
Abstract
Background:
It has recently been demonstrated that the combination of miRNA-190 and -95 (expressed as probability of malignant risk: pmiRNA) in the serum of Caucasian patients with thyroid nodular disease allows the identification of nodules at high risk of malignancy with great accuracy. The present study aimed to validate these results in a larger cohort of patients.
Materials and Methods:
This study prospectively analyzed 1000 patients. Cytological diagnosis was available in 982/1000 (98.2%) and histological diagnosis in 445/1000 (44.5%). The expression levels of circulating miRNA-190 and -95 were determined by real time polymerase chain reaction with the 2–ΔΔct method. The diagnostic performance (sensitivity, specificity, and accuracy) of fine-needle aspiration cytology (FNAC), pmiRNA, and a combination of the two methods was correlated with the cytological and histological diagnoses.
Results:
The combination of pmiRNA and FNAC significantly increased the sensitivity (96.3%) with respect to each method alone (88.9% for FNAC and 89.6% for pmiRNA) by reducing the rate of false-negative results from 18 for FNAC and 17 for pmiRNA to only five. In patients in whom FNAC was not performed (n = 14) or in those with inadequate (n = 18) or indeterminate (n = 72) lesions submitted to surgery, pmiRNA correctly identified 90.8% of patients with benign disease and 74.3% of patients with cancer.
Conclusions:
These results confirm that a combination of serum expression levels of miRNA-95 and −190 is an accurate and noninvasive tool for the differential diagnosis of thyroid nodules in the Italian population.
Introduction
M
The use of the expression of circulating miRNA compared to those in the tissues would be preferable, since blood samples may be obtained by a simple and minimally invasive procedure. The mechanisms underlying the release of miRNAs in the blood from cancer tissue are still under investigation, but it is speculated that circulating miRNAs derive from tumor necrosis or lysis, or direct secretion from cancer cells, or are related to the immune response against the tumor (3).
The authors' group evaluated for the first time the expression profile of miRNAs in the serum of Caucasian patients with nodular thyroid disease and healthy subjects (4). Four miRNAs were deregulated in PTC patients. In particular, miRNA-190 was upregulated, and miRNA-95, -579, and -29b were downregulated. The expression levels of miRNA-190 and −95 were combined in a mathematical formula, resulting in a value, called pmiRNA, which estimated the risk of malignancy for each patient, with a cutoff of 0.5. Values >0.5 were correlated with an increased risk of malignancy. The pmiRNA showed a very high diagnostic power, with an area under the curve (AUC%) of 99.0% [confidence interval (CI) 96.9–100%]. A correlation was also observed between the expression levels of miRNA-190 and -95 in the serum and in the corresponding tumoral tissue. The miRNA expression was not correlated with the age and sex of patients, presence of chronic lymphocytic thyroiditis, pathological features of cancer (tumor diameter, multifocality, bilaterality, histological variant, lymph node, or distant metastases), patient outcome, or presence of genetic alterations such as RET/PTC, RAS, and BRAF.
The present study aimed to validating the preliminary data (4) in the differential diagnosis of thyroid nodules in a prospective larger series of patients.
Patients and Methods
Patients
A total of 1000 patients (754 female) with nodular thyroid disease (M age = 54 years; SD = 14 years; range 14–88 years), consecutively selected at the authors' institution for fine-needle aspiration cytology (FNAC) from January 2014 to March 2013, were enrolled in this study. Cytological diagnosis was available in 982/1000 (98.2%) patients. The study was approved by the local ethics committee. Consent and blood specimen were collected before FNAC. Of the total patients, 445 (44.5%) were treated surgically with total thyroidectomy. At final histology, 243/445 (54.6%) patients had benign disease (F:M = 179:64; M age = 53.2 years, SD = 12.6 years) represented by hyperplastic nodules in 216 cases and follicular adenomas in 27. Of the 445 patients treated surgically, 202 (45.4%) had differentiated thyroid carcinoma (DTC; F:M = 139:52; M age = 53.2 years, SD = 12.6 years), 192 had papillary thyroid carcinoma (PTC; classical variant in 113 cases, follicular variant in 44, sclerosing variant in 17, columnar/tall-cell variant in 12, and a less common variant in six patients), seven had follicular thyroid carcinoma (FTC), and three had Hürthle cell carcinoma. Of the 202 patients with DTC, 96 (47.5%) showed an intrathyroidal tumor, while 105/202 (52%) patients had minimal extrathyroidal extension of the tumor. Cervical lymph node metastases were present in 57/202 (28.2%) patients, and distant metastases were found in 8/202 (4%) patients; 80/202 (39.6%) patients had multifocal disease, and 20/80 (25%) had a tumor limited to one lobe.
