
Abstract
Background:
While screening of thyroid peroxidase antibody (TPOAb) has been recommended in women with primary ovarian insufficiency, the relationship between thyroid autoimmunity (TAI) and ovarian reserve remains undetermined. Because the TAI prevalence was reported to be different between different ethnic/racial groups, this study aimed to investigate the TAI prevalence in Chinese women with variable ovarian reserve.
Methods:
This is a cross-sectional study conducted in a university infertility clinic between October 2013 and March 2016. Among patients at their first entry to the infertility clinic, a total of 1044 patients with available results of anti-Müllerian hormone (AMH), thyrotropin (TSH), TPOAb, and thyroglobulin antibody (TgAb) were enrolled. The TSH levels and the prevalence of positive TPOAb and positive TgAb were compared between patients with low, normal, and high ovarian reserve categorized with age-specific AMH levels.
Results:
For the whole study population, the TSH levels, TPOAb positivity, and TgAb positivity were comparable between patients with variable ovarian reserve. However, after patients with known causes compromising ovarian reserve (iatrogenic or genetic) were excluded, only TPOAb positivity became significantly different between patients with low (22.7%), normal (14.0%), and high ovarian reserve (10.3%; p = 0.012). The TPOAb levels were not significantly correlated to AMH levels (Spearman's ρ = −0.027; p = 0.413). For the infertile subgroup, TPOAb positivity was significantly associated with idiopathic low ovarian reserve in unexplained infertility (low ovarian reserve: 28.6%; normal: 15.7%; high: 9.5%; p = 0.020).
Conclusions:
Idiopathic low ovarian reserve was associated with more frequent positive TPOAb rather than thyroid function or TgAb positivity in Chinese women.
Introduction
T
In December 2015, the European Society of Human Reproduction and Embryology (ESHRE) recommended screening for TPOAb in women with premature ovarian insufficiency (POI) of unknown cause (8). Thus, the relationship between TAI and ovarian reserve is of potential interest. Saglam et al. recruited women <40 years old and found that anti-Müllerian hormone (AMH) levels were significantly lower in TAI women than in controls (9). On the contrary, another study reported significantly higher AMH levels in woman with autoimmune thyroiditis compared to the control group (10). Moreover, in a large cross-sectional analysis, there was no association between TAI, hypothyroidism, and reduced ovarian reserve (11). The undetermined relationship between TAI and ovarian function leads to discrepant interpretations and management for women with TAI between reproductive endocrinologists, medical endocrinologists, and immunologists. Because the TAI prevalence was reported to be different between ethnic/racial groups (12), it was hypothesized that an association between TAI and diminished ovarian reserve could be present in Chinese women. More frequent positive TPOAb or higher levels of TPOAb were expected among Chinese women with idiopathic low ovarian reserve.
Materials and Methods
This study was a cross-sectional analysis conducted in the Center for Reproductive Medicine of Taipei Medical University Hospital. The study was approved by the joint Institutional Review Board of Taipei Medical University (TMU-JIRB number: N201607051). Patients evaluated in an infertility clinic at their first entry were offered screening examinations if further assisted reproductive treatments were necessary, which included pelvic sonography, hysterosalpingography, and blood samples taken at Union Clinical Laboratory (UCL) on the third day of the menstrual cycle for serum levels of follicle-stimulating hormone, luteinizing hormone, estradiol, progesterone, testosterone, AMH, prolactin, TSH, TPOAb, and thyroglobulin antibody (TgAb), as well as semen analysis of the partner. Diagnostic laparoscopy and hysteroscopy were not incorporated into routine examinations. The inclusion criteria included: (i) patients at their first entry, (ii) eligible indications for intrauterine insemination or in vitro fertilization, and (iii) available results of all parameters in the screening examinations. Those who were not ethnic Chinese were excluded.
Patients were diagnosed as infertile if they failed to conceive after one year of regular intercourse without contraception. According to the findings of screening examinations, etiologies of infertility were categorized as endometriosis, unexplained infertility, anovulation, tubal factor, uterine factor, male factor, and others. For patients with multiple etiologies, the categorization depended on the judgment of a single staff member according to the severity of each factor. Patients who did not fulfil the criteria of infertility came for reasons such as single woman for egg freezing, couples with hereditary diseases enquiring about preimplantation genetic diagnosis, women suffering from recurrent abortions, and couples trying to conceive for less than one year. History of thyroid dysfunction and causes resulting in reduced ovarian reserve were also evaluated.
