
Abstract
Background:
In the Study of (E7080) Lenvatinib in Differentiated Cancer of the Thyroid (SELECT) phase 3 trial on advanced radioactive iodine–refractory differentiated thyroid cancer (rDTC), lenvatinib improved median progression-free survival over placebo by almost 15 months and induces an objective response rate of 64.8%, but adverse events occurred in almost all patients. The present study evaluates the efficacy and toxicity of lenvatinib treatment in real-life practice.
Methods:
Clinical charts of 88 consecutive patients treated with lenvatinib from July 2015 to June 2016 in 27 French centers were retrospectively reviewed. Patients treated for other thyroid cancer types (n = 11) or previously treated with lenvatinib within a trial (n = 2) were excluded and the remaining 75 rDTC patients formed the basis of this report.
Results:
75 rDTC patients were analyzed (33 females, median age 65 years [range, 35–88 years]), 12 had an Eastern Cooperative Oncology Group performance status ≥2; 24 cases received lenvatinib as first line systemic treatment; 47 (63%) patients had documented progressive disease prior to treatment initiation. Distant metastases were located in lungs, bones, and lymph nodes (89%, 60%, and 69%, respectively). The initial treatment dose was 24 mg in 54 patients and was lower in the other 21 patients. The median follow-up was 7 months, with a median duration of treatment of 6 months [0.3–15]. Median progression-free survival was 10 months. Among the 65 patients with evaluation of tumor response during treatment, best tumor response was a partial response in 23 patients (31%) and stable disease in 38 (51%). Eleven patients (14.7%) discontinued lenvatinib because of disease progression. Forty-four (59%) and 23 (31%) patients had dose reductions or an interruption of lenvatinib for adverse events (AEs). The most frequent AEs related to treatment were fatigue, hypertension, weight loss, diarrhea, and anorexia. Eleven deaths occurred during the study (one considered to be drug related). Pneumothorax occurred in 2 patients with lung metastases.
Conclusions:
Real-life patients with rDTC can benefit from lenvatinib treatment. AEs are frequent and should be closely monitored.
Introduction
L
In France, lenvatinib could be given to RAI-refractory DTC (rDTC) patients according to the EMA label from April 2015 to January 2017 only within the frame of a temporary use authorization (Autorisation Temporaire d'Utilisation [ATU]). During this period of time, all patients treated with lenvatinib were registered. Prescription and follow-up were based on local practices.
The objective of our national, retrospective, multicenter study performed within the frame of the French Tumeurs de la THYroïde REFractaires (TUTHYREF) network is to describe the efficacy and the toxicity profile of lenvatinib in real life, outside the frame of a clinical trial during this limited period of time when all patients treated with lenvatinib were registered. This is a retrospective study of all consecutive patients treated with lenvatinib between April 2015 and June 2016.
Patients and Methods
Inclusion criteria
Within the frame of the ATU, no patient received lenvatinib between April 2015 and July 2015, and 88 patients were treated with lenvatinib from July 2015 to June 2016. During the ATU, all patients who received the medication were registered by the health authorities to permit its subsequent evaluation in real life.
Selection criteria for treatment were based on the EMA label for lenvatinib and guidelines (4). In real-life practice, lenvatinib was used for the treatment of locally advanced, metastatic rDTC. For most patients, treatment initiation was validated by the multidisciplinary national thyroid tumor board of the TUTHYREF network or by a multidisciplinary regional tumor board. Patients were treated and followed according to local practices. Comorbidities were evaluated per protocol. Efficacy was assessed by imaging with computed tomography scans (CT scans) performed approximately every 3 months (local assessment, RECISTv1.1). 18Fluorodeoxyglucose positron emission tomography and magnetic resonance imaging (brain, axial bones) were performed in selected cases. Serum thyroglobulin evaluations were recorded. Toxic events were recorded retrospectively based on hospital records and were classified according to Common Terminology Criteria for Adverse Events version 4.03.
Data on each patient were retrospectively reviewed during an on-site visit by a single physician (B.A.) between August and November 2016.
Exclusion criteria
Thirteen patients were excluded from the analysis: two patients were already treated with lenvatinib in the phase 3 SELECT trial, one patient had a medullary thyroid cancer, and ten patients had an anaplastic thyroid carcinoma. Here, we report data on 75 DTC patients.
