
Abstract
Background:
This study aimed to explore the relation of immunoglobulin G4 (IgG4) to clinical and laboratory characteristics of patients newly diagnosed with Graves' disease (GD) without or with Graves' ophthalmopathy (GO) and to analyze association of IgG4 with development and grade of GO in GD patients.
Methods:
Sixty-four GD patients and 64 sex- and age-matched euthyroid subjects were enrolled. Serum levels of thyroid hormones, thyroid autoantibodies, immunoglobulin G (IgG), and IgG4 were measured, and ophthalmological and ultrasonographical evaluation was performed.
Results:
In GD patients compared with euthyroid subjects, levels of thyroid hormones, thyroid autoantibodies and IgG4 as well as the IgG4/IgG ratio were elevated. GD patients having GO in comparison to not having GO were characterized by a female predominance; a high incidence of smoking history; high levels of T3, free T4, TSH receptor autoantibody (TRAb) and IgG4; and a high IgG4/IgG ratio after adjusting for sex. In GD patients, the IgG4 level was the independent factor associated with GO development on multivariate analysis. When severity and activity of GO were classified using the European Group on Graves' Orbitopathy criteria in GD patients with GO, IgG4 levels and IgG4/IgG ratio were elevated in the moderate-to-severe group compared with the mild group and in the active group compared with the inactive group. IgG4 levels and IgG4/IgG ratio became elevated as clinical activity score increased. IgG4 levels were positively correlated with TRAb levels. The high IgG4 group in comparison to the normal IgG4 group had a high incidence of family history of autoimmune thyroid disease, high levels of free T4, TRAb and IgG4, a high IgG4/IgG ratio and extensive hypoechogenicity.
Conclusions:
These results suggest that IgG4 levels are elevated in newly diagnosed GD patients compared with euthyroid subjects and in the presence of GO compared with the absence of GO. Moreover, our findings suggest that IgG4 levels are associated with the development and grade of GO in GD patients.
Introduction
G
Graves' ophthalmopathy (GO) is a common extrathyroidal manifestation of GD affecting 25–50% of GD patients to various extents (3 –5). In the pathogenesis of GO, orbital adipocytes and fibroblasts release proinflammatory cytokines augmenting TRAb production by orbital plasma cells (6,7). As a result, TRAb activate TSH receptors expressed in orbital tissues, and GO develops (6,7).
Immunoglobulin G4 (IgG4)–related disease (IgG4-RD) is defined by elevated IgG4 levels, and at the level of the thyroid it shows pathological features such as dense lymphoplasmacytic infiltration in a storiform pattern, increased numbers of IgG4-positive plasma cells, mild-to-moderate eosinophilic infiltration, obliterative phlebitis, and fibrosis (8,9). Since sclerosing pancreatitis was reported to be an IgG4-RD, Mikulicz's syndrome, periaortitis, peirarteritis, retroperitoneal fibrosis, sclerosing cholangitis, and tubulointersitial nephritis have also been revealed to be IgG4-RD (8 –10). With respect to IgG4-RD of the thyroid gland, it was shown that IgG4-RD patients with hypothyroidism had an enlarged thyroid volume, and elevated levels of thyroglobulin autoantibodies (TgAb) and thyroid peroxidase autoantibodies (TPOAb) (11). Moreover, it has been proposed that some groups of autoimmune thyroid diseases (AITD) including Hashimoto's thyroiditis and Riedel's thyroiditis are IgG4-RD (12 –18). It has been reported that Hashimoto's thyroiditis can be divided into two distinct subtypes as IgG4 thyroiditis and non-IgG4 thyroiditis based on histopathological findings: IgG4 thyroiditis correlated with male sex, high levels of thyroid autoantibodies, low echogenicity, and rapid progression to hypothyroidism (12,13).
In terms of the relationship between GD and IgG4-RD, it was shown that GD patients with high IgG4 levels presented clinical and ultrasonographical features associated with old age, increases in hypoechoic areas, and good response to antithyroid drugs, and IgG4 levels were high in GD patients having GO in comparison with not having GO (19 –21). Furthermore, GD patients who underwent thyroidectomy were reported to display marked stromal fibrosis with diffuse lymphoplasmacytic infiltration in the thyroid gland (22). Although the link between IgG4-RD and both GD-dependent and GD-independent ophthalmopathy has been assumed (23 –26), the clinical significance of IgG4 in GD patients without or with GO has not yet been fully investigated.