The serum AMH levels were assessed by the enzyme-linked immunosorbent assay (ELISA) method with Beckman Coulter reagent before September 29, 2015. For blood samples taken thereafter, the Elecsys electrochemiluminescence immunoassays on a Cobas e411 immunoanalyzer (Roche Diagnostics) were used. A regression line: (Cobas AMH) = 0.804(ELISA AMH) – 0.478, R 2 = 0.910, was derived from 40 samples at UCL for the transformation of the ELISA method to the Elecsys Cobas method (13). The intra-assay and inter-assay coefficients of variation (CV) were <5.66% and <6.97% in the ELISA method and <1.8% and <4.4% in the Elecsys Cobas method. A two-site sandwich immunoassay automated chemiluminescence system was used for the measurement of serum TSH, TPOAb, and TgAb concentrations on the ADVIA Centaur analyzer (Bayer HealthCare). The reference values were 0.550–4.780 mIU/L for TSH and <60IU/mL for both TPOAb and TgAb. The intra-assay and inter-assay CV values for TSH were 4.69% and 3.62% at 0.026 mIU/L, 1.97% and 4.13% at 0.383 mIU/L, 1.95% and 4.28% at 4.17 mIU/L, and 2.26% and 3.99% at 16.6 mIU/L; for TPOAb, they values were <6.8% and <3.4%; and for TgAb, the values were <5.8% and <5.7%, respectively.
There is currently no consensus on the definition of low, normal, and high ovarian reserve in terms of AMH. The Bologna criteria adopted a range between 0.5 and 1.1 ng/mL for AMH as the feature of an abnormal ovarian reserve test (14). A population-based study revealed that around 10% women in the general population experienced early menopause (15). With numerous women having AMH levels lower than the reportable range in the present study population, the whole study subjects were categorized into three distinct groups by age-specific AMH levels (every five years): (i) low ovarian reserve (patients with age-specific AMH below the 15th percentile of the values), (ii) normal ovarian reserve (patients with age-specific AMH between the 15th and 85th percentile of the values), and (iii) high ovarian reserve (patients with age-specific AMH above the 85th percentile of the values). With respect to thyroid function, patients who were on medication for either hyper- or hypothyroidism were excluded from the calculation of median TSH in different AMH groups. The prevalence of positive TPOAb and TgAb along with the levels of TSH were compared between patients belonging to different ovarian reserve categories. Subgroup analyses were performed for patients without known causes compromising ovarian reserve and for infertile patients with different etiologies.
Statistical analyses were performed using MedCalc for Windows v16.0 (MedCalc Software, Ostend, Belgium). Continuous variables were compared by using the Kruskal–Wallis test followed by the Conover test as post hoc analysis, while categorical variables were compared with the use of the chi-square test or Fisher's exact test. Correlations between AMH levels and TPOAb levels were quantified by using Spearman's rho correlation coefficient. Results were considered significant when p < 0.05.
Results
A total of 1044 ethnic Chinese women were enrolled between October 2013 and March 2016 (Fig. 1). Most of them were local Taiwan people, while a small part of them came from Hong Kong or Mainland China. Among them, 157 patients were categorized as having low ovarian reserve, 729 with normal reserve, and 158 with high reserve. There were 111 patients with known causes compromising ovarian reserve, including 106 with iatrogenic causes (ovarian surgery, pelvic radiotherapy, or gonadotoxic chemotherapy) and five with genetic causes (Turner syndrome or Fragile X premutations; Fig. 1).
