
Abstract
Background:
Reported results for thyroid nodule fine-needle aspiration (FNA) cytology mainly originate from tertiary centers. However, thyroid nodule FNA cytology is mainly performed in primary care settings for which the distribution of FNA Bethesda categories and their respective malignancy rates are largely unknown. Therefore, this study investigated FNA cytology malignancy rates of a large primary care setting to determine to what extent current evidence-based strategies for the malignancy risk stratification of thyroid nodules are applied and applicable in such primary care settings.
Methods:
In a primary care setting, 9460 FNAs of thyroid nodules were retrospectively analyzed from 8380 patients evaluated by one cytologist (I.R.) during a period of two years. The 8380 FNA cytologies were performed by 64 physicians in different private practices throughout Germany in primary care settings.
Results:
The cytopathologic results were classified according to the Bethesda System as non-diagnostic in 19%, cyst/cystic nodule in 21%, benign (including thyroiditis) in 48%, atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS) in 6%, follicular neoplasms/suspicious for follicular neoplasm (FN/SFN) in 4%, suspicious for malignancy (SFM) in 1%, and malignant in 1%. The proportion of patients proceeding to surgery or with a follow-up of at least one year and the observed risks of malignancy were 22%/8% for AUS/FLUS, 69%/17% for FN/SFN, 78%/86% for SFM, and 71%/98% for malignant. For 112 cytologically suspicious and malignant FNAs, there were 102 true positives and 10 false positives, considering histology as gold standard.
Conclusion:
At variance with other data mostly originating from tertiary centers, these data demonstrate low percentages for malignant, SFM, FN/SFN, and AUS/FLUS, and high percentages for cysts/cystic nodules in this primary care setting in Germany. The risks of malignancy for malignant, SFM, AUS/FLUS, and FN/SFN FNA cytologies are according to Bethesda recommendations.
Introduction
T
Most recent studies evaluating the diagnostic performance of FNA originate from tertiary centers in the United States and report FNA malignancy rates of 8% (5). However, European studies, mostly also from tertiary centers, have reported lower FNA malignancy rates. European FNA cytology studies reported malignancy in 2.9% of 18,359 FNA cytologies (6), 1.8% of 1238 FNA cytologies (7), 2.5% for 2071 nodules clinically selected for increased malignancy risk (8), and 2.0% of 3782 FNA cytologies (9).
Furthermore, studies from Europe reported that the majority of thyroid cancers are not detected by FNA (10). FNA was only used in 21% of patients undergoing diagnostic surgery for a single thyroid nodule in Germany (11), and low preoperative FNA rates were also reported in Belgium (12) and France (13). Moreover, in a setting of a training hospital with 33 cytologists and 49 endocrinologists with varying degrees of experience, FNA was reported as non-diagnostic in 50% (8). In Germany, investigations of thyroid nodule FNA outcomes for larger FNA numbers date back to 1978 (14). In Germany, cytology is mainly performed in non-university settings, and the working group for cytopathology of the German Society of Pathology was recently closed (15).
This leads to several questions such as to what extent are current evidence-based strategies for the malignancy risk stratification of thyroid nodules applied in many European settings? Are they applicable in such settings? What are the outcomes of these practice patterns? This study aimed to answer these questions by investigating the outcome of FNA cytology in Germany by evaluating 9460 consecutive FNAs performed during a two-year period in 38 private practices by 64 physicians in a general care setting in Germany. All FNAs were evaluated by one cytologist.
Patients and Methods
From June 2012 to June 2014, 9584 consecutive FNAs (Fig. 1) of thyroid nodules from 9489 patients were received by the cytology laboratory MVZ Wagnerstibbe in Einbeck (Germany) and were evaluated by one cytologist (I.R.) according to The Bethesda System For Reporting Thyroid Cytopathology (TBSRTC) (16). Of these, 95 FNAs with previous thyroid surgery and 29 FNAs derived from ectopic thyroid tissue or lymph nodes were excluded, resulting in 9460 FNAs. These 9460 FNAs included 408 FNAs of 382 patients with more than one nodule (in these cases, the most malignant nodule was considered), and 672 FNAs of 603 patients who had more than one FNA during the two-year observation period (Fig. 1). Among the 9460 FNAs, there were 1161 malignant, suspicious for malignancy (SFM), atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS), and follicular neoplasms/suspicious for follicular neoplasm (FN/SFN) FNAs. A further breakdown is given in Figure 1. Recently, data were reported for molecular FNA diagnostics of 564 AUS/FLUS, FN/SFN, SFM, and malignant routine air-dried FNA smears with 322 patients with histology and 33 patients with a follow-up of at least one year (17). These FNAs with additional molecular diagnostics form a subset of the 1161 FNAs with AUS/FLUS, FN/SFN, SFM, and malignant cytology analyzed in this study, of whom 477 patients underwent surgery and 95 patients had a follow-up of at least one year.