In the present study, we evaluated the relevance of IgG4 to clinical and laboratory characteristics of newly diagnosed GD patients without or with GO and examined possible associations of IgG4 with development and grade of GO in GD patients.
Subjects and Methods
Subjects
This case-control study was performed on subjects who visited or were referred to the Endocrinology and Metabolism Outpatient Clinic of the Hallym University Sacred Heart Hospital, Republic of Korea, from January 2013 to August 2015. The control group was composed of sex- and age-matched euthyroid subjects who did not have any thyroid disease history. Patients were enrolled at the initial diagnosis of GD, and thus none of the patients underwent antithyroid drug or radioactive iodine therapy or surgery at the time of enrollment. The diagnosis of GD was based on the presence of hyperthyroidism, positive TRAb and increased 131I uptake without hot nodule in the thyroid gland. GD patients were divided into two groups depending on the presence of GO on the basis of NOSPECS (no signs or symptoms, only signs, soft tissue, proptosis, extraocular muscle, cornea, sight loss) and clinical activity score (CAS). GD patients with no signs or symptoms (NOSPECS grade 0) were assessed as no GO. Euthyroid subjects and GD patients were analyzed for sex, age, familial history of AITD, and smoking history. Also, serum levels of thyroid hormones, thyroid autoantibodies, IgG, and IgG4 were measured, and ophthalmological and ultrasonographical evaluation was performed. Exclusion criteria of the study were as follows: (i) liver and/or kidney dysfunction, (ii) steroid or immunosuppressive agent use within the last six months, (iii) pregnancy, (iv) active infection, (v) history of allergy, (vi) history of malignancy, (vii) patients with any kind of immunodeficiency disorder, and (viii) evidence of any unresolved medical problem that can affect IgG4 levels like fever of unknown origin or weight loss. The study protocol was approved by the Hallym University Sacred Heart Hospital Institutional Review Board and Ethics Committee.
Measurement of serum thyroid hormones and thyroid autoantibodies
Serum levels of triiodothyronine (T3), free thyroxine (T4), TSH, TRAb, TgAb, and TPOAb were measured by an electrochemiluminescent immunoassay (Roche, Rotkreuz, Switzerland). Reference ranges were defined as follows: T3, 80–200 ng/dL; free T4, 0.9–1.7 ng/dL; TSH, 0.27–5.0 mIU/L; TRAb, <1.75 IU/L; TgAb, <115 IU/mL; TPOAb, <34 IU/mL.
Measurement of serum IgG and IgG4
Serum levels of immunoglobulin G (IgG) and IgG4 were measured by a turbidimetric assay (Toshiba, Tochigi-ken, Japan). Reference ranges for IgG and IgG4 were defined as 680–1620 mg/dL and 3.9–86.4 mg/dL, respectively.
Ophthalmological evaluation
The severity of GO was rated as mild, moderate-to-severe and sight-threatening using the European Group on Graves' Orbitopathy (EUGOGO) criteria (4,27). Independently of severity, activity of GO was assessed by the sum of CAS based on seven items (spontaneous retrobulbar pain, pain on attempted upward or downward gaze, redness of eyelids, redness of conjunctiva, swelling of caruncle or plica, swelling of eyelids, and swelling of the conjunctivae) (4,27). When CAS was three or more, GO was considered to be active (4,27).