Methods
miRNA were extracted from 200 μL of serum using the miRNeasy Serum/Plasma Kit (Qiagen), according to the manufacturer's instructions. Reverse transcriptase reactions were carried out with miScript II RT Kit (Qiagen). RNA (5 μL) was used for each sample, adding 4 μL of 5 × miScript Hispec Buffer, 2 μL of 10 × miScript Nucleics Mix, 7 μL of RNase-free water, and 2 μL of miScript Reverse Transcriptase Mix. Reactions were subjected to the following program: 37°C for 60 min, and 95°C for 5 min. cDNA (2 μL) was used as a template for real time polymerase chain reaction (RT-PCR) to measure miRNA expression levels with the miScript SYBR Green PCR Kit (Qiagen) with specific primers for miRNA-95 and -190 (Qiagen). RT-PCR was performed in duplicate on the Rotor-gene Q MDx (Qiagen) under the following cycling conditions: 95°C for 15 min, 40 cycles at 94°C for 15 s, 55°C for 30 s, and 70°C for 30 s. Relative expression levels were calculated using the 2-ΔΔct method, with the miRNA-16 as an endogenous control. Cytological results were classified based on the Bethesda classification system (5).
pmiRNA
By applying a logistic regression model, a mathematical formula was developed that calculates the probability of malignancy (pmiRNA) with a cutoff value of 0.5, above which the patient was at high risk of malignancy. Details of this formula are reported in a previous study (4).
Statistical analysis
Statistical analysis was performed using Statview for Windows v5.0.1 (SAS Institute). The diagnostic accuracy of each test (pmiRNA or FNAC) or their combination was calculated as the proportion of true positives and true negatives according to FNAC results (cytological series) or to histology (histological series). The sensitivity was calculated as true positive (TP)/TP + false negative (FN), the specificity as true negative (TN)/TN + false positive (FP), the positive predictive value (PPV) of the test as TP/TP + FP, and the negative predictive value (NPV) of the test as TN/TN + FN. Differences between groups were analyzed with the Mann–Whitney U-test (two groups) or Kruskal–Wallis test (three or more groups) and the chi-square test for continuous or nominal variables. A p-value of <0.05 was considered statistically significant. The study parameters are expressed as the mean ± standard deviation.
Results
Cytological series (982 patients)
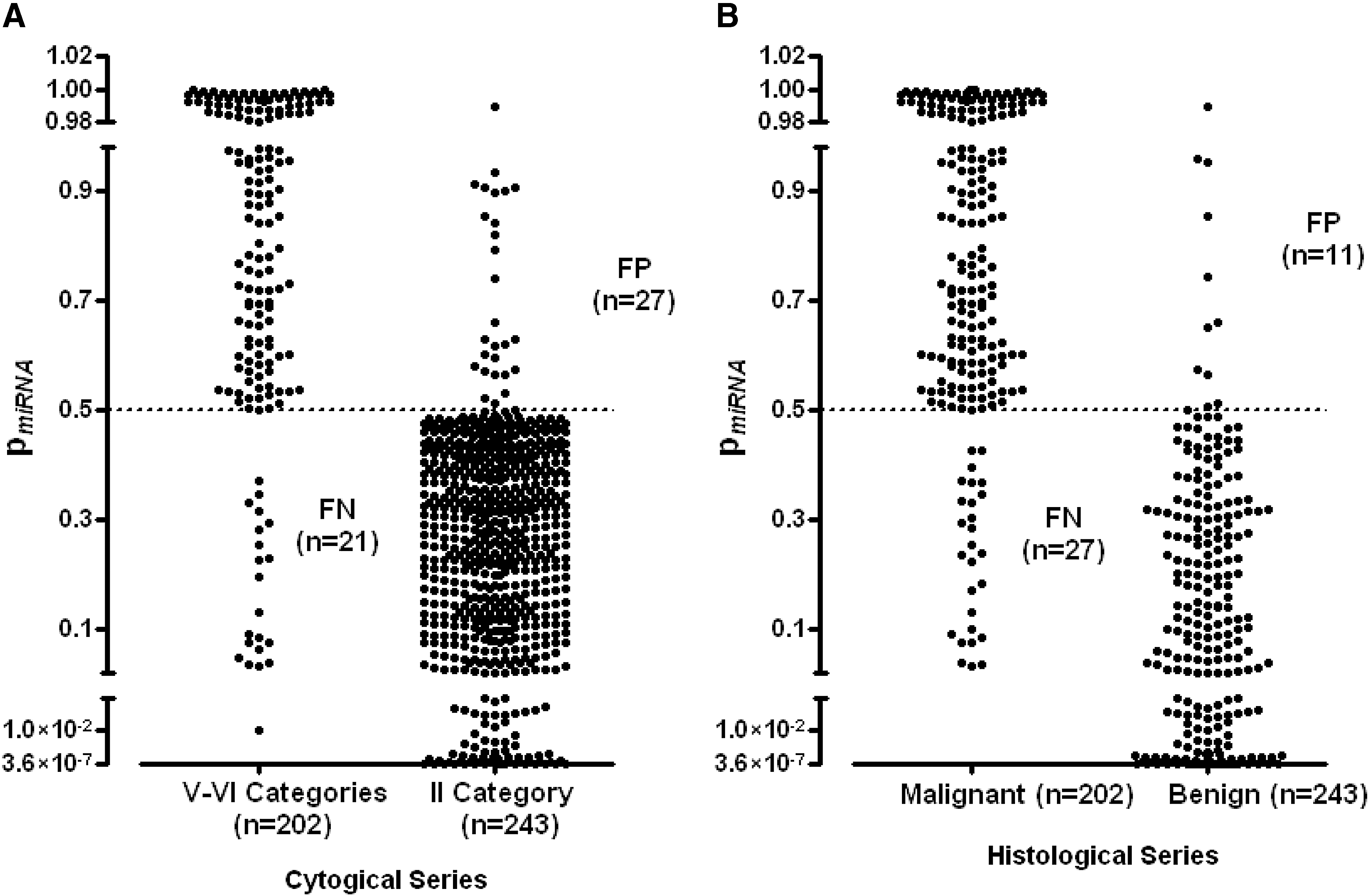