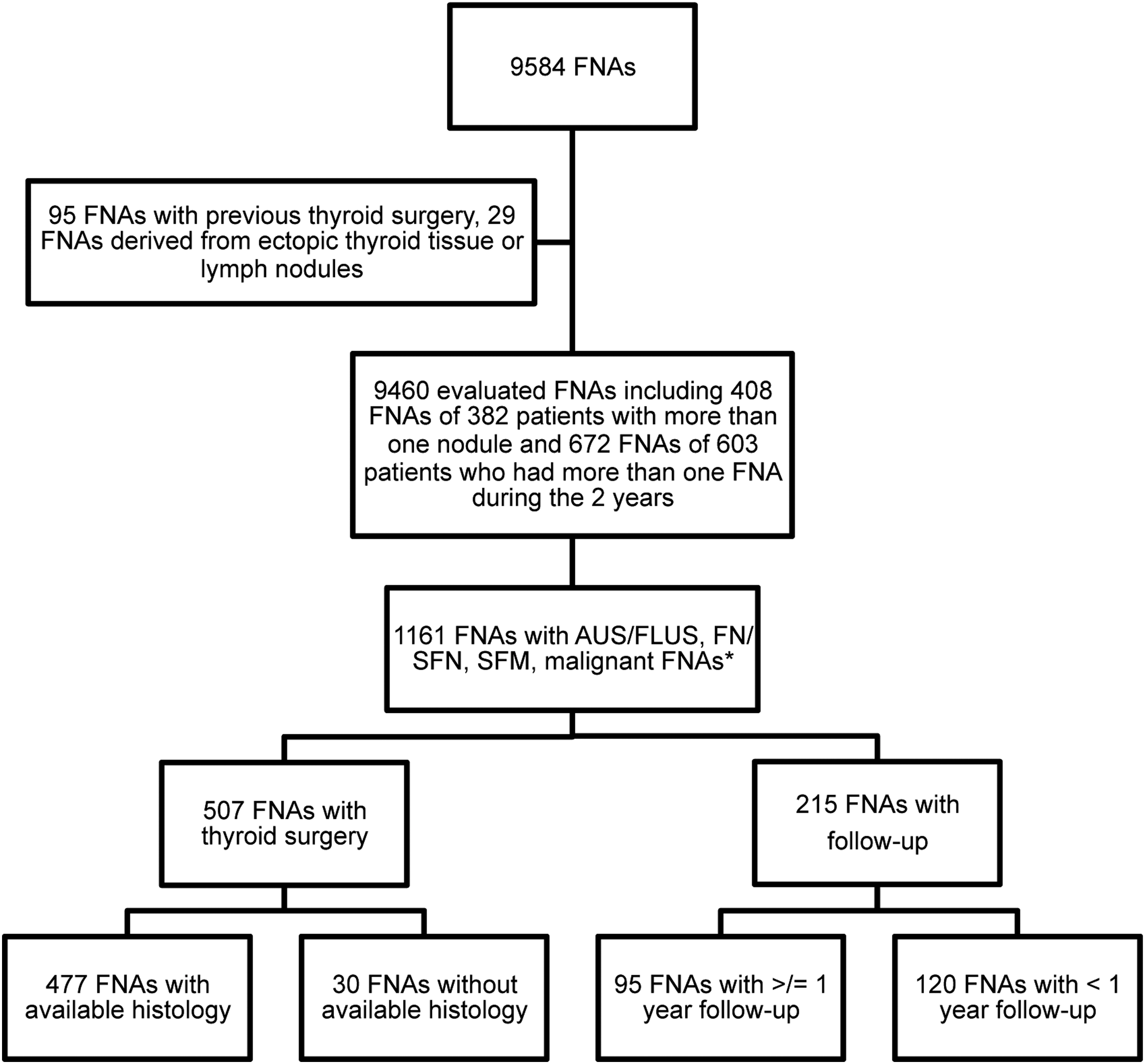
A total of 9584 consecutive fine-needle aspiration (FNA) cytologies were evaluated. Exclusion of 95 patients with 95 FNAs with previous thyroid surgery and 29 FNAs of 29 patients derived from ectopic thyroid tissue or lymph nodules led to 9460 FNAs. These 9460 FNAs included 408 FNAs of 382 patients with more than one nodule (in these cases the most malignant nodule was considered) and 672 FNAs of 603 patients who had more than one FNA during the two-year observation period (in these cases only the first FNA was analyzed). There were 1161 atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS), follicular neoplasms/suspicious for follicular neoplasm (FN/SFN), suspicious for malignancy (SFM), and malignant FNAs. Histology or follow-up of at least a year could be obtained for 572/1161 FNAs. *For distribution of non-diagnostic, cyst, cystic nodules, and benign FNA results, see Figure 2.