Ultrasonographical evaluation
Ultrasonographical analysis was performed with a 10 MHz linear transducer (Phillips Healthcare, Amsterdam, The Netherlands) in mode of conventional gray scale and color Doppler. Hypoechogenicity was graded as follows: 0, absent; 1, mild when compared with the normal thyroid parenchyma assessed in the same conditions; 2, well recognizable when compared with the normal thyroid parenchyma assessed in the same conditions; 3, comparable with echostructure of the neck strap muscle (Supplementary Fig. S1; Supplementary Data are available online at
Statistical analysis
All data are expressed as mean ± standard deviation. Fisher's exact test or chi-squared test were used to compare data in the two-dimensional contingency tables for sex, age, family history of AITD, and smoking history in two or three individual groups, respectively. Mann-Whitney U-test or Kruskal-Wallis test were used to compare data in two or three individual groups, respectively. Two-tailed Spearman's rank correlation analysis was used to evaluate correlation between two variables. Multivariate logistic regression analysis was used to estimate the influence of variables on GO development in GD patients. Sample size for Mann-Whitney test was determined using power analysis. The power analysis was conducted in G-POWER program version 3.1 using an alpha of 0.05, a power of 0.80 and a medium effect size of 0.5 for a two-tailed test. Based on the aforementioned assumptions, the required sample size was 67. A p-value less than 0.05 was considered to be statistically significant. All analyses were performed using SPSS program version 24.0 (SPSS, Chicago, IL).
Results
Baseline characteristics of control subjects and GD patients
We enrolled 64 treatment-naive GD patients to the GD group and 64 sex- and age-matched euthyroid subjects to the control group. The baseline characteristics of the two groups are summarized in Table 1.
Data are presented as mean ± SD unless otherwise indicated.
p < 0.05.
AITD, autoimmune thyroid disease; GD, Graves' disease; IgG, immunoglobulin G; IgG4, immunoglobulin G4; T3, triiodothyronine; T4, thyroxine; TgAb, thyroglobulin autoantibody; TPOAb, thyroid peroxidase autoantibody; TRAb, thyrotropin receptor autoantibody; TSH, thyrotropin.
In the GD group compared with the control group, family history of AITD and smoking history did not differ, while levels of T3, free T4, TRAb, TgAb, and TPOAb were elevated, and TSH levels were reduced. No difference in IgG levels between the two groups was found. IgG4 levels were normal in all subjects of the control group, whereas these were elevated in 6 of 64 patients (9.4%) of the GD group. Moreover, IgG4 levels (control vs. GD, 25.2 ± 12.4 vs. 42.0 ± 25.9 mg/dL, p < 0.001) and IgG4/IgG ratio (control vs. GD, 2.2 ± 1.0 vs. 3.3 ± 1.9%, p < 0.001) were elevated in the GD group in comparison to the control group. No euthyroid subject or GD patient had any other IgG4-RD.
On ultrasonographical examination, the thyroid gland was enlarged, and prominent hypoechogenicity and CDF were evident in the GD group compared with the control group.
Comparison of clinical and laboratory parameters between GD patients without and with GO
GD patients were divided into two groups based on the presence (GO+) or absence (GO−) of GO (Table 2). Twenty-two GD patients (34.4%) were diagnosed with GO on the basis of NOSPECS and CAS. Among GD patients with elevated IgG4 levels, 6 patients had GO. The GO+ group exhibited female predominance and high smoking history in comparison to the GO− group. In contrast, age and family history of AITD between the two groups were not different.
Data are presented as mean ± SD unless otherwise indicated.
p < 0.05.
GO, Graves' ophthalmopathy.
In the GO+ group compared with the GO− group, levels of IgG (GO− vs. GO+, 1194.5 ± 175.1 vs. 1500.5 ± 429.2 mg/dL, p = 0.022) and IgG4 (GO− vs. GO+, 28.9 ± 13.7 vs. 66.9 ± 25.4 mg/dL, p < 0.001; Fig. 1), and IgG4/IgG ratio (GO− vs. GO+, 2.5 ± 1.3 vs. 4.7 ± 1.9%, p < 0.001) increased. Levels of T3, free T4, TRAb, and TgAb of the GO+ group were higher than those in the GO− group. The groups did not differ in levels of TSH and TPOAb, thyroid volume, hypoechogenicity, and CDF.

Comparison of immunoglobulin 4 (IgG4) levels of Graves' disease patients without and with Graves' ophthalmopathy (GO).
As females were more prevalent in the GO+ group than in the GO− group, the data were stratified by sex, and association between the dichotomized variables and the presence of GO was estimated in a general linear model using the Cochran-Mantel-Haenszel test. The statistical significance (adjusted p-value) of differences in variables, except levels of IgG and TgAb, and hypoechogenicity, remained after adjusting for sex.
