
Abstract
Background:
The management of differentiated thyroid cancer has traditionally consisted of total thyroidectomy with or without adjuvant radioactive iodine. However, in the last two decades, this approach has been challenged, with the consideration of more conservative approaches such as less radical surgery and deferring adjuvant treatment, especially in lower-risk patients. The objective of this study was to consider the effectiveness of current treatment options by comparing the survival outcomes from different geographic regions with different treatment philosophies. This study design was based on the concept of natural experiments in patient care that occur when physicians in different regions treat the spectrum of typical patients with varying treatments.
Method:
This population-based retrospective cohort study investigated 2444 patients with differentiated thyroid cancer ≤4 cm between 1990 and 2001 from Ontario, Canada. Extent of disease and extent of surgery were abstracted from pathology reports and were linked to downstream administrative medical information on treatments and outcomes. Patient demographics, tumor characteristics, treatments, and outcomes were compared between those geographic regions with more aggressive treatments and those regions with less aggressive treatments.
Results:
Treatment varied across the province. When comparing outcomes in regions where patients had more extensive treatment to those in regions where patients had less extensive therapy, similar rates were found for 15-year survival, recurrence, and survival after recurrence.
Conclusion:
There were significant variations in treatment but no differences in outcomes for regions with more versus less aggressive approaches. These findings support the trend toward more conservative management approaches in the treatment of thyroid cancer.
Introduction
T
The evidence on treatments and extent of treatments has been recently reviewed by Sawka et al. (8) and McLeod et al. (9). Both studies acknowledge that there is no level 1 evidence on the question of the extent of surgery (10) and that the observational studies used as the basis of current treatments, including Surveillance, Epidemiology, and End Results–based studies, have conflicting results. A commonly cited observational study on extent of surgery by Bilimora et al. (11) found improved overall survival (OS) with total thyroidectomy over lobectomy (p < 0.05) based on the National Cancer Database (n = 52,173). Their reported survival benefit, regardless of tumor size, was only 1.3% (97.1–98.4%), leading authors, including McLeod et al. (9), to conclude that “the small absolute benefits obtained from total thyroidectomy may be outweighed by other considerations” that might include potential complications of surgery. Adjuvant 131I therapy is used both to destroy residual disease after surgery and to facilitate long-term follow-up, but despite systematic reviews, large multicenter observational studies, and meta-analyses, the evidence of a significant reduction in mortality, especially in low-risk patients, is lacking. Sawka et al. (8) concluded that RAI is of most benefit to those with higher-risk disease and some with intermediate-risk disease, but the “benefits in patients with low risk disease are not clearly established.” Jonklaas et al. (12) analyzed both extent of surgery and the use of adjuvant RAI in a study based on 2936 patients in a multi-institutional prospective cancer registry. For the low-risk disease group (>50% of the patients), they found that improved survival “was not associated with any particular therapy,” as neither more extensive surgery nor the addition of RAI had an impact on OS or disease-specific survival (DSS).
This article reports on a retrospective population-based cohort study that linked clinical data (pathology reports) to electronic data (demographics, treatments, and outcomes) on all patients with DTC ≤4 cm diagnosed in Ontario, Canada, between January 1, 1990, and December, 31 2001. The objective was to consider the effectiveness of current treatment options by comparing the survival outcomes from different geographic regions to different treatment philosophies. The study takes advantage of both the natural experiments on treatment effectiveness that occur when the spectrum of typical patients in different regions receive different treatments and the unique research opportunity when the administrative data sets of a universal healthcare system are linked to pathology reports for a complete population of patients. A tumor of 4 cm is one parameter separating higher from lower risk, and 4 cm was selected initially to separate lower-risk cancer patients from higher-risk patients.
Methods
Study design and setting
This was a population-based retrospective cohort study, including all patients who had definitive surgery for DTC ≤4 cm in Ontario, Canada, between January 1, 1990, and December 31, 2001, followed until December 31, 2011.
Data collection
Case identification
The Ontario Cancer Registry (OCR) (13) is a population-based tumor registry operated by Cancer Care Ontario (CCO) including all patients with cancer, excluding non-melanoma skin cancer, since 1982. Patients were identified with a new diagnosis of thyroid cancer (ICD9 193) established between January 1, 1990, and December 31, 2001, with the specific histology codes for all papillary and follicular carcinomas (n = 7459; Fig. 1).

Summary of data collection and creation of the study populations.
Sampling
Previous investigations had demonstrated wide variations in treatments across the geographic regions of the province when defined by eight regional cancer treatment centers of Ontario (CCORs), regions that have been used extensively for population-based oncology research (14). The Toronto CCOR included 47% of the population of Ontario, and to ensure generalizability as well as to reduce study costs in the pathology review portion of the study, only every fourth (25%) OCR case was sampled by date of diagnosis from the Toronto CCOR for each year plus all patients from the remainder of the province (n = 4091).
Pathology report review
All thyroid cancer–related surgical pathology reports for the 4091 cases were requested from date of diagnosis forward from the OCR. Patients with a fine-needle aspiration biopsy or biopsy only were excluded. The 6746 reports were abstracted by two trained research associates for variables related to histological features, extent of disease, and extent of surgery. A total of 837 cases were excluded (Fig. 1).