At cytology, 49/982 (4.9%) patients had a diagnosis of inadequate (category I) and 114/982 (11.6%) of indeterminate (category III–IV) lesions. These cases were excluded from the analysis. In 165/982 (16.8%) patients, the cytological diagnosis was suspicious for malignancy (category V–VI), and in 655/982 (66.7%), the diagnosis was benign lesion (category II). pmiRNA correctly identified 87.3% of the malignant cases and 95.9% of the benign lesions (Fig. 1A). The rate of false-negative or false-positive results was 21/165 (12.7%) and 27/655 (4.1%), respectively. The overall diagnostic performance of pmiRNA is reported in Table 1.
(
pmiRNA, probability of malignancy.
Histological series (445 patients)
Patients undergoing thyroidectomy were diagnosed at cytology as category I in 18 (4%) cases, category II in 188 (42.2%) cases, categories III–IV in 72 (16.1%) cases, category V in 40 (8.9%) cases, and category VI in 113 (25.4%) cases; 14 (3.1%) patients were treated surgically without performing FNAC. At histology, 243/445 (54.6%) had benign nodules, and 202/445 (45.4%) had malignant lesions. pmiRNA correctly identified 87% of cancers and 95.5% of benign nodules, showing a PPV of 94.1% and a NPV of 89.9% (Table 1). Considering all cytological categories, in the histological series, pmiRNA failed to diagnose 27/202 (13.4%) malignant nodules (FN) and 11/243 (4.5%) benign nodules (FP; Fig. 1B). In the histological series, there were no epidemiological, clinical, or pathological differences between FP and TN in the benign category and between FN and TP in the malignant group in terms of age, sex, history of current or previous benign or malignant tumors, thyrotropin values, uni- or multinodular goiter, thyroid volume, coexistence of chronic autoimmune thyroiditis, TNM, and histological variant.
Combination of pmiRNA and FNAC
Diagnostic categories (category II–V–VI = 341 patients)
The combination of pmiRNA and FNAC significantly increased the sensitivity (96.3%) with respect to each method alone (88.9% for FNAC and 89.6% for pMIRNA) by reducing the false-negative rate from 18 for FNAC and 17 for pMIRNA to only five (Table 2). However, an increase in the number of FP was observed, with a minimal decrease in specificity (Table 2).
FNAC, fine-needle aspiration cytology; FN, false negative; FP, false positive.
Unknown cytological category (category X = 14 patients), non-diagnostic (category I = 18 patients), and indeterminate lesions (category III–IV = 72 patients)
Fourteen of 18 patients with no cytological diagnosis, 18/48 with inadequate lesions (category I), and 72/114 with indeterminate lesions (category III–IV) at cytology underwent surgery.