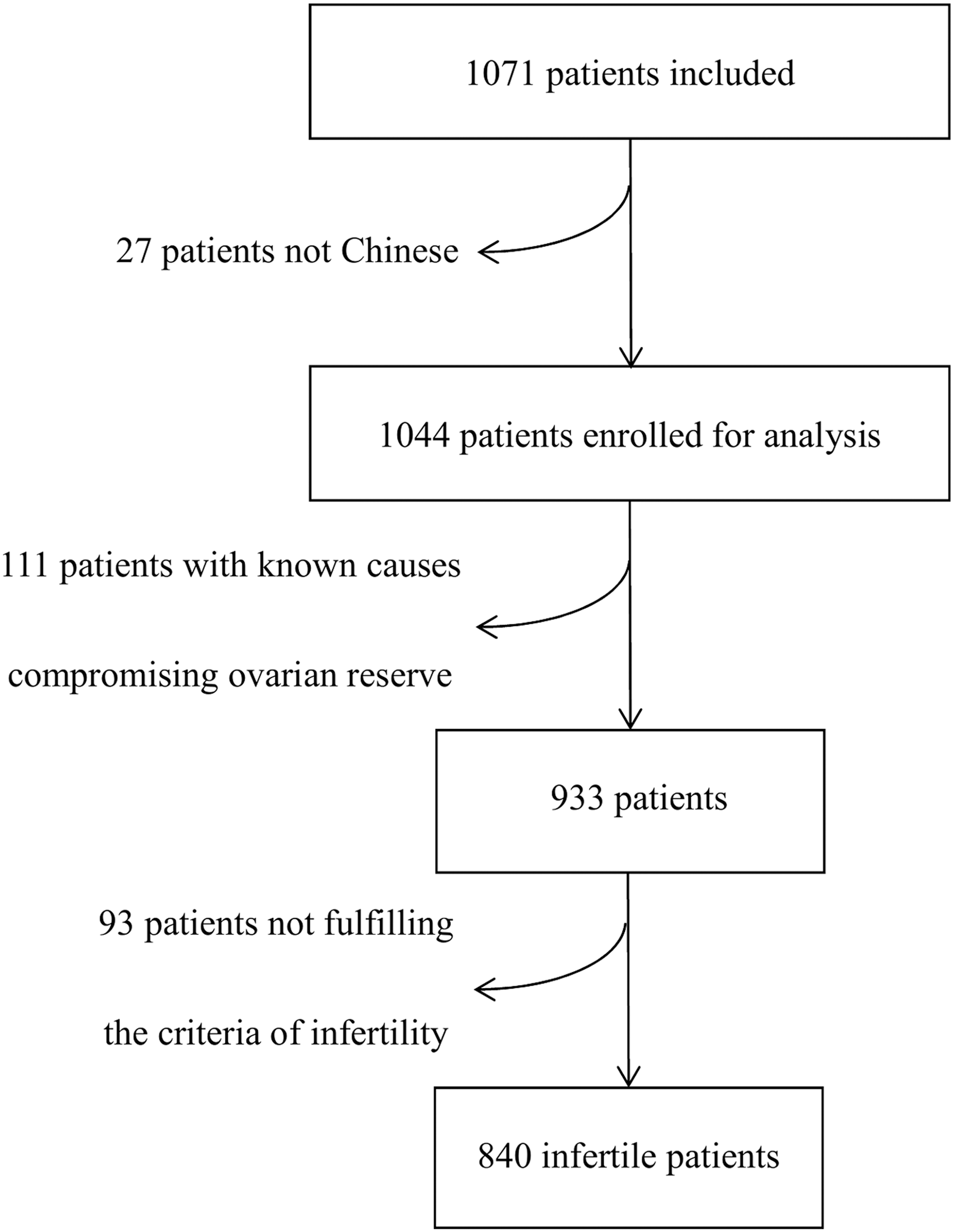
Flow chart of the study.
As shown in Table 1, age and body mass index were comparable between the ovarian reserve groups. For the infertile patients, the etiologies that accounted for the largest proportion in each category of ovarian reserve were unexplained infertility for both low and normal reserve, and anovulation for high reserve.
Values are mean ± SD or n (%).
Single woman for social egg freezing, couples with hereditary diseases enquiring preimplantation genetic diagnosis, women suffering from recurrent abortion, and couples trying to conceive for less than one year.
BMI, body mass index.
Regarding the relationship between thyroid function and ovarian reserve, the median (interquartile range [IQR]) of serum TSH levels were comparable between groups: low ovarian reserve 1.61 mIU/L (1.11–2.24), normal reserve 1.52 mIU/L (1.05–2.20), and high reserve 1.47 mIU/L (1.04–2.40; p = 0.612). An analysis excluding patients with known causes compromising ovarian reserve showed a similar result (Table 2).