Database linkage
The Institute of Clinical and Evaluative Sciences (ICES) is an independent, nonprofit research organization funded by the Ontario Ministry of Health and Long-Term Care. The 3254 patients were linked at ICES to the Ontario Health Insurance Plan physician billing codes with dates (surgery, type of surgery, RAI treatment), to the Canadian Institutes of Health Information for hospital procedure codes (surgery, types of surgery, RAI treatment, dates of treatment), and to CCO databases for radiotherapy information. One hundred and thirty-two patients could not be linked, leaving 3122 cases. Values of five or fewer subjects could be reported in order to protect the privacy of personal health information. To focus the study on patients whose initial treatment was for malignancy, 238 patients whose malignant thyroid tumor was <1 cm with associated benign nodule(s) >2 cm were excluded because these patients were likely to have had surgery for other indications.
Study populations
The overall provincial data set, including all eight regions, was re-created by reweighting the Toronto region based on the sampling strategy (4:1; n = 6212). Patients with tumors ≤4 cm were the specific study population (n = 2444). Two subgroups were also identified: all females with papillary cancer ≤4 cm (the most common clinical scenario), and all “low-risk” patients (<45 years, tumor ≤4 cm, low-grade histology, no extrathyroidal invasion, and M0) (15).
Personal health information
Values for variables on five or fewer subjects could not be reported (ICES policy).
Independent variables
Age was dichotomized based on 45 years, according to current risk stratification based on version 7 of the TNM classification (16).
Comorbidity was estimated using the Elixhauser scale for administrative data (17 –19) based on look back prior to diagnosis beginning 1988. Elixhauser is a summative scale over 30 domains based on hospitalization data, and cut points of 0, 1, 2, >2 were utilized (17,20), with increasing comorbidity having higher scores.
Histology was divided into three subgroups of papillary-favorable histology, papillary-unfavorable histology, and follicular thyroid cancer. The papillary-unfavorable group included patients with more aggressive histology, including the tall-cell, columnar-cell, and diffuse-sclerosing variants. Other abstracted histological features of the primary tumor included margins, single versus multiple foci, extrathyroidal spread, lymphatic invasion, and angioinvasion. The number of harvested lymph nodes and the number of positive lymph nodes were recorded.
Risk strata included the Memorial Sloan Kettering scale (MSK) (15) and TNM stage groups (16) based on characteristics including age, sex, tumor size, histological features, T category, and N category. M category could not be assigned, as no data on or surrogate for metastases were available electronically. MSK was chosen due to restrictions of data availability.
The index surgical procedures based on the pathology reports were lobectomy or total thyroidectomy. Incisional biopsy cases or nodulectomy without subsequent therapeutic surgery were excluded and subtotal thyroidectomy was included with total thyroidectomy, consistent with other studies (11,15).
Initial treatment was based on all information, including pathology reports and the operative note if obtained. The distributions of time between treatments were used based on preliminary work and the advice of the expert co-investigators to sort out sequences in order to define initial versus salvage treatments. For example, a patient who had a completion thyroidectomy within 90 days of lobectomy was classified as an initial total thyroidectomy unless recurrence was clearly stated in the documentation. Treatments such as combinations with radiotherapy or inconsistent sequences such as RAI after biopsy only were grouped as “other.” The initial treatments were: (i) lobectomy ± isthmusectomy; (ii) lobectomy ± isthmusectomy plus completion thyroidectomy within 12 months; (iii) total thyroidectomy; (iv) total thyroidectomy plus RAI within 12 months; (v) lobectomy ± isthmusectomy plus completion thyroidectomy within 12 months plus RAI within 12 months; and (vi) other.
Tumor size (cm) was based on the pathology report of the largest malignant nodule. As reports were being reviewed from hospitals of every size, location, and level of expertise across the province between 1990 and 2001, the quality and completeness of the reports varied. For example, rules had to be created for size assignment when the exact dimensions of the tumor were unreported. When the tumor size was stated as “little,” “focal,” “tiny,” “microscopic,” or “occult” but no size/dimensions were provided, tumor size was estimated at 0.49 cm (T1). If tumor size was reported as a range (e.g., 2–3 cm), the size would be captured as the medium value (e.g., 2.5 cm). In some cases, there was only sufficient information to assign TNM stage (n = 93).
The numbers of lymph nodes removed and the number of positive nodes reported were recorded and classified as 0, 1–5, and >5. In the occasional situation of poor-quality pathology reports, the numbers of nodes had to extrapolated from words such as “few” or “many,” which became 1–5 and >5, respectively.
Dependent variables
Vital status and cause of death were captured from multiple sources, including the Ontario Registrar General, the Ontario Death Registry, and hospitalizations. Only patients who moved out of Ontario were lost to follow-up. There are 15 years of follow-up data on 50.3% of cases based on death clearance as of December 31, 2011. Of the 2444 patients, 267 (10.9%) had died, including 54 who died of thyroid cancer. Of the remaining 213 patients who died, 17 had had thyroid cancer treatment (RAI, surgery, radiotherapy) or had a positive biopsy for thyroid cancer within one year of death. Assuming either a contribution to death by the thyroid cancer or a mistake on the death certificate, the survival analysis for DSS includes those patients for a total of 71 (2.9%) patients who died of thyroid cancer.
