial largest diameter of lung metastases between the three groups.
CSS and metastatic tumor growth kinetics
During a median 6.3 years of follow-up after diagnosis of lung metastases, 21 (48%) patients died due to progression of DTC. There were significant differences in CSS between the three groups (p = 0.029; Fig. 2A). When the slow group was compared with the moderate and rapid groups, there were no significant differences in CSS (p = 0.06; Fig. 2B). In univariate and multivariate analyses, disease progression of lung metastases within three years (slow vs. moderate and rapid groups) was not an independent predictor of CSS (unadjusted HR = 2.7 [CI 0.9–8.1], p = 0.072; adjusted HR = 2.0 [CI 0.5–8.3], p = 0.338, Model 3, respectively; left panel of Table 3).
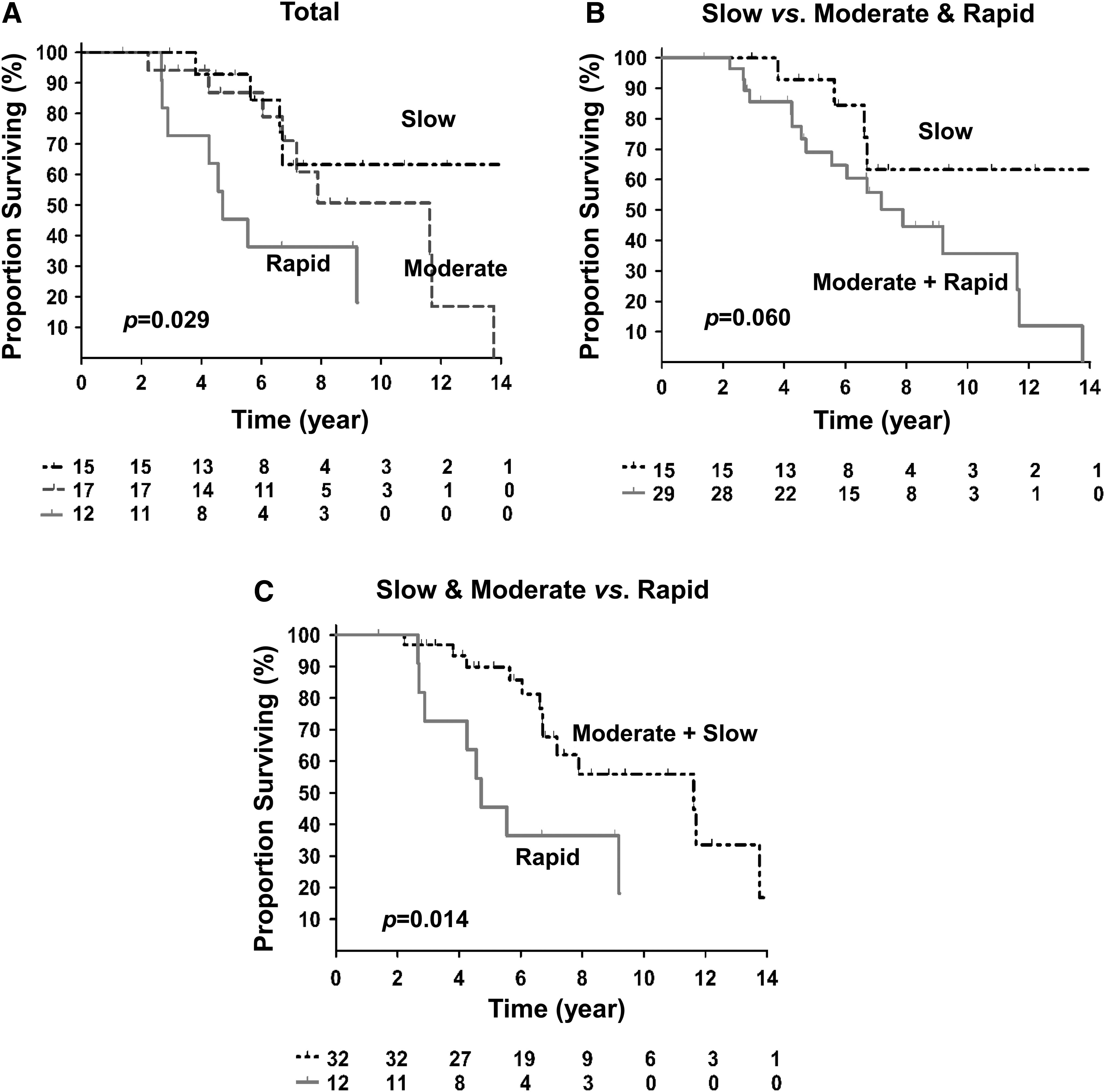
Cancer-specific survival (CSS) according to the tumor growth pattern of macronodular lung metastases in patients with DTC. (
The CSS of the moderate and rapid groups was compared with that of the slow group (left panel). Tumor progression within three years (moderate and rapid groups) was not significantly associated with CSS. The CSS of the rapid group was compared to that of the moderate and slow groups (right panel). Tumor progression within one year (rapid group) was significantly associated with poor CSS in univariate and multivariate analysis. Model 1 was adjusted for age and sex. Model 2 was adjusted for age, sex, tumor size, extrathyroidal extension, and cervical lymph node metastasis. Model 3 was adjusted as for Model 2 with additional adjustments for RAI avidity. p-Values were calculated using the Cox proportional hazard model.
CSS, cancer-specific survival; HR, hazard ratio; CI, confidence interval.