Values are presented as mean ± SD.
Values are calculated by excluding 15 patients in total on medication for known hypo- or hyperthyroidism at the time of the serum sampling and presented as median (interquartile range).
Values are presented as n (%).
TSH, thyrotropin; TPOAb, thyroid peroxidase antibody; TgAb, thyroglobulin antibody.
With respect to TAI, the prevalence was 14.1% for positive TPOAb and 15.4% for positive TgAb in the whole study population, while 9.7% had both positive TPOAb and TgAb. The prevalence of positive TPOAb was 6.7% for women aged 25–29 years, 13.3% for those aged 30–39 years, and 18.3% for those aged 40–48 years, which indicates an age-dependent increase. Similarly, the prevalence of positive TgAb also increased with age: 6.7% for those aged 25–29 years, 15.9% for those aged 30–39 years, and 16.5% for those aged 40–48 years. In relation to ovarian reserve, the prevalence was comparable for positive TPOAb—low (19.1%), normal (13.9%), and high (10.1%) ovarian reserve (p = 0.069)—as well as for positive TgAb—low (20.4%), normal (14.8%), and high (13.9%) ovarian reserve (p = 0.181). However, excluding patients with known causes compromising ovarian reserve, only the prevalence of positive TPOAb became significantly different between patients with low (22.7%), normal (14.0%), and high (10.3%) ovarian reserve (p = 0.012; Table 2). There was no correlation between AMH levels and TPOAb levels, whether for the whole study population (Spearman's ρ = −0.013; p = 0.685) or for patients without known causes compromising ovarian reserve (Spearman's ρ = −0.027; p = 0.413; Fig. 2).
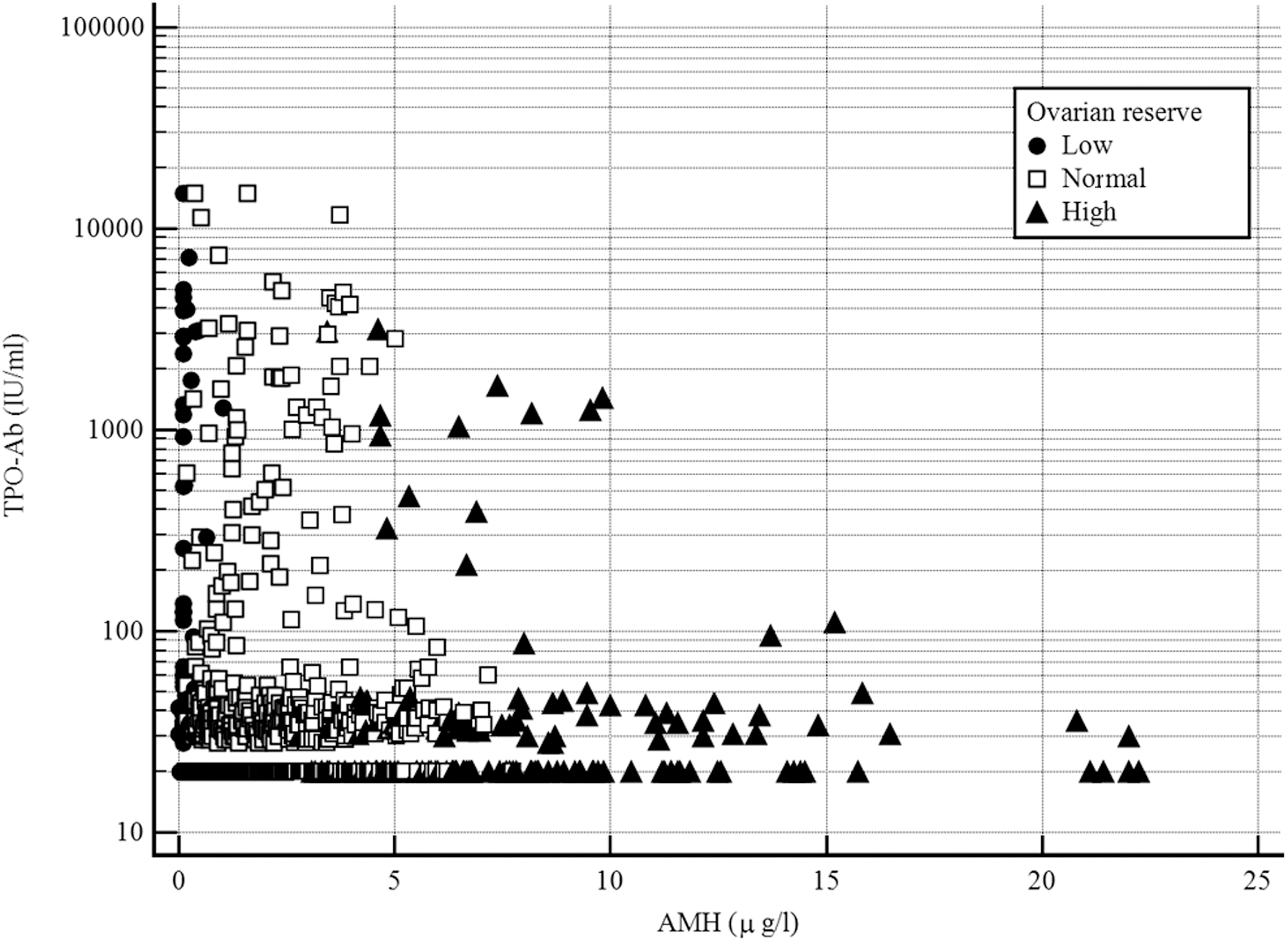
Correlation between anti-Müllerian hormone levels and thyroid peroxidase antibody levels (excluding patients with known causes compromising ovarian reserve). Spearman's rho = −0.027, p = 0.413.
Among the 840 infertile patients (Fig. 1), 116 patients had low ovarian reserve, 589 had normal reserve, and 135 had high reserve. As shown in Table 3, age and the TSH levels were comparable between categories of ovarian reserve. In this infertile subgroup, the prevalence was 15.1% for positive TPOAb and 16.4% for positive TgAb. The prevalence of positive TPOAb differed significantly between infertile patients with low (23.3%), normal (14.6%), and