First recurrence and the date of first recurrence was defined as a subsequent treatment event after the completion of initial treatment, including a positive biopsy (pathology report), a surgical procedure targeting the thyroid bed, a neck dissection, a first treatment with RAI, a second treatment with RAI, radiotherapy when diagnosis was thyroid cancer, or death due to thyroid cancer when no subsequent treatment had been given.
Statistical analysis
For the descriptive analysis of all 6212 patients, the proportions are reported rather than actual values due to re-weighting. The remainder of the analysis is based on the 2444 patients with tumors ≤4 cm.
For the survival analysis, the Kaplan–Meier method was utilized with log-rank tests and Cox proportional hazards regression models (hazard ratios [HR], confidence intervals [CI], and p-values). The baseline variables were age <45 years, female, comorbidity = 0, well-differentiated histology, unifocal no lymphatic invasion, no vascular invasion, clear surgical margins, tumor 1–2 cm, no extrathyroidal spread, no regional lymph node involvement, MSK low risk, and TNM stage 1. The models that included risk (MSK) and stage group (TNM) were run separately, as the risk strata are made up of multiple factors and are not independent.
Logistic regression was used to model the patient factors and tumor factors that independently triggered the decisions on extent of surgery (total thyroidectomy, yes/no; RAI, yes/no) for all patients with tumors ≤4 cm.
Results
This section begins by reporting on all 6212 patients and then progresses through groups with less severe cancers, including all patients with tumors <4 cm, all female patients with papillary cancers <4 cm, and finally all “low-risk” patients. This section finishes with a comparison of prognostic factors to indications for treatment.
All patients with thyroid cancer (n = 6212)
The number of cases with thyroid cancer increased in Ontario from 309 to 797 per year, an increase >150% over the 11 years. As expected, the majority of the patients were female (78.8%), young ≤45 years (55.9%), and healthy (63% with no comorbidity) with favorable histology (89.9%). Of all the cases, 89.7% had tumors ≤4 cm in size, 61.4% had tumors ≤2 cm in size, 80.2% had no lymph node involvement, and 76% of patients were TNM stage I. A total of 39.2% of patients were designated MSK low risk.
Over the 11-year study period, the rate of total thyroidectomy rose from 53.4% to 63.6%, and the rate of RAI increased from 20.8% to 47.8%. A total of 31.1% of the patients underwent initial lobectomy (with 36% proceeding to completion thyroidectomy), and 62.6% had initial total thyroidectomy. Overall, 73.8% patients had total thyroidectomy as initial treatment, and 61.5% of those received RAI within the first year. One hundred and eighty-two (2.9%) patients received external beam radiotherapy within the first year.
Figure 2 presents the DSS curves for all patients based on the MSK risk criteria.
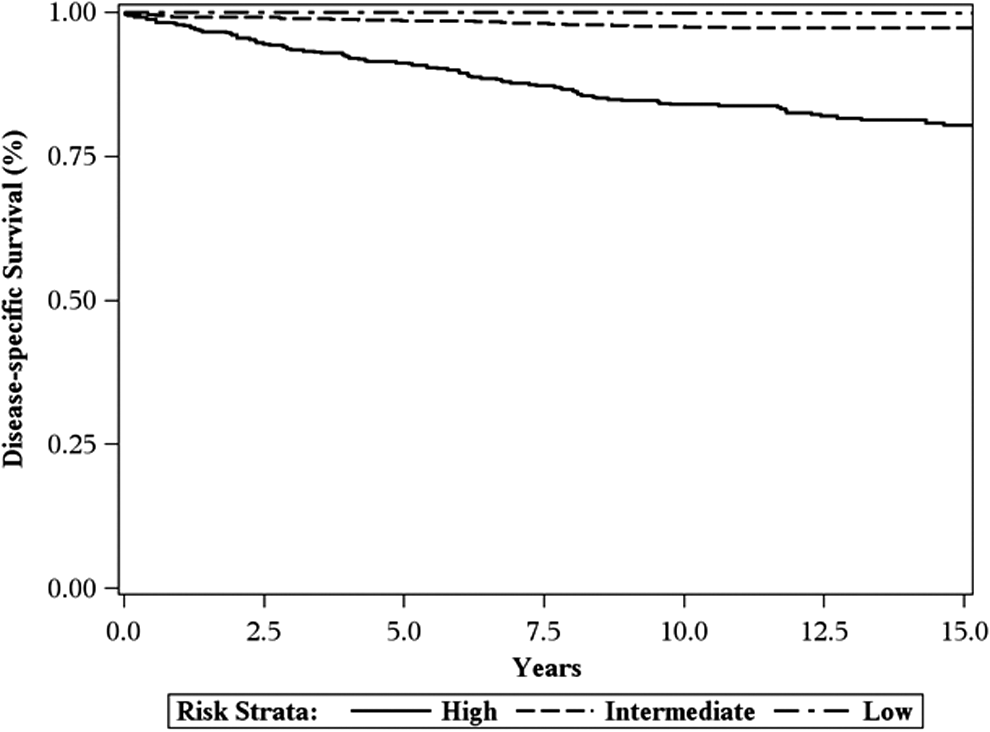
Disease-specific survival (DSS) by risk strata (Memorial Sloan Kettering) for all patients with tumors ≤4 cm.