For the evaluation of the ultrasound reports, all 408 FNAs of patients with more than one nodule were excluded, and for patients with repeated FNAs, only the first FNA was analyzed, thus resulting in 8380 patients analyzed for ultrasound reports. The FNAs were mostly performed with ultrasound guidance by 64 physicians in 38 different private practices throughout Germany. The median age of the patients was 52 years (range 7–96 years). Data for the molecular FNA diagnostics results for a subset of 564 AUS/FLUS, FN/SFN, SFM, and malignant routine air-dried FNA smears were previously reported (17).
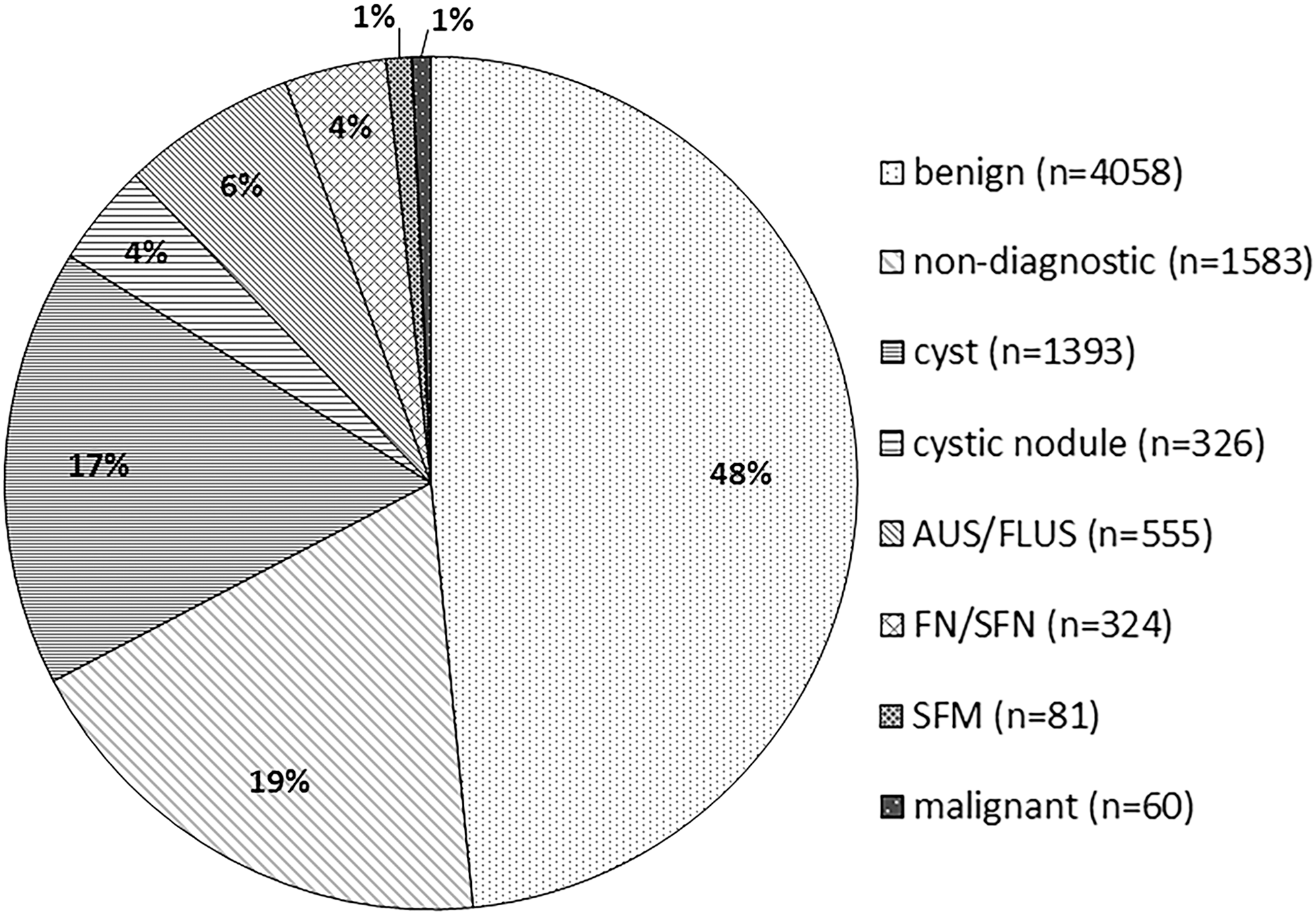
Among the 8380 first FNAs of single thyroid nodules (Fig. 2), there were: 1583 non-diagnostic, 1719 cyst/cystic nodule, 4058 benign (including thyroiditis), 555 AUS/FLUS, 324 FN/SFN, 81 SFM (including suspicious for papillary thyroid carcinoma [PTC], medullary thyroid carcinoma [MTC], and lymphoma), and 60 malignant (including PTC, MTC, anaplastic thyroid carcinoma, poorly differentiated carcinoma, metastasis of non-thyroidal cancer, and lymphoma).