However, CSS was significantly shorter in the rapid group than it was in the other groups (p = 0.014; Fig. 2C). In multivariate analysis, disease progression of lung metastases within the first year (slow and moderate groups vs. rapid group) was an independent predictor of CSS after adjusting for age, sex, primary tumor size, extrathyroidal extension, cervical LN metastasis, and RAI avidity (HR = 8.6 [95% CI 2.7–35.6], p = 0.003, Model 3; right panel of Table 3). When the association between the patients with good RAI uptake and CSS were evaluated, RAI avidity was not significantly associated with CSS (p = 0.095).
Discussion
This study evaluated tumor growth kinetics of macronodular lung metastases by using serial CT findings in patients with DTC during a median of 6.3 years of follow-up. Increases in the rate of maximal diameters of lung lesions varied. Some patients exhibited disease progression within one year, but others had stable disease for more than three years. Patients were classified into three groups according to whether the progression of lung metastases occurred within one year or within three years. The results show that if lung metastases rapidly progressed according to RECIST within year 1 (rapid group), the relative risk of cancer-specific death was significantly increased by 8.6-fold in multivariate analysis after adjusting for age, sex, primary tumor size, extrathyroidal extension, cervical LN metastasis, and RAI avidity. In addition, changes in tumor burden based on serial chest CT exhibited a linear pattern and enabled prediction of the growth kinetics of lung metastases within a year. The doubling time of tumor burden was 1.8 years in the rapid group, and the estimated doubling time of the tumor burden in the moderate and slow groups was 5.9 years and 19.3 years, respectively. By estimating tumor growth kinetics by serial chest CT, it is possible to predict the clinical course of DTC patients with macronodular lung metastases. These findings support the concept that chest CT scans should be performed at least twice within a year after diagnosis in patients with macronodular lung metastases of DTC.
This study included patients with macronodular lung metastases defined as ≥1.0 cm on chest CT. The size of metastatic lung lesions measured by chest CT is known to be an important prognostic factor in patients with lung metastases of DTC (9,10,12). Patients with macronodular lung metastases have poor prognoses, despite repeated high-dose RAIT (9,10). Before approval of sorafenib and lenvatinib, high-dose RAIT was the only available therapeutic modality for treatment of patients with metastatic DTC, and high-dose RAIT was repeatedly administered, even though the effects were uncertain (11). After approval of the above-mentioned TKIs as new treatment options for metastatic, rapidly progressive, symptomatic, and/or imminently threatening disease of patients with RAI-refractory DTC, the issue of whom to treat and when to treat with TKIs emerged (2,14,15). Therefore, it is important to define the subgroup of patients expected to have poorer prognosis among those with macronodular lung metastases. The findings indicate that a rapid increase in tumor burden within the first year could be a critical factor to initiate TKI therapy in patients with macronocular lung metastases of DTC.
There was no independent clinicopathologic variable predictive of metastatic tumor growth kinetics in this study. RAI avidity, value of initial serum sTg, Tg-DT, and the largest diameter of lung metastases on initial chest CT were not significantly associated with increasing rate of tumor burden. The change in serial serum Tg levels over time and Tg-DT have been considered as another approach for predicting the disease progression rate (20). However, the tumor growth kinetics of lung metastases were not associated with Tg-DT. Measurement of serum Tg levels also had limited value because the levels were dependent on circulating serum TSH concentrations and interference by the positivity of serum TgAb (20,21). Therefore, patients should not be identified as having PD and requiring more aggressive therapy solely on the basis of rising levels of serum Tg (2).
This study has some limitations that should be considered. The study used a retrospective design, and the sample size is small. There is a possibility that the small number of patients could be associated with the insignificant correlation between RAI avidity and survival in this study. There is also a possibility of selection bias in a single tertiary referral institution. If the response of high-dose RAIT is heterogeneous among lung lesions, the change in target lesions might not reflect total tumor burden. The association between the most rapid disease progression and 18F-fluorodeoxyglucose-positron emission tomography (FDG-PET) could not be evaluated in this study. Only a limited number of patients were evaluated with FDG-PET because the national health insurance of Korea reimburses FDG-PET only for patients with RAI non-avid distant metastases, which cannot be detected by CT or magnetic resonance imaging. In addition, the volume of lung metastases could not be calculated in all patients. Thin-section CT imaging with 1 mm cuts for volumetric analysis was not available in some patients because patients were included from 1995. Doubling times had to be estimated based on the sum of target lesions according to the RECIST criteria rather than the volume of lung lesions. However, this is the first study to demonstrate objectively the clinical course and growth kinetics of macronodular lung metastases on serial chest CT scans by using RECIST for patients with DTC.
In conclusion, the tumor growth kinetics determined by serial chest CT within the first year after diagnosis of macronodular lung metastases were found to be an independent prognostic factor for predicting CSS in patients with DTC. Changes in the tumor burden of lung metastases exhibited linear kinetics. However, no independent variable was found to be predictive of the growth kinetics of lung metastases in this study. These findings suggest that regular chest CT scans should be performed at least twice within a year after diagnosis of macronodular lung metastases in patients with DTC. Estimating growth kinetics of lung metastasis can be helpful for the early identification patients with rapidly PD eligible for TKI therapy. This approach may provide objective, evidence-based guidance to counsel patients regarding their individual disease risk and allow them to participate more actively in decisions surrounding their management.
Footnotes
Acknowledgments
This study was supported by the National Research Foundation (NRF) of Korea Research Grant (NRF-2015R1C1A1A02036597). An abstract (OS-13) covering a part of this article was presented at the 12th Asia and Oceania Thyroid Association Congress (AOTA 2017), March 16–19, 2017, Busan, Korea.
Author Disclosure Statement
No authors have any conflicts of interest in relation to this manuscript.