high (10.4%) ovarian reserve (p = 0.014). However, the difference was not significant regarding the prevalence of positive TgAb: low (22.4%), normal (16.1%), and high (12.6%) ovarian reserve (p = 0.105). Classified based on etiologies of infertility, TPOAb positivity in unexplained infertility and infertility related to endometriosis were significantly different between the various AMH groups (Table 3).
Values are presented as mean ± SD.
Values are calculated by excluding 15 patients in total on medication for known hypo- or hyperthyroidism at the time of the serum sampling and presented as median (interquartile range).
Values are presented as number of positive thyroid antibody/total (%).
Discussion
Up to now, this is the largest cross-sectional study investigating the prevalence of TAI in Chinese women. By comparing the AMH levels between women with and without TAI, previous studies reported opposite results regarding the relationship between TAI and ovarian reserve (9,10). On the other hand, this study recruiting >1000 Chinese women clearly demonstrates more frequent positive TPOAb in women with idiopathic low ovarian reserve.
Defining ovarian reserve by age-specific AMH is a characteristic of this study. In comparison to other surrogates for ovarian reserve, such as basal gonadotropin levels, antral follicle counts, and previous response to ovarian stimulation, AMH is an objective marker that remains stable between and during menstrual cycles (16). Because AMH levels decline with age, an age-specific AMH level represents the ovarian reserve more accurately. Among the limited studies utilizing age-specific AMH levels, a large cross-sectional study reported that TAI and hypothyroidism were not associated with low ovarian reserve (11), which is consistent with the present results. This study found no difference in TSH levels and TAI prevalence between groups with variable ovarian reserve if all study subjects were enrolled for analysis. Only when patients with known causes compromising ovarian reserve were excluded did the difference in TPOAb positivity become significant. It is probably the confounding effect of iatrogenic and genetic causes leading to the reduction in ovarian reserve that masked the relationship between TPOAb positivity and low ovarian reserve.