Cytological diagnoses for 8380 first FNAs of single thyroid nodules (n, %).
Availability of clinical data from the cytology submission forms for this retrospective study was dependent on their documentation by the physician performing the FNA. Clinical data given on the cytology submission forms were evaluated in a standardized way for the ultrasound criteria hypoechoechogenicity, blurred margins, hypervascularization, microcalcifications, solid, nodule size (Fisher's exact test was used to evaluate statistical significance; p < 0.05 was considered as significant). Tc-scintigraphy data for decreased uptake (cold) were available on 3857 nodules, and MIBI-scintigraphy data for increased uptake were available for 217 cytology submission forms.
Clinical information regarding nodule size was given on 528 cytology submission forms. The largest diameter given and only those in millimeters or centimeters were evaluated.
For all patients who underwent the 9460 FNAs with a diagnosis of AUS/FLUS or FN/SFN, SFM, or malignant who underwent surgery, the FNA-performing physicians were asked for the histology reports or the follow-up results to determine the malignancy rates of the AUS/FLUS, FN/SFN, SFM, and malignant cytology categories. As not all the FNA-performing physicians had the histologic results available, 38 pathologists were also asked for histologic results. Clinical recommendation for surgery or follow-up were made based on cytological, molecular (if available), and clinical data. Histologic results could be analyzed for 477 (94%) of 507 operated patients. For 95 (44%) of 215 patients undergoing follow-up without surgery, data on follow-up of at least one year could be obtained. A benign follow-up was defined by a cervical ultrasound with a non-suspicious impression after one year and/or a benign repeat FNA. Ethics consent for the retrospective evaluation was obtained from the ethics board of the University of Leipzig.
Statistical analysis
Statistical calculations were based on the following definitions:
Tc-scintigraphy versus cytology: true positives = cold nodules and SFM or malignant cytology; true negatives = warm or isocaptant nodules and benign cytology; false positives = cold nodules and benign cytology; false negatives = warm or isocaptant nodules and SFM or malignant cytology.
MiBi versus cytology: true positives = nodules with increased uptake and SFM or malignant cytology; true negatives = no uptake or isocaptant nodules and benign cytology; false positives = nodules with increased uptake and benign cytology; false negatives = no uptake or isocaptant nodules and SFM or malignant cytology.
Cytology versus histology: true positives = cytology either SFM or malignant and histology malignant; true negatives = benign cytology and benign histology; false positives = SFM or malignant cytology and benign histology; false negatives = cytology benign and histology malignant.
Results
The distribution of the cytological diagnoses for the 8380 FNAs is summarized in Figure 2. Cytological signs of thyroiditis were noted for 119/4058 benign samples. For 1158 (83%) of the 1393 cytological cyst diagnoses and 280 (86%) of the 326 cytologically cystic nodules, there was documented equivalent clinical evidence on the cytology submission form.