Factors associated with GO development in GD patients
To identify factors associated with GO development in GD patients, we performed a multivariate analysis using only those factors that were significant on univariate analysis (Table 3). On univariate analysis, female sex (p = 0.019), smoking history (p = 0.016), and levels of IgG (p = 0.012), IgG4 (p < 0.001), T3 (p = 0.007), free T4 (p = 0.012), TRAb (p < 0.001) and TgAb (p = 0.016) were significantly associated with GO development in GD patients. After adjusting for other significant factors in multivariate analysis, the IgG4 level was the independent factor associated with GO development in GD patients, with p = 0.046, odds ratio (OR) = 1.351 [95% confidence interval = 1.006–1.815].
Statistically significant values are in bold.
CI, 95% confidence interval; OR, odds ratio.
Analysis of GD patients with GO according to clinical assessment of GO
In GD patients with GO, severity of GO was assessed in 14 patients as mild severity and in 8 patients as moderate-to-severe severity (Table 4). No patient had sight-threatening severity. Sex, age, family history of AITD, and smoking history of two groups were not different. IgG levels in the moderate-to-severe group did not differ from those in the mild group. By contrast, IgG4 levels (mild vs. moderate-to-severe, 52.8 ± 17.0 vs. 91.4 ± 17.6 mg/dL, p = 0.001; Fig. 2) and IgG4/IgG ratio (mild vs. moderate-to-severe, 3.8 ± 1.5 vs. 6.2 ± 1.6%, p = 0.006) were elevated in the moderate-to-severe group in comparison with the mild group. While levels of TSH, TRAb, TgAb and TPOAb, thyroid volume and CDF did not differ in the two groups, levels of T3 and free T4, and hypoechogenicity in the moderate-to-severe group were higher than those in the mild group.
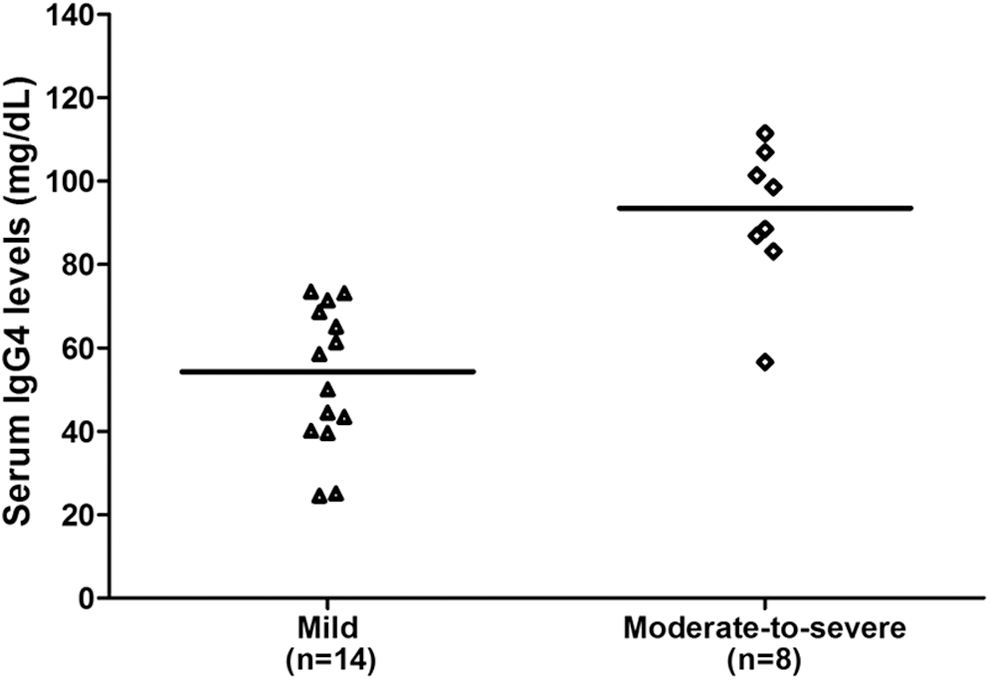
Comparison of IgG4 levels according to severity of GO in Graves' disease patients.