Extent of treatment regions
Based on treatment location for all 6212 patients, the rates of total thyroidectomy (initial treatment) varied across the eight geographic regions from 44% to 67% (median 51.5%). The eight regions were divided into two groups of treatment regions based on a cut point of 60%, with patients in treatment regions A having a ≥60% rate of total thyroidectomy and patients in treatment regions B having a <60% rate of total thyroidectomy.
All patients with tumors ≤4 cm (n = 2440)
Of all the patients, 78.6% had tumors ≤4 cm. The population is described and compared for regions A versus B in Table 1. Patients in regions A were healthier with smaller tumors that had less aggressive histological features. Patients from regions A had a higher rate of extrathyroidal spread, and there was no difference in the number of involved nodes. There was no difference in rates across the MSK risk strata, with 11–12% of patients classified as high risk.
TNM, tumor, node, metastasis; MSK, Memorial Sloan Kettering scale.
Treatment was variable between regions (Table 2), with 69.3% of patients from regions A having initial total thyroidectomy versus 52.1% in regions B, and of those who had total thyroidectomy as initial treatment, 63.8% went on to adjuvant RAI treatments in regions A versus 39.6% in regions B.
RAI, radioactive iodine.
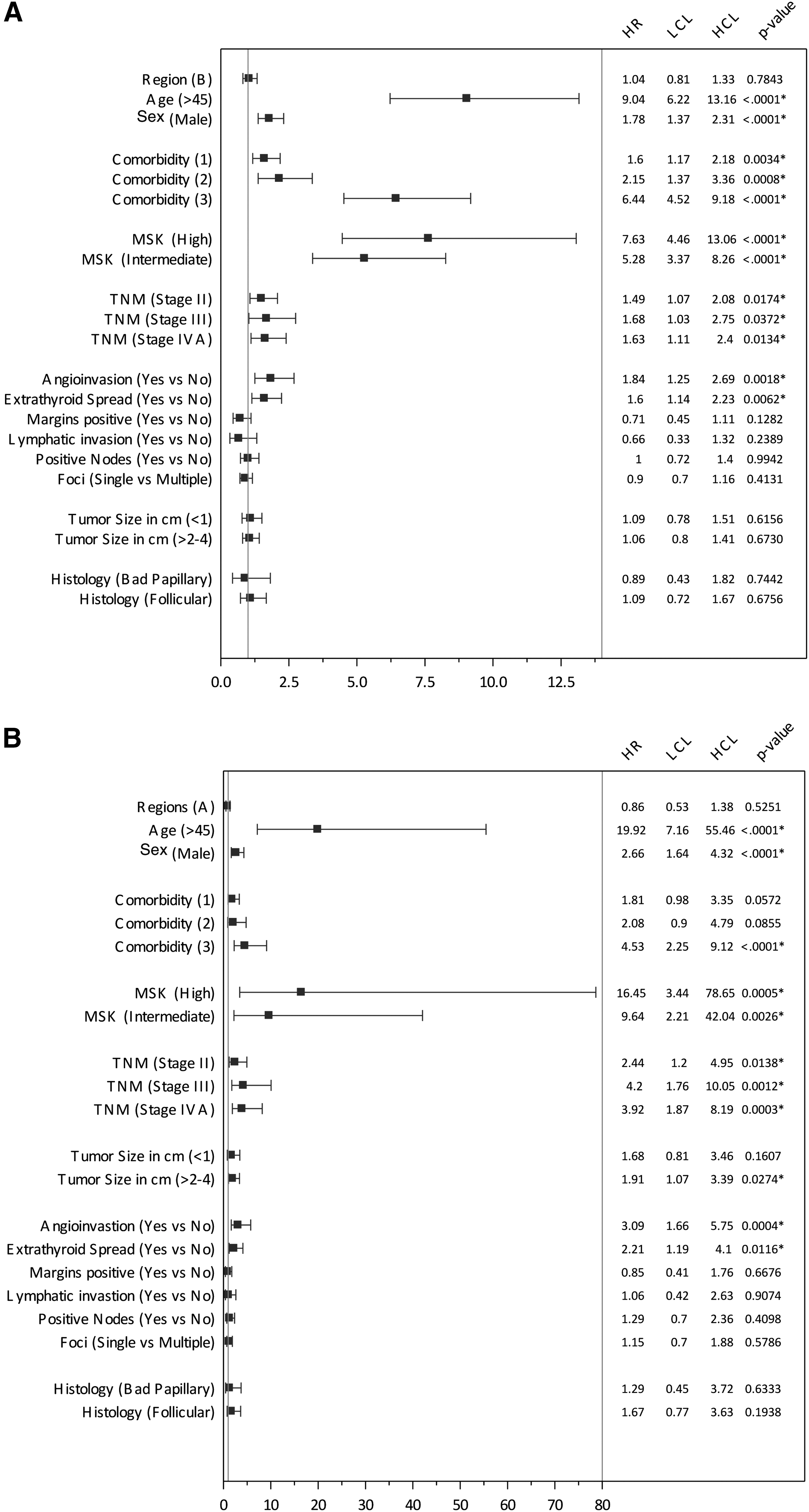
The 15-year OS for all patients was 90%, and DSS was 97%. When comparing treatment outcomes for regions A and B, there was no statistically significant difference in OS, DSS, or disease-free survival (Table 3). Similarly, there were no differences in outcomes (OS and DSS) between regions A and B based on the Cox regression models (HR for OS = 1.04 [CI 0.81–1.33], p = 0.78; HR for DSS = 0.86 [CI 0.53–1.38], p = 0.53; Fig. 3A and B). There was no statistically significant difference in DFS (data not included).