Histology in comparison to cytology
Histology reports or data for follow-up could be obtained from the patient files of the treating physician or from the respective pathologist for 477 patients who underwent surgery and 95 patients with a follow-up of at least one year: 129 and 74 of 639 AUS/FLUS, 236 and 21 of 366 FN/SFN, 65 and 0 of 89 SFM, and 47 and 0 of 67 malignant cytology results, respectively. Based on these histological and follow-up data, the observed risks of malignancy were calculated as 8% in AUS/FLUS, 18% in FN/SFN, 86% in SFM, and 98% in the malignant category (Table 1). For 112 cytologically suspicious (n = 65) and malignant (n = 47) FNAs with available histology result, there were 102 true positives (56 SFM, 46 malignant) and 10 (9 SFM, 1 malignant) false positives, considering histology as the gold standard. In a previous study by Eszlinger et al. (17), the risks of malignancy were calculated for a subset of 322 patients with histology and 33 patients with follow-up of at least one year (195 AUS/FLUS, 278 FN/SFN, 55 SFM/SUS, 36 MAL) who underwent molecular FNA diagnostics.
Number and percentage of patients within the FNA categories proceeding to surgery. Number of patients within the FNA categories with histology results. Number of patients with a follow-up of at least one year. Percentage of patients with histology result or patients with FU of at least one year within the FNA categories. Observed risks of malignancy of nodules with available histology result or with a follow-up of at least one year.
AUS/FLUS, atypia of undetermined significance/follicular lesion of undetermined significance; FN/SFN, follicular neoplasms/suspicious for follicular neoplasm; SFM, suspicious for malignancy; CI, confidence interval; FNA, fine-needle aspiration.
Ultrasound in comparison to histology
Overall, at least one ultrasound criterion was available from the cytology submission forms for 4507/9460 FNAs. For 188/477 nodules with histology, thyroid ultrasound data were available from the cytology submission forms. While a statistically significant association of blurred margins with malignant tumors could be shown (p < 0.002), no associations could be shown for microcalcifications, solid nodules, hypervascularization, and hypoechogenicity (Table 2). However, the numbers with data for the different ultrasound malignancy criteria were small.
Number of patients with respective ultrasound criteria/number of patients evaluated for respective ultrasound criteria (percentage of positives of total), p for Fisher's exact test, sensitivity, specificity, PPV and NPV.
PPV, positive predictive value; NPV, negative predictive value.
Size in comparison to cytology
For 528/3987 evaluated cytology submission forms from 8380 patients, the nodule size was stated, with a median nodule size of 2.2 cm (range 0.16–10 cm). Only 18 nodules were <1 cm. For 170 (32%) of the 528 nodules, the nodule diameter was between 3 and 6 cm. The cytology results for these 170 nodules were: FNA benign 86 (50%), AUS/FLUS 20 (12%), FN/SFN 13 (8%), SFM 3 (2%), and malignant 5 (3%). The FNA cytology results for 353 (67%) nodules <3 cm were benign for 201 (57%), AUS/FLUS for 20 (6%), FN/SFN for 23 (7%), SFM for 9 (3%), and malignant for 4 (1%). According to Fisher's exact test (p = 0.40), a nodule size >3 cm is not a predictor of malignant FNA cytology results compared to nodules <3 cm. However, the significance of this result is limited by the low number of malignant samples and the fact that the nodule size was available on only 528/3987 cytology submission forms.
Scintigraphy in comparison to cytology
Tc-scintigraphy results were given on the cytology submission form for 3857/8380 patients. Ultrasound records plus scintigraphy data were given on the cytology submission form for 2016/3857 investigated patients. Cytological results for 3743 scintigraphically cold thyroid nodules were benign in 56% (n = 2089), SFM in 1% (n = 40), and malignant in 0.7% (n = 25).
MIBI-scintigraphy results were given on the cytology submission form for 217 patients. The cytological results for 73% (n = 158) nodules with increased uptake were benign in 32% (n = 51), SFM in 1% (n = 1), and malignant in 1% (n = 2). They were benign in 60% (n = 30), SFM in 2% (n = 1), and malignant in 2% (n = 1) for 23% (n = 50) nodules without uptake, and benign in 78% (n = 7) and malignant in 0% (n = 0) for 4% (n = 9) isocaptant nodules.
Based on these data, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for a cold nodule on Tc-scintigraphy and increased uptake on MIBI scintigraphy were calculated (Table 3) for the distinction of benign and suspicious/malignant cytology results. Whereas sensitivity for Tc-scintigraphy was high (97%), specificity was very low (2%). For MIBI scintigraphy, both sensitivity and specificity were low (60% and 42%, respectively).