Data are presented as mean ± SD unless otherwise indicated.
p < 0.05.
GD patients with GO were classified into inactive (n = 16) and active (n = 6) ophthalmopathy groups (Table 5). Sex, age, family history of AITD, and smoking history were not different between the two groups. IgG levels between the two groups did not differ, whereas IgG4 levels (inactive vs. active, 56.8 ± 19.3 vs. 93.9 ± 19.9 mg/dL, p = 0.004; Fig. 3) and IgG4/IgG ratio (inactive vs. active, 4.2 ± 1.9 vs. 6.0 ± 1.5%, p = 0.033) were elevated in the active group compared with the inactive group. There was no difference in levels of TSH, TgAb and TPOAb, thyroid volume, hypoechogenicity, and CDF between the two groups. In contrast, levels of T3, free T4, and TRAb of the active group were higher than those of the inactive group.
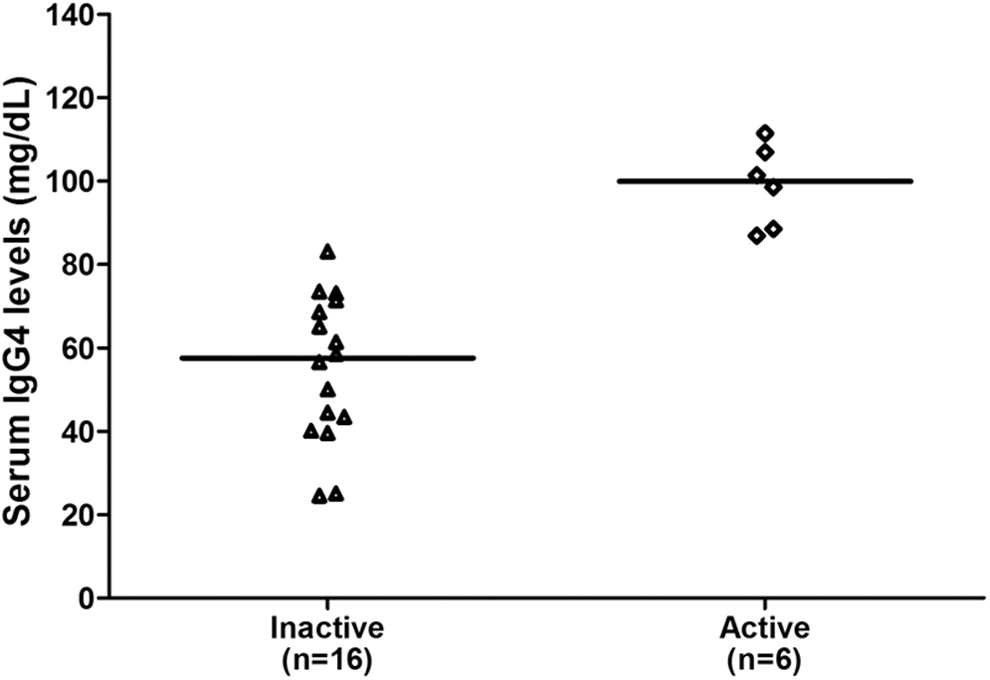
Comparison of IgG4 levels according to activity of GO in Graves' disease patients.
Data are presented as mean ± SD.
p < 0.05.
When GD patients with GO were divided by individual CAS status, 10 (45.4%), 6 (27.3%), and 6 (27.3%) patients were allocated to the CAS1, CAS2, and CAS3 groups, respectively (Table 5). Although sex, age, and smoking history were not different among the three groups, family history of AITD was higher in the CAS2 and CAS3 groups than in the CAS1 group. IgG levels tended to be elevated as a function of advancement in CAS. In addition, IgG4 levels (CAS1 vs. CAS2 vs. CAS3, 46.5 ± 15.9 vs. 74.1 ± 9.4 vs. 93.9 ± 19.9 mg/dL, p = 0.001) and IgG4/IgG ratio (CAS1 vs. CAS2 vs. CAS3, 3.6 ± 1.6 vs. 5.3 ± 2.0 vs. 6.0 ± 1.5%, p = 0.033) were elevated in ascending order of CAS. A higher CAS was related to higher levels of T3 and free T4, but not of TSH. Furthermore, TRAb levels were the highest in the CAS3 group, and TgAb levels were the highest in the CAS2 group. The three groups did not differ regarding TPOAb levels, thyroid volume, hypoechogenicity and CDF.