(
There were 202 patients treated for recurrence in regions A, and 223 in regions B. However, the differences between regions were not statistically significant for overall recurrence (p = 0.33), thyroid bed recurrence (p = 0.07), or neck recurrence (p = 0.37; Table 4). Similarly, there were no differences in recurrence rates comparing regions A and B for the MSK low-risk cohort or female patients (data not included). Furthermore, there was no difference in OS (p = 0.425) or DSS (p = 0.418) comparing the outcomes of the patients from regions A and B who recurred (data not included).
Females with papillary cancer ≤4 cm (n = 1838)
Females with papillary cancer ≤4 cm represented 58.9% of the overall patient population. When comparing the patients between the treatment regions, there was no statistically significant difference in age, lymph node involvement, or histology, although those from regions A had smaller tumors with more multiple foci. The rate of total thyroidectomy for patients of regions A (68.8%) was significantly greater than that for patients of regions B (52.8%; p < 0.0001), and the rate of adjuvant RAI was significantly greater for the patients of regions A (62.9%) compared to regions B (39.7%; p < 0.0001). The DSS was 98% in both regions.
“Low-risk” patients (n = 1086)
The “low-risk” group represented 34.8% of the overall population. When comparing patients between the treatment regions, there was no statistically significant difference in age, sex, comorbidity, margins, or lymph node involvement. The patients from regions A had more small tumors and more tumors with multiple foci compared to patients from regions B. The rate of total thyroidectomy for patients from regions A (71.1%) was significantly greater than that for patients from regions B (52.1%; p < 0.0001), and the rate of adjuvant RAI was significantly greater for patients from regions A (62.3%) compared to those from regions B (41.8%; p < 0.0001). The 15-year DSS was 99.9%.