In addition, it was TPOAb positivity rather than TPOAb levels that was associated significantly with ovarian reserve. Once the TPOAb levels were above the reference value, different TPOAb levels would affect ovarian reserve equivalently. An autoimmune pathogenesis is clearly demonstrated in patients with adrenal autoimmunity, in part presumably due to common antigens in the ovaries and the adrenal glands in steroidogenic cells (17). Although a direct connection between TAI and POI has not been documented, the confirmed presence of TPOAb in the follicular fluid obtained from women positive for TPOAb leads to a hypothesis of a cytotoxic effect of TPOAb on oocytes (18). It is also possible that TPOAb is a small part of an activated immune system that actually causes damages to ovarian tissue (19).
In this study, TSH levels were comparable between the different AMH groups, while TPOAb positivity differed significantly. The study failed to demonstrate an association between TPOAb positivity and TSH levels probably because the prevalence of TAI was as high as 31% for women with abnormally depressed TSH. The 20-year follow-up study of the Whickham cohort reported that a detectable TPOAb preceded the development of an elevated TSH (20). A study design recording the hormonal change over time for the same cohort is superior to a cross-sectional design when it comes to investigating the relationship between TAI and TSH.
A high percentage of women in this study had unexplained infertility. Infertile women were candidates for either intrauterine insemination or in vitro fertilization. The association between TPOAb positivity and idiopathic low ovarian reserve in unexplained infertility was similar to that in the whole study population. Among women with anovulatory infertility, no significantly high prevalence of positive TPOAb or TgAb was found for women with high ovarian reserve. Although the prevalence of TAI was reported to be higher in women with PCOS (5), the present finding may be attributed to the small number of women with PCOS in the study population and the ethnic difference (21). In addition, there was an unusual association presented as more frequent positive TgAb in patients with endometriosis with either low or high ovarian reserve. Characterized by ectopic endometrial cells and stroma, endometriosis is often associated with chronic local inflammation and presence of autoantibodies. Although it is not known whether the immunological reaction is one of the etiologies or is secondary to the ectopic tissue, endometriosis does share similarities with autoimmune diseases (22). Previous studies demonstrated both beneficial and detrimental impact of autoimmunity on ovarian reserve (19,23).
Another atypical finding in the present study was a higher prevalence of positive TgAb compared to that of TPOAb, which was also found in studies recruiting women of reproductive age (24,25). A lower prevalence of positive TgAb was related to iodine deficiency because iodination alters epitopes of human thyroglobulin, resulting in generation of TgAb (26). However, the iodine status of the Taiwanese population is merely borderline adequate (27). A higher prevalence of TgAb was also found in Belgium, an iodine-deficient region (25).
Although the cross-sectional design of this study is considered by most as the optimal design to assess the prevalence of conditions, several limitations of this study should be underlined. First, because all the patients were recruited from a single center, a type II error resulting from selection bias cannot be excluded. However, the TAI prevalence derived from >1000 women in this study was close to the results in the National Health and Nutrition Examination Survey III (NHANES III) (12). Second, AMH levels determined by ELISA assays are limited by a high CV. Defining ovarian reserve in a comparative manner, age-specific AMH for example, instead of an absolute cutoff value, helped to reduce the impact of the high CV inherent in the ELISA method. Third, while the etiologies of infertility were diagnosed according to the results of screening examinations, early stage endometriosis, which can only be diagnosed through laparoscopy, may have been categorized into the unexplained infertility group. Lastly, some infertile subgroups became small after patients with known causes compromising ovarian reserve were excluded. For example, nearly half of the endometriosis patients were excluded because of past ovarian surgery, which attenuated the association between TgAb positivity and ovarian reserve in endometriosis patients.
In conclusion, this is the largest survey on the TAI prevalence in Asia and the first study investigating the relationship between TAI and ovarian reserve in a Chinese population. The findings of more frequent positive TPOAb in patients with idiopathic low ovarian reserve and the irrelevance of TPOAb levels to AMH levels suggest a detrimental influence of TPOAb positivity instead of TPOAb levels on ovarian reserve. However, the exact mechanisms directly connecting TPOAb and low ovarian reserve remain elusive and should be studied in the future.
Footnotes
Acknowledgments
The authors thank to the staff at Union Clinical Laboratory for their invaluable help in data collection.
Author Disclosure Statement
No competing financial interests exist.