Cytological results for 3743 scintigraphically cold thyroid nodules were benign in 56% (n = 2089), SFM in 1% (n = 40), and malignant in 0.7% (n = 25). Sensitivity, specificity, PPV, and NPV for 217 MIBI-scintigraphies with increased uptake to distinguish a benign from a suspicious/malignant cytology result. Cytological results for 73% (n = 158) of the nodules with increased uptake were benign in 32% (n = 51), SFM in 1% (n = 1), and malignant in 1% (n = 2). Twenty-three percent (n = 50) of the nodules without uptake were benign in 60% (n = 30), SFM 2% (n = 1), and malignant in 2% (n = 1), and 4% (n = 9) isocaptant nodules were benign in 78% (n = 7) and malignant in 0% (n = 0).
Non-diagnostic FNAs
A high variance was observed in the number of non-diagnostic (excluding cystic) FNAs per practice (range 10–1117) in the two years, with a median of 15 and a mean of 42. As shown in Figure 3, there is a high heterogeneity for the percentage of non-diagnostic FNAs between the practices, and there is no correlation between the number of FNAs performed and the rates of non-diagnostic FNAs per practice.
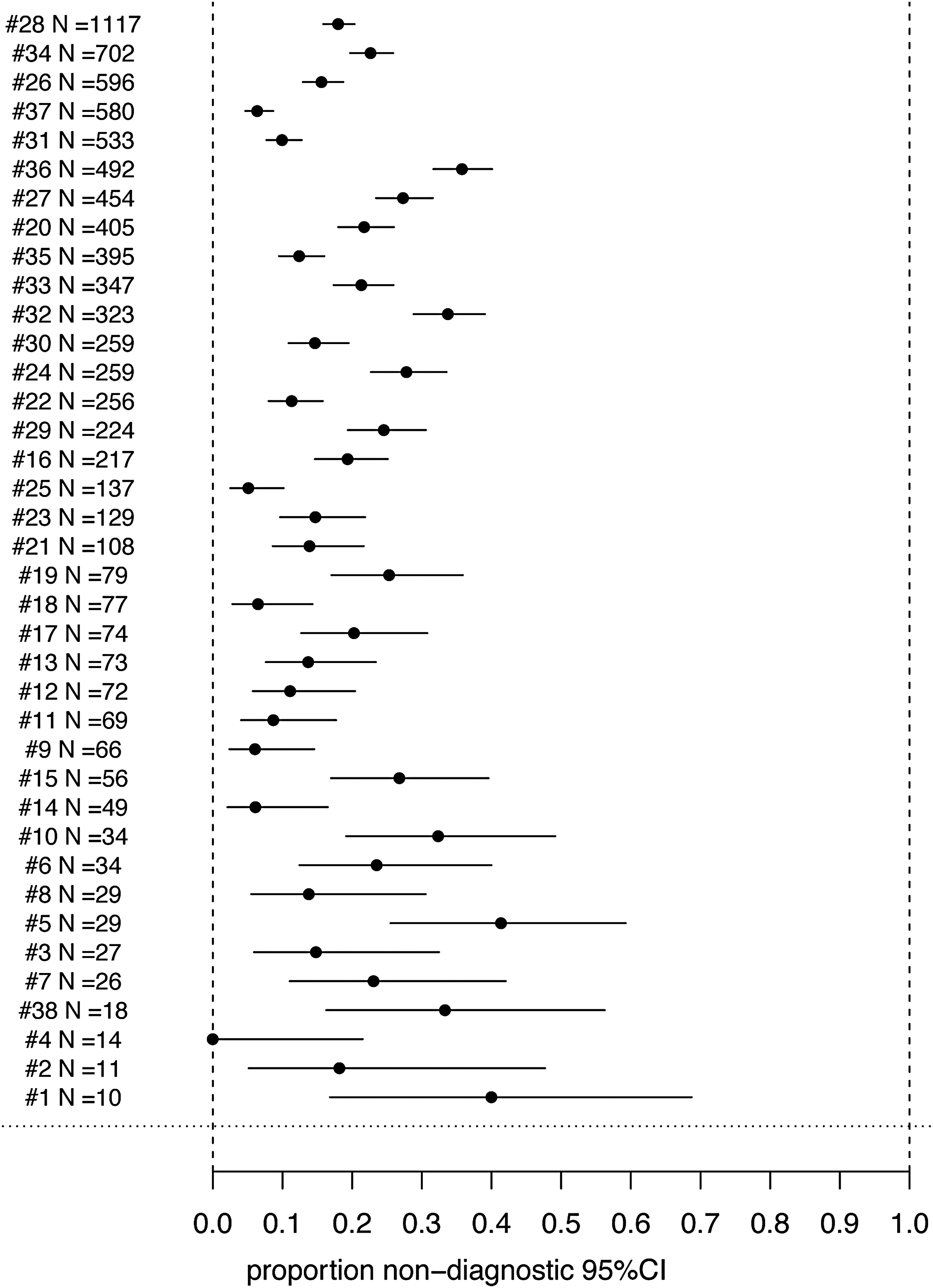
Forest plot showing number of FNAs per practice sorted in ascending number (x) and proportion of non-diagnostic (NDs) FNAs per practice (y) in percent with confidence intervals.