Prognostic factors
The variables of age, sex, comorbidity, vascular invasion, extrathyroidal spread, MSK risk strata, and TNM stage were statistically prognostic for both OS and DDS (Fig. 3A and B). The Forest plots highlight that age is the overwhelming risk factor, minimizing others such as sex and angioinvasion. Interestingly, the variables of multiple foci, positive margins, and lymph node involvement (binary variable) had no impact on outcomes. When the various permutations of lymph node involvement (1–2 nodes, 3–5 nodes, >2 nodes, and >5 nodes) were compared to no involved nodes, only the presence of 3–5 involved nodes demonstrated statistical significance for DSS (HR = 2.80 [CI 1.28–6.12]). The statistically significant increased risk for patients with higher comorbidity scores suggests that there was treatment selection bias, and the very high HR estimates for intermediate- and high-risk patients are almost certainly driven by age and sex.
Indications for treatment
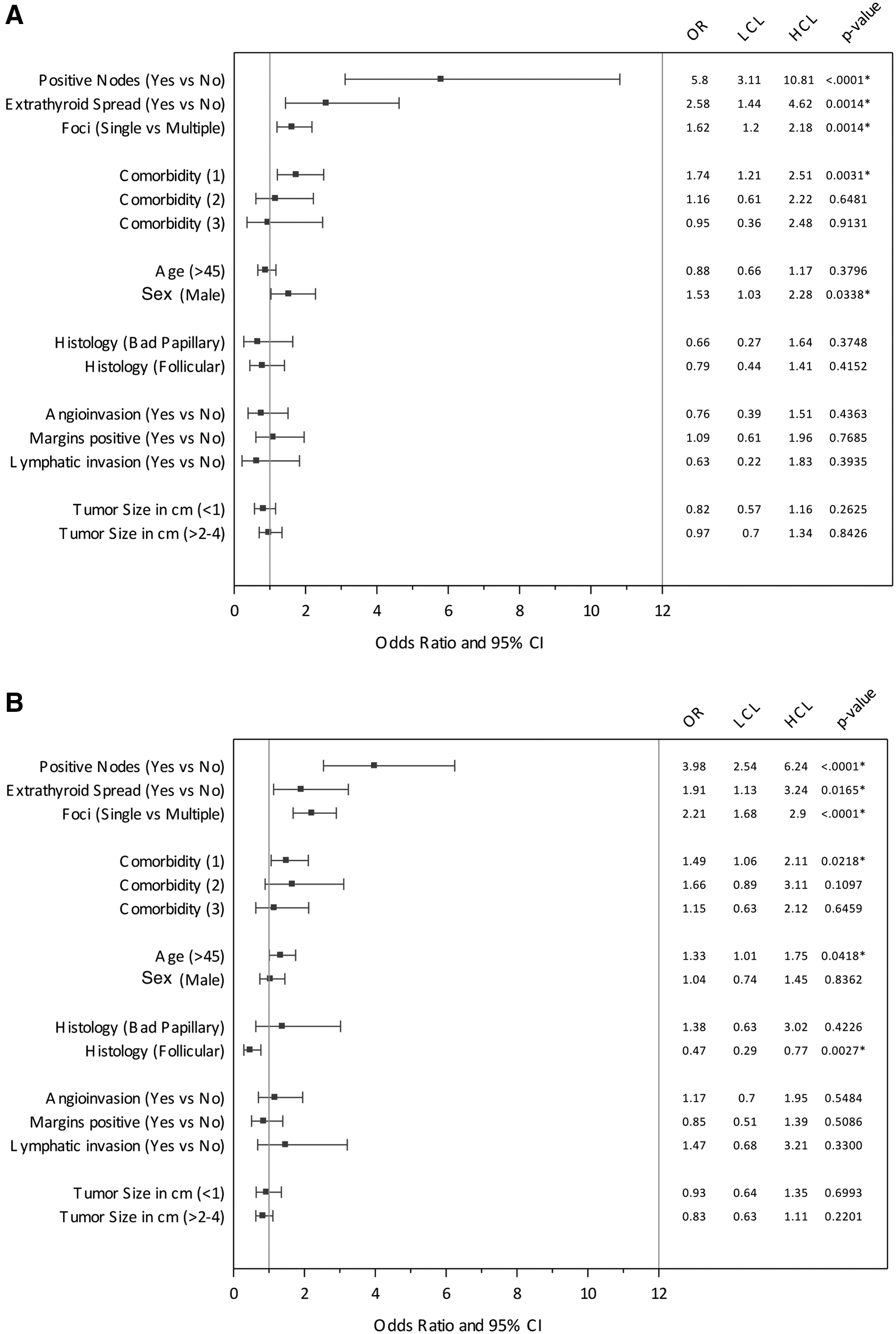
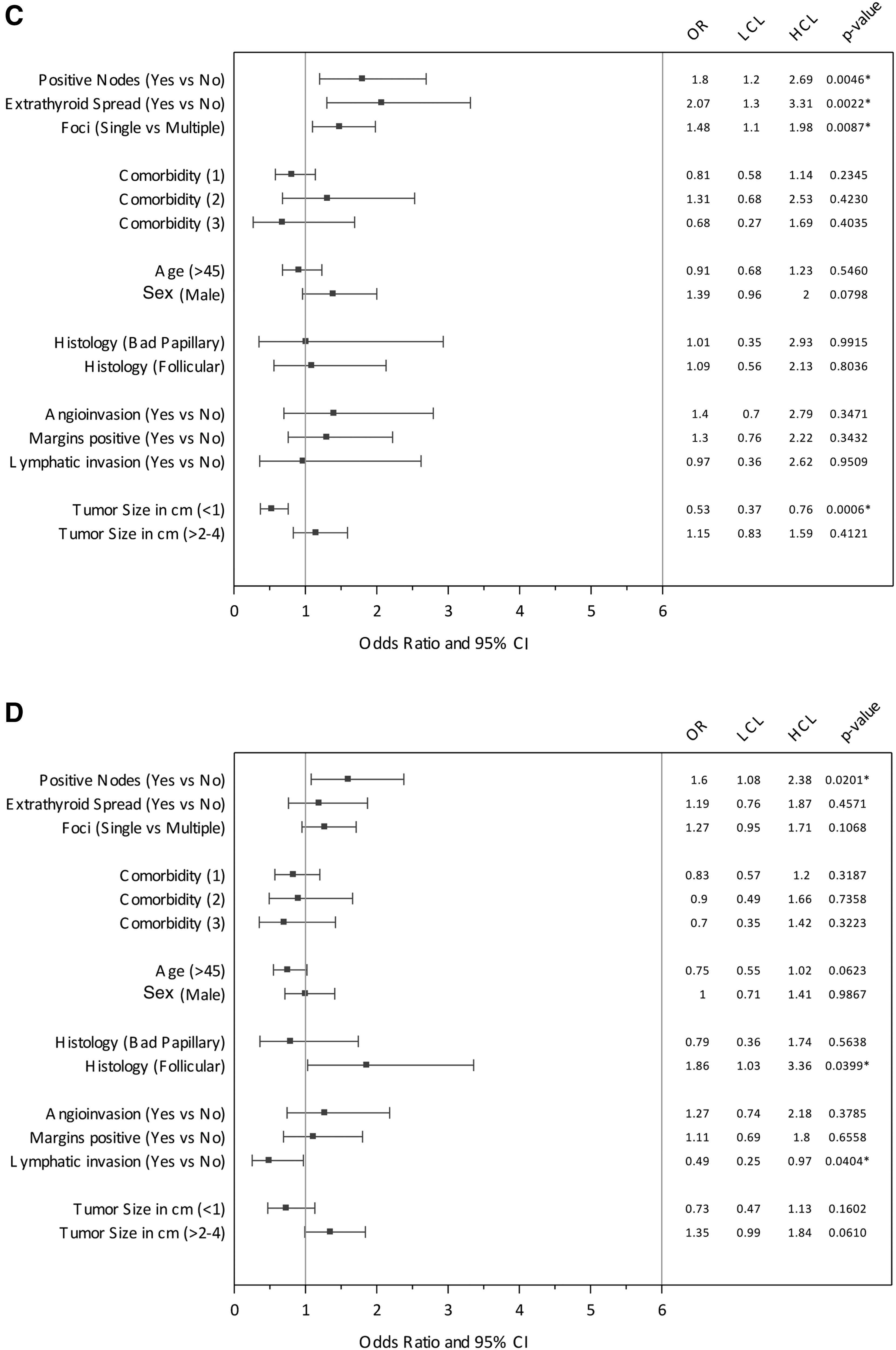
Figure 4A–D reports the patient and tumor factors that independently determined the treatments of total thyroidectomy and RAI for treatment regions A and B. The variables that influenced extent of surgery in both regions were extrathyroidal spread, lymph node involvement, and multifocal disease. Tumor size was not a treatment factor in regions A or B. The only variable that predicted RAI treatment in both regions was the presence of involved lymph nodes. Overall, regions A and B differed in indications for total thyroidectomy and RAI for most variables. Furthermore, the predictors of more extensive treatment often did not match the predictors of outcome, including, in particular, age (relative risk [RR] = 19.9), sex (RR = 2.66), and angioinvasion (RR = 3.09; Fig. 3A and B).