Analysis of GD patients with GO according to IgG4 levels
GD patients with GO were classified into two groups: those with normal and those with high IgG4 levels (Table 6). In the latter group in comparison to the former group, family history of AITD increased, while no difference in sex, age, and smoking history was observed between the two groups. In terms of the laboratory parameters, levels of IgG4 (normal IgG4 vs. high IgG4, 54.9 ± 17.5 vs. 98.9 ± 9.8 mg/dL, p < 0.001), free T4 and TRAb, IgG4/IgG ratio (normal IgG4 vs. high IgG4, 4.2 ± 1.9 vs. 6.1 ± 1.3%, p = 0.021) and hypoechogenicity increased in the high IgG4 group compared with the normal IgG4 group. However, levels of IgG, T3, TSH, TgAb and TPOAb, thyroid volume, and CDF were not different between the two groups.
Data are presented as mean ± SD.
p < 0.05.
Correlation of IgG4 levels with clinical and laboratory parameters in GD patients with GO
In GD patients with GO, correlation of IgG4 levels with clinical and laboratory variables was investigated (Table 7). IgG4 levels were positively correlated with TRAb levels (r = 0.462, p = 0.031), but not with age and levels of IgG, thyroid hormones, TgAb, and TPOAb.
p < 0.05.
Discussion
In the present study, our results demonstrate that IgG4 levels and IgG4/IgG ratio increase in GD patients compared with euthyroid subjects and in GD patients having GO in comparison with not having GO. Furthermore, these findings indicate for the first time that IgG4 levels are associated with the development and grade of GO in GD patients.
In terms of the clinical relationship between IgG4-RD and AITD, IgG4 levels are elevated in patients with the fibrous variant of Hashimoto's thyroiditis and with Riedel's thyroiditis (12 –18). The pathophysiological relevance of IgG4-RD to thyroid disorders is illustrated by the observation that IgG4 levels fall after thyroidectomy in patients with IgG4 subtype Hashimoto's thyroiditis producing IgG4 in response to antigen(s) derived from the thyroid gland (28). In GD, it was shown that patients have high IgG4 levels and large thyroid volumes compared with control subjects (21). In the present study, GD patients exhibited a pathognomonic elevation of levels of thyroid hormones and thyroid autoantibodies in comparison to euthyroid controls. All euthyroid subjects had normal IgG4 levels, whereas 9.4% of GD patients had high IgG4 levels. Compared with euthyroid subjects, GD patients displayed thyroid enlargement, prominent hypoechogenicity, and profound vascularity. Collectively, our results suggest that IgG4 may play a crucial role in the development of GD similar to its role in IgG4 thyroiditis. However, we have no histopathological data on GD patients, and the possible relationship between GD and IgG4-RD should be further studied.
In view of cut-off IgG4 levels, earlier studies used different values to distinguish high IgG4 (or elevated IgG4) groups from normal IgG4 (or nonelevated IgG4) groups in control subjects and GD patients (19 –21). Takeshima et al. used a nephelometric immunoassay to measure IgG4 levels with reference values of 4∼108 mg/dL (19). In their study, instead of analyzing a control group, virtual control subjects were supposed to have an IgG4 level of 43 mg/dL, which was the mean estimate based on the data (n = 21) reported by Yamamoto et al. (29). They classified GD patients with an IgG4 level above 135 mg/dL, and fulfilling comprehensive diagnostic criteria for IgG4-RD (30), into an elevated IgG4 group. Bozkirli et al. measured IgG4 levels nephelometrically but did not give a reference value (20). The control group had a mean IgG4 level of 28 mg/dL. They also used an IgG4 level of 135 mg/dL as the cutoff point for defining an elevated IgG4 group among GD patients. Martin et al. measured IgG4 levels via an enzyme immunoassay with reference values of 3.1∼328.9 mg/dL (21). There was no real control group, and a mean IgG4 level provided by the manufacturer was 107.4 mg/dL (n = 20). They divided GD patients into two groups by quartile exploration of the 75th (237.52 mg/dL) and the 90th (286.28 mg/dL) percentiles. In the present study, we measured IgG4 levels using a turbidimetric assay, and employed reference values of 3.9–86.4 mg/dL. GD patients with GO having IgG4 levels higher than the upper limit (16/22) were assigned to the high IgG4 group, which placed them above the 73rd percentile.