Discussion
At variance with other data mostly originating from academic/tertiary centers, these data from a primary care setting in Germany demonstrate low percentages for malignant, SFM, FN/SFN, and AUS/FLUS thyroid nodule FNA cytology results (Fig. 2) for 8380 consecutive FNA cytologies. It is important to note that only 18 nodules of the 9489 patients were <1 cm. Apart from studies including different cytology classifications (5,18), this is best illustrated by comparison with the results of a meta-analysis of studies analyzing outcomes for the application of TBSRTC, which reported overall percentages of 9.6% for AUS/FLUS, 10.1% for FN/SFN, 2.7% for SFN, and 5.4% for malignant (19). The low percentages for malignant, SFM, FN/SFN, and AUS/FLUS in the present study are associated with a high percentage for cysts/cystic nodules (4%/17%) in addition to 19% non-diagnostic cytologies in this primary care setting in Germany. As cyst cytology results are part of the TBSRTC non-diagnostic category, they are included in the non-diagnostic category of 12.9% (range 1.8–23.6%) for this TBSRTC meta-analysis (19). There was documented equivalent clinical evidence for 83% of the cytological cyst diagnoses and 86% of the cytological cystic nodule diagnoses. Therefore, this high percentage of cysts/cystic nodules distinguishes these results for a primary care setting in a previously iodine-deficient region from those of previous studies mostly originating from academic/tertiary centers. This assumption is supported by the report of only 7% cysts and cystic nodules in the study by Leenhardt et al. (20). Interestingly, in spite of the broad variance for the percentage of the non-diagnostic rates (excluding cysts and cystic nodules) between the practices, there is no correlation between the number of FNAs performed and the non-diagnostic rates per practice in the forest plot (Fig. 3). Poor technique is not necessarily associated with how long the physician has been doing biopsies or how many they do. The high non-diagnostic rates in this study are concerning for inadequate FNA technique training and speak to a general need for nodule selection criteria training and FNA technique training, and they call for avoiding FNA cytologies in nodules with benign and very low suspicion ultrasound patterns.
Risk of malignancy
Generally, the observed risks of malignancy (Table 1) for AUS/FLUS, FN/SFN, SFM, and malignant FNAs are in line with the Bethesda recommendations (16) of the TBSRTC meta-analysis (19). The rates of histology or follow-up for FN/SFN, SFM, and malignant FNAs are similar to the 70%, 74%, and 74%, respectively, for the same categories in the meta-analysis (19). The rates of histology or follow-up are above the pooled surgery rates of 51% and 40% for malignant and suspicious FNAs, respectively, of an older literature review that selected studies with histologic assessment for malignant and suspicious FNAs (21). In contrast, the rate of histology results and follow-up for AUS/FLUS of 32% is relatively low. Thus, the malignancy rate of 8% for this category may be less reliable. However, an even lower malignancy rate of only 3.2% for FLUS has been previously been reported by others (22).
There is lack of consensus and large variation for the calculation and statistical analysis of false negatives, false positives, sensitivity, specificity, NPV, and PPV for FNA cytology studies (5). Moreover, histology rates for benign cytologies are intrinsically low—only 3.2% for the literature review that selected studies with histologic assessment (21). The only exception with a surgical rate of 85% for benign FNACs is by Kuru et al. (23) who reported 2% malignancy for benign FNA cytologies. Moreover, it is inherently clinically biased, thus further reducing the reliability of the statistical analysis of FNA studies for sensitivity, specificity, NPV, and PPV. In a primary care setting with many physicians involved in the care of the patients, the evaluation of follow-up is even more demanding than in academic/tertiary centers. Therefore, the follow-up for benign FNA results was not evaluated, and sensitivity, specificity, NPV, and PPV were not calculated for benign cytologies.
Ultrasound
Pre-FNA ultrasound data were mentioned on only 188/477 cytology submission forms of nodules with histology. Thus, ultrasound criteria apparently only infrequently guided the decision for thyroid nodule FNA in a way that was considered important enough to be forwarded to the cytologist. This interpretation is consistent with the finding that only blurred margins statistically significantly distinguished between benign and malignant histology (Table 2). However, this finding contrasts with the repeatedly reported evidence for the relevance of ultrasound malignancy criteria for the selection of thyroid nodules for FNA (2 –4).