(
Discussion
A total of 7459 patients with DTC in Ontario, Canada, between 1990 and 2002 were identified, and this article reports on both the overall population of 6214 and specific cohorts, including 2444 patients with tumors ≤4 cm, 1838 females with papillary cancer ≤4 cm, and 1086 “low-risk” patients. Only 3% of patients died of their cancer, and if the sample is restricted to the 34.5% of patents with a low-risk designation, this was <1%. No difference was found in the survival or first recurrence outcomes for the patients from regions with more aggressive surgical management compared to those from regions with less aggressive treatments, and no agreement on indications for more aggressive treatment. These findings confirm the work by Sawka et al. (8) and McLeod et al. (9), as well as the findings of Jonklaas et al. (12) and Shaha et al. (15). Shaha et al. (15) reported 99% 20-year survival, regardless of extent of treatment, for 465 patients classified as MSK low risk, and no statistically significant difference in any outcome between total thyroidectomy and lobectomy. The present study found that prognostic factors did not direct the extent of treatment between 1990 and 2001, consistent with the poor evidence and controversy available at that time. The data suggest that lower-risk thyroid cancer was being over-treated, and that the extent of both surgery and the use of RAI could be reduced without affecting outcomes, particularly when the increasing incidence is due to smaller and smaller cancers. These findings are consistent with the latest American Thyroid Association (ATA) guidelines that suggest de-intensification of surgery and RAI for many patients with lower-risk disease (21).
This study design is based on the concept of natural experiments in patient care that occur when physicians in different regions treat the spectrum of typical patients with varying treatments (22,23). The methodology has been reported in head and neck oncology research (24 –27), as well as other cancer sites (28 –31). This study might be considered an example of a comparative effectiveness study (32) using population-based retrospective observational data, except that the comparisons are based on accepted instead of clinical trial–proven treatments for thyroid cancer. In particular, patients who had total thyroidectomy were compared to those who had lobectomy for lower-risk disease. The rationale for the “pre-emptive strike” of total thyroidectomy in this patient group is “knowing the extent of the disease,” eliminating concern over multifocality in the contralateral lobe, ease of follow-up with thyroglobulin, and the avoidance of a second completion thyroidectomy procedure in those patients who are found to have higher-risk disease based on the final pathology. However, the downsides of a total thyroidectomy compared to lobectomy alone include increased hospital costs, increased risk for recurrent laryngeal nerve injury, temporary hypoparathyroidism, permanent hypoparathyroidism, surgical complications of a longer procedure, and a lifetime of balancing hormone replacement. In this study, the extent of surgery did not compromise survival or recurrence, as the group of patients from treatment regions A, where patients had 25% more total thyroidectomies compared those from regions B, had identical outcomes, noting that the patients from regions B were at higher risk.
The risk factors for patients with cancer ≤4 cm were identified to be age >45 years, male, higher comorbidity, unfavorable histology, tumors 2–4 cm, angioinvasion, and extrathyroidal spread, with the major risk factor being age. However, and contrary to both the literature and common practice, factors such as multiple foci, positive margins, and presence of involved lymph nodes were not prognostic factors. Remarkable variation was also found during the study time frame in the indications for the extent of surgery and for the addition of RAI, even for established risk factors such as age (HR = 19.92) and sex (HR = 2.66). Figure 4A and B compares the indications for total thyroidectomy by regions, and there was agreement on extrathyroidal disease, involved nodes, and multiple foci only. Similarly, the data in Figure 4C and D indicate that the presence of involved nodes was an indication for RAI. However, there was no agreement on any other factor comparing treatment regions. Hopefully, as guidelines are accepted more widely by those treating thyroid cancer, variations in treatments will be reduced.
The variations in treatments are consistent with the thyroid cancer literature. For example, Haymart et al. (33) utilized the U.S. National Cancer Database data set that included 189,219 patients with DTC between 1990 and 2008 to study practice patterns for RAI across the United States. They found that the variables associated with increased use of RAI included age, comorbidity (healthier), stage (increasing stage), and increasing hospital case volume, and the variables associated with decreasing use were race/ethnicity (African American), insurance (absence of), and sex (female). They reported that only small proportions of the variance in practice could be explained by age, sex, race, comorbidity, poverty, insurance, education, rurality, stage, case volume, and hospital type. For subsets of patients where the indications might have been clearer (low-risk younger females with small tumors and older males with larger tumors), they found high unexplained variance. They concluded that the “variation demonstrated in both low- and high- risk patients suggests clinical uncertainty” for the indications for RAI, that extent of disease did not correlate with extent of treatment, and that over-treatment was of concern, especially considering the risk of associated toxicity and late side effects.