Although it has been proposed that various genetic and environmental factors including female sex, smoking, stress, and TRAb are risk factors for GO development in GD patients, controversy still remains (5,7). In regard to IgG4 status of GD patients, it has been shown previously that GO is relevant to increases in IgG4 levels (20), but the question of whether IgG4 level was a factor associated with GO development has not been investigated. In the present study, the GO+ group in comparison to the GO− group was characterized by a female preponderance, a high incidence of smoking history, and high levels of T3, free T4, TRAb, and TgAb. However, levels of TSH and TPOAb were similar in two groups. Intriguingly, the GO+ group had high levels of IgG and IgG4, and a high IgG4/IgG ratio compared with the GO− group. As sex distribution between the GO+ and GO− groups differed, we performed a stratified analysis under adjustment for sex: the statistical significance of differences in variables, except levels of IgG and TgAb, and hypoechogenicity, was not changed. Moreover, since it was possible that high IgG4 levels in the GO+ group were attributable to severe hyperthyroidism, we performed a multivariate analysis using those factors that were significant on univariate analysis to identify factors associated with GO development. On univariate analysis, female sex, smoking history, and levels of IgG, IgG4, T3, free T4, TRAb, and TgAb were significantly associated with GO development. However, after adjusting for other significant factors on multivariate analysis, IgG4 level was the independent factor associated with GO development. In summary, our results suggest that IgG4 level may be associated with GO development, and high IgG4 levels may aid to select patients at risk for developing GO. Further prospective studies are required to elucidate whether IgG4 levels reliably predicts GO development and to evaluate the IgG4 threshold for detection of patients at high risk of GO.
With respect to the relation of IgG4 levels to GO grade, a previous study reported that IgG4 levels in CAS2 patients were higher than those in CAS3 patients, suggesting that IgG4 levels are not relevant to CAS status (20). However, no relationship between IgG4 levels and severity and activity of GO has yet been determined. In the present study, we classified severity and activity of GO using the EUGOGO criteria, and analyzed clinical and laboratory parameters. As for GO severity, IgG4 levels and IgG4/IgG ratio, but not IgG levels, were elevated in the moderate-to-severe group compared with the mild group. In addition, levels of T3 and free T4, but not of TSH and thyroid autoantibodies, were higher in the moderate-to-severe group than in the mild group. As for GO activity, levels of IgG4, T3, free T4 and TRAb, and IgG4/IgG ratio were elevated in the active group in comparison to the inactive group. Our analysis of clinical and laboratory parameters by individual CAS status showed that a higher CAS score was associated with higher IgG4 levels and a higher IgG4/IgG ratio. When CAS status became elevated, family history of AITD became more prevalent, and levels of T3 and free T4 rose. TRAb levels were the highest in the CAS3 group, while TgAb levels were the highest in the CAS2 group. In contrast, TPOAb levels were not different among the CAS groups. Taken together, our results suggest that IgG4 levels may be associated with severity and activity of GO. Furthermore, these findings suggest that measurement of IgG4 levels may be helpful to manage GO because classification of GO facilitates selection of the most appropriate treatment. Intriguingly, our results differ from the data of the previous study, in that our findings suggest an association of IgG4 levels with individual CAS status (20). This may be explained by the fact that our patients were treatment-naive, whereas some patients in the previous study had undergone thyroidectomy and were receiving levothyroxine replacement therapy.