Scintigraphy
Tc-scintigraphy results were given on 278/477 cytology submission forms of nodules with histology (Table 3). More importantly, overall Tc-scintigraphy results were noted on 3857 cytology submission forms, whereas ultrasound data were noted on 3987 cytology submission forms. Ultrasound records plus scintigraphy data were given on only 2016/3857 (52%) cytology submission forms with Tc-scintigraphy results. This suggests that although the ultrasound result was frequently available, it did not influence the indication for a FNA, or it was simply not mentioned on the cytology submission forms. The frequent introduction of Tc-scintigraphy and the relatively low rate of ultrasound data on the cytology submission forms for nodules with histology may suggest that the indication for FNA was more often guided by Tc-scintigraphy than by relevant ultrasound findings. However, the specificity of a cold thyroid nodule on Tc-scintigraphy for a malignant or SFM cytology was only 2% (Table 3). Qualitative MIBI-scintigraphy results were given for 217 patients. Their PPV for a malignant or SFM cytology was only 6% (Table 3). Based on these data, both tests should be excluded from the evaluation of single thyroid nodules, except for suspicion of a hot nodule. It is unclear if this result can be improved by a quantitative analysis of MIBI scans, as recently reported (24).
Conclusion
The current data help to identify likely reasons for the low prevalence of malignancy in the FN/SFN FNA samples such as a likely insufficient use of ultrasound malignancy criteria and overuse of Tc-scintigraphy with low specificity for SFM and malignant cytologies and thus for the selection of patients for FNA. These practice patterns are at variance with current evidence-based guideline recommendations (2,3). More efficient use of ultrasound malignancy criteria and exclusion of Tc-scintigraphy and qualitative MIBI-scintigraphy from the evaluation of single thyroid nodules except for suspicion of a hot nodule for Tc-scintigraphy for thyroid nodule FNA selection and interdisciplinary practice settings would most likely lead to more efficient thyroid nodule malignancy diagnostics and higher risks of malignancy for FN/SFN cytologies (2,3).
Footnotes
Acknowledgments
We would like to thank Dr. Dirk Hasenclever, IMISE Leipzig University, for advice on statistics and Praxen für Diagnostische und Therapeutische Nuklearmedizin, Berlin, Germany; Dr. Seidel, Schilddrüsenpraxis Kantstraße, Berlin, Germany; Dr. Grußendorf, MVZ Rothebühlplatz der Medivision, Stuttgart, Germany; Dr. Rehder, Radiologische Gemeinschaftspraxis, Buchholz, Germany; Prof. Dr. Reinhardt, Oldenburg, Germany; Dr. Yousef, MVZ Nuklearmedizin, Bremerhaven, Germany; Radiologiezentrum Nordharz, Wolfenbüttel, Germany; Röntgenpraxis im Tesdopfhaus, Lübeck, Germany; Dr. Troglauer, Gemeinschaftspraxis für Radiologie und Nuklearmedizin Wiesbaden, Germany; Dr. Wilbert, Radiologisches Institut, Koblenz, Germany; Dr. Körber, Diagnostikum Nuklearmedizin, Fulda, Germany; Radiologische Gemeinschaftspraxis Fischer & Fischer, Trier, Germany; MVZ Endokrinologikum Frankfurt/Main, Germany; Dr. de la Roche, MVZ am Klinikum, Oldenburg, Germany; MVZ Endokrinologikum, Osnabrück, Germany; PD Dr. Dobschütz, Krankenhaus Reinbeck St. Adolf-Stift, Reinbeck, Germany; Dr. Pinick, Internistische Gemeinschaftspraxis, Buchholz, Germany; MVZ Endokrinologikum, Berlin, Germany; and Dr. Strache, Radiologische Gemeinschaftspraxis, Buxtehude, Germany for participating in this study by submitting FNAs for molecular diagnostics and by comprehensively supporting the analysis of the data. M.E. is supported by a Deutsche Krebshilfe grant (109994) and a Wilhelm-Sander-Stiftung grant (2013.010.1). R.P. is supported by the DFG, a Deutsche Krebshilfe grant, and a Wilhelm-Sander-Stiftung grant (2013.010.1).
Author Disclosure Statement
All authors have nothing to declare. No competing financial interests exist.