The strengths of this study include the long follow-up on a complete cohort of non-selected patients, the quality of the pathology report data abstraction (two trained tumor abstractors reviewed all 6746 pathology reports), the quality of the electronic patient information data available in Ontario, and the inclusion of recurrence along with survival outcomes. Furthermore, the results are generalizable, as Ontario has a strong comprehensive cancer program, the evidence in thyroid cancer is weak, and treatment is known to vary in many jurisdictions. The findings are consistent with the literature on over-diagnosis and the potential over-treatment of cancers (34 –39) and specifically thyroid cancer (4,40 –44).
The study has eight potential weaknesses. The assessment of outcomes in thyroid cancer is often criticized due to insufficient follow-up time, but in order to have 15 years of follow-up, a study has to rely on information from eras with different standards of reporting, different staging systems, different treatments, and different follow-up methods. For example, the quality of the pathology reports varied considerably over the time period and by hospital. Occasionally, basic information such as tumor size was missing, and almost certainly the numbers of patients with poorer histological features when it was not reported have been underestimated. There is, however, no reason to suspect that the rate of missing data would vary between regions A and B, and if present, the rates would be very low. Using older data is problematic, as treatment philosophies have changed since 2000. The second potential weakness is the lack of M category data. Although the low-risk classification may not be completely accurate, there is no reason to think that the very low rate of distant disease would be vary between regions A and B in this group of lower-risk patients. The third potential weakness is that microscopic nodal disease was not abstracted separately from gross involvement. The fourth potential weakness is that unknown confounders or differences in patients between regions A and B that are not available in the registry data or electronic health records cannot be accounted for. For example, there is no information on the use of or compliance with oral thyroid hormone suppression in patients after lobectomy only. Fifth, the reasons for first subsequent treatments (the surrogate for first recurrence) are not known. The data on thyroid bed and neck recurrences are accurate, as surgery would only be indicated in the case of recurrence, but those who underwent RAI may not reflect true recurrences. Sixth, due to excellent survival in patients with well-differentiated thyroid cancer, there are not enough survival events, despite 2444 cases, to be statistically confident of some prognostic factors. This is a common limitation of studies on thyroid cancer. Seventh, treatment complications were not included. Ideally, rates of surgical complications such as vocal cord paralysis or hypocalcemia or RAI complications such as sialadenitis would have been compared. However, the recorded diagnosis codes for office consultation billing are not sufficiently reliable in the Ontario Health Insurance Plan data set. Finally, the study relied on administrative data to estimate cause of death and DSS, and may have underestimated a major outcome, noting that OS may be more reflective of comorbid illness in this patient population.
Conclusion
In Ontario, Canada, there was significant variation in treatment, little agreement on indications for treatment, and no difference in outcomes when comparing regions with very different treatment philosophies between 1990 and 2001. The results of this population-based study are consistent with uncertainty about the evidence at the time and the potential for over-treatment in the management of lower-risk thyroid cancer. Many patients could have been managed with less treatment such as hemithyroidectomy alone and without RAI, as the risks of over-treatment may outweigh the potential gains. Further research in this evidence-to-practice gap is required to identify barriers and enablers in order to address overly aggressive treatment in patients with lower-risk thyroid cancer.
Footnotes
Acknowledgments
Funding was provided from the Canadian Institutes of Health Research MOP # 84356 (Controversy in the management of differentiated thyroid cancer). The original CIHR co-investigators included Drs. W. Kent, R. George, W. Shelley, A. Driedger, D. Feldman-Stewart, R. Houlden, P. Isatalo, S. Archibald, P. Peng, and G.R. Walker. Ethics approval was obtained from the Ethics Review Board of Queen's University (OTOL 029-06). The study coordinator was Susan Rohland with assistance from Sarah Pickett. Dr. D. Hurlbut advised on the pathology abstraction. The Site PIs included Drs. P. O'Dell (University of Ottawa), S. Archibald (McMaster University), J. Yoo (University of Western Ontario), and K. Higgins (Sunnybrook Health Sciences Center).
The Institute of Clinical and Evaluative Sciences is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. The project analysis was approved by the ICES Cancer Program, and the analysis was conducted at ICES@Queens. The opinions, results, and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario Ministry of Health and Long-Term Care is intended or should be inferred.
ICES is a prescribed entity under the Ontario Personal Health Information Protection Act. As such, ICES policies and procedures are approved by Ontario's Information and Privacy Commissioner. These policies require that access to data be limited to persons who require such access to perform their role on an approved ICES project or third-party project. Thus, we are prohibited from making ICES data publicly available. Only the results of analysis of ICES data may be made available.
Data management was undertaken by Amy Schneeburg and Dianna Martins at Division of Cancer Care and Epidemiology of the Queen's Cancer Research Institute and by Rebecca Griffiths and Marlo Whitehead at ICES@Queens. Melanie Walker, PhD, kindly reviewed the manuscript. We acknowledge the Ontario Cancer Registry and Cancer Care Ontario for providing us with the Ontario Cancer Registry data used in this report, as well as the assistance of IntelliHealth Ontario.
This article was presented at the Canadian Otolaryngology Society (June 2014) and at Preventing Overdiagnosis (September 2014).
Author Disclosure Statement
The authors have no conflicts of interest and no competing financial interests exist.