In GD, it was reported that IgG4 levels increased in a proportion of patients, and patients with high IgG4 levels were characterized by old age, extensive hypoechoic areas, and excellent responsiveness to antithyroid drugs (19). However, contradictory results in younger GD patients with high IgG4 levels receiving high doses of antithyroid drugs have been shown as well (21). In the present study, when GD patients with GO were divided into two groups by IgG4 levels, the high IgG4 group had a high incidence of family history of AITD, and high levels of free T4 and TRAb compared with the normal IgG4 group. Moreover, the percentage of male patients in the high IgG4 group was higher than in the normal IgG4 group (33.3% vs. 0%) although the difference was not significant. In this context, IgG4-RD especially involving the pancreas, kidney, and retroperitoneum is more common in males, which contrasts with other autoimmune diseases that are more common in females (8). The high IgG4 group tended to have higher TgAb levels, suggesting that TgAb may be a possible source of IgG4. In terms of the relationship between IgG4 and TgAb, it was reported that IgG4 was the dominant TgAb subtype in GD patients, and GD patients with both GO and TgAb expression presented a shift toward IgG4 TgAb (31,32). In view of ultrasonographical findings, the high IgG4 group in comparison to the normal IgG4 group showed extensive hypoechogenicity and relatively small thyroid glands. As lesions infiltrated by lymphocytes and plasma cells can be hypoechoic (8), it is likely that dense lymphoplasmacytic infiltration may be associated with IgG4 release and destructive shrinkage of the thyroid gland.
In regard to IgG subclasses expressed by GD patients, it was reported that TRAb are limited to IgG1, and the restriction of heterogeneity reflected IgG oligoclonality (33,34). However, Latrofa et al. later showed that TRAb synthesis was skewed away from IgG1 toward the other IgG subclasses, particularly IgG2 and IgG3, diametrically opposed to the previous results of IgG1 restriction (35). In addition, they found that TRAb consisted predominantly of IgG4 and IgG1 (35). Based on direct analysis of IgG subclass distribution in highly enriched TRAb preparations, they concluded that TRAb of GD patients was not necessarily restricted to IgG1 (35). In the present study, in GD patients with GO, IgG4 levels correlated with TRAb levels, demonstrating the presence of stimulatory TSH receptor antibodies in the IgG4 fraction. TRAb levels have been reported to correlate with CAS and proptosis in GD patients with GO, but not with disease duration and TPOAb levels (36). Furthermore, serial measurements of TRAb levels were useful to predict the course of GO in about half of all GD patients (37). Thus, our results provide additional evidence for the hypothesis that IgG4 alone or in combination with TRAb may play a pivotal role in development and progression of GO.
In contrast to the previous study conducted by Bozkirli et al. (20), our study included results for family history of AITD, smoking history, levels of IgG and thyroid autoantibodies including TRAb, IgG4/IgG ratio, and ultrasonographical findings including hypoechogenicity and CDF. Moreover, our study suggests that IgG4 levels correlate with TRAb levels, and are relevant to severity and activity of GO. Most importantly, our study indicates for the first time that IgG4 levels are an independent factor associated with GO development.
There are several limitations in our study. First, we did not fully examine alterations in IgG4 levels during and after GD treatment. Second, we had no histopathological data for IgG4 expression and lymphoplasmacytic infiltration in the thyroid gland since our patients did not undergo surgery. Third, we did not measure TSH receptor stimulating immunoglobulin level because the National Healthcare Insurance System of Korea does not fund this expensive test. Forth, we included only patients who visited or were referred to a single university hospital, which may have introduced selection bias.
In conclusion, our results suggest that IgG4 levels are elevated in newly diagnosed GD patients compared with euthyroid subjects and in the presence of GO compared with the absence of GO. In addition, these findings suggest that the IgG4 levels are associated with the development and grade of GO in GD patients. Further studies should focus on changes in IgG4 levels during and after treatment to validate the clinical significance of IgG4 in GD patients with GO.
Footnotes
Acknowledgments
The authors thank all patients as well their families and caregivers for providing clinical data for this study.
This study was presented as poster (#EP976) in the 18th European Congress of Endocrinology, May 28–30, 2016, Munich, Germany.
Author Disclosure Statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.