At histology, patients who did not undergo FNAC had PTC in three cases and hyperplastic nodules in 11 cases. Patients with category I cytology were diagnosed as hyperplastic nodules in 13 cases, PTC in 14 cases, and FTC in one case. Patients with category III–IV cytology were diagnosed as follicular adenomas in 13 cases, hyperplastic nodules in 27 cases, PTC in 27 cases, FTC in three cases, and Hürthle cell carcinoma in two cases.
As shown in Table 3, pmiRNA correctly identified 90.8% of patients with benign disease and 74.3% of patients with cancer in the group of non-diagnostic cytological lesions (category X, I, and III–IV). Ten false-negative cases were observed, represented by eight patients with PTC (three classic, four follicular, and one tall-cell variant), one with FTC, and one with Hürthle cell carcinoma, and six false-positive cases with histological diagnosis of hyperplastic nodules in five cases and follicular adenoma in one case. If the analysis was limited to the group of indeterminate lesions (category III and IV), pmiRNA showed a PPV of 79.3% and a NPV of 79.1%. There were nine false-negative samples (one FTC, one Hürthle cell carcinoma, and seven PTC) and six false-positive cases (five hyperplastic nodules and one follicular adenoma).
Discussion
FNAC is currently considered the gold standard for the differential diagnosis of thyroid nodules. However, the diagnostic accuracy of FNAC is limited in cases of indeterminate lesions or samples with insufficient or inadequate material (6,7). The diagnosis of thyroid nodules has been significantly improved by searching cancer-specific genetic alterations in the material obtained by FNAC (8,9). However, some patients are still undergoing thyroidectomy for diagnostic purposes due to inconclusive results. Previous studies have analyzed the expression profile of miRNAs in tissue or cytological samples showing significantly different levels of miRNAs between benign and malignant thyroid lesions (10 –13).
Recently, several authors have reported that circulating miRNAs are stable and easy to detect in the serum, and may be used as diagnostic or prognostic markers for different cancer types (2,14,15). Two studies, one performed in China (16) and one in Italy (4), have analyzed the expression profile of serum miRNAs in patients with benign nodular goiter and thyroid cancer. Yu et al. have identified three miRNAs (let-7e, miRNA-151-5p, and miRNA-222) significantly overexpressed in the serum of PTC patients compared to healthy subjects and patients with benign nodules. Cantara et al. have extensively studied (4), for the first time, the expression profile of miRNAs in the serum of Caucasian patients with DTC or benign goiter and healthy subjects, and have found two miRNAs, -95 and -190, that in combination (pmiRNA) show great accuracy in the differential diagnosis of thyroid nodules.
The present work aimed to validate the results of a preliminary study in a larger cohort of patients. As previously reported, false-negative and -positive cases did not correlate with clinical or histopathological features. The study cohort also included seven cases of follicular cancer and three cases of Hürthle cell carcinoma, and although pmiRNAs showed high accuracy in these histotypes, the small number of cases does not allow a firm conclusion to be drawn about the use of pmiRNAs as diagnostic tool in these types of cancer. The diagnostic accuracy of the pmiRNA profile was similar to that of FNAC, and the combination of the two methods showed a significant improvement in the sensitivity and NPV with respect to each method separately. Therefore, pmiRNA analysis may represent a useful complementary diagnostic approach to FNAC performed on thyroid nodules following the recent American Thyroid Association guidelines (7).
In conclusion, the present study confirmed that the combination of two miRNAs, -90 and -195, differently expressed in the serum of DTC patients, may be used with great accuracy for the differential diagnosis of thyroid nodules, in particular in cases with a non-diagnostic cytology.
Currently, two other methods are commercially available for the differential diagnosis of indeterminate lesions with a similar accuracy as pmiRNA analysis: a next generation sequencing assay, ThyroSeq® v.2, with very high PPV and NPV and a rule-in approach, or a gene expression classifier, Afirma ® , with a good NPV but a low PPV and a rule-out approach (17 –19). The miRNAs identified in this study are not consistent with those found in the Chinese study (16). This discrepancy may be due to differences in technique or a different genetic background. Therefore, prospective studies performed with similar techniques and involving patients from several ethnic groups are needed to validate the clinical relevance of the present findings.
Footnotes
Acknowledgments
This work was supported by the Italian Ministry of Health (Grant #RF-2011-02350673) and by PRIN (#2012Z3F7HE).
Author Disclosure Statement
The authors have nothing to declare.