Statistical analysis
Descriptive analyses were performed; quantitative data are expressed as absolute numbers and median or mean. Qualitative data are expressed as percentage of the entire population. Overall survival (OS) and PFS were estimated using the Kaplan–Meier method. PFS was defined as the time between the date of initiation of lenvatinib treatment and progression or death.
Best morphological response was evaluated with an intention-to-treat analysis. The OS was defined as the duration between the date of the initiation of lenvatinib treatment to death from any cause or to the date of the last follow-up.
Results
Patient characteristics
We analyzed the clinical files of the 75 patients with locally advanced or metastatic rDTC who were treated in 27 medical centers. There were 33 women (44%) and 42 men (56%), with a median age of 65 years (range, 35–88). Thirty-two (43%), 22 (29%), 19 (25%), and 2 (3%) patients had a papillary, follicular, poorly differentiated, and oncocytic thyroid cancer, respectively. All patients had demonstrated RAI refractory disease, with the exception of 3 patients who were not treated with RAI because of unresectable thyroid tumors. One patient had unresectable local disease without distant metastases. Seventy-four patients had distant metastases, which were located in lungs in 66 individuals (89%), in bones in 44 (60%), in neck and mediastinal lymph nodes in 52 (69%), and in other sites in 32 patients (liver, brain, adrenal gland, pleural, cutaneous, muscular, peritoneal, splenic, ocular, renal, mammary, and pancreatic) (Table 1).
Fifty-one patients (68%) had received at least one systemic treatment before initiation of lenvatinib: 50 patients had been treated with at least one tyrosine kinase inhibitor (sorafenib: 31, sunitinib: 8, pazopanib: 23, nintedanib: 7, buparlisib: 4, vandetanib: 3, vemurafenib: 1, motesanib: 1), among whom 18 patients had received more than one tyrosine kinase inhibitor (TKI). Eight patients had been treated with cytotoxic chemotherapy (cisplatin and pemetrexed: 1, cisplatin and vinorelbine: 1, doxorubicin based chemotherapy: 3, gemcitabine and oxaliplatin: 3); among these 8 patients, 7 had also been treated with TKI. Lenvatinib was the first systemic treatment for 24 (32%) patients. Treatment of neck recurrences in 31 patients consisted of surgery in 26 (35%) and/or external beam radiation therapy (EBRT) in 12 (16%) patients. Forty-four (59%) patients had focal treatment of distant metastases before lenvatinib initiation: surgery in 23, EBRT in 36, and thermal ablation in 16 patients, including radiofrequency in 6 and/or cryoablation in 7 and/or cementoplasty in 9.
Disease progression before lenvatinib initiation was demonstrated in 47 patients (63%) and could not be assessed in the other 28 patients, among whom 7 patients received lenvatinib because of tumor extension, threatening tumor localization, or symptomatic disease and 21 patients because of an unconfirmed morphological progression. Median doubling time of serum thyroglobulin level before treatment (available for 21 patients) was 5.7 months (range, 0.1–73]. Median time between the date of classification as RAI refractory disease and lenvatinib initiation was 32 months (range, 1–156). Median time between the date of initial thyroid surgery and lenvatinib initiation was 5.9 years (1.1–32.6).
Comorbidities at baseline were identified in 52 cases (69%): 44 patients were treated for hypertension, 3 had ischemic heart disease, 1 had a previous stroke, 1 had cardiac arrhythmia, 1 patient had heart failure, 11 had been treated for another cancer, 1 had chronic hepatitis B, and 1 patient had a gastrostomy (due to tumor invasion of the esophagus). Twelve (16%) patients had an Eastern Cooperative Oncology Group performance status ≥2. Forty-four (59%) patients had symptoms (including hemoptysis in 3 cases) related to DTC before lenvatinib initiation. The median body mass index available in 54 patients was 24 kg/m2 (range, 18–40), and it was lower than 18.5 kg/m2 in 1 patient.
Only 17 patients (23%) would have been eligible for inclusion in the SELECT phase 3 trial. The other patients would have been excluded for because of an Eastern Cooperative Oncology Group performance status ≥2 in 12 patients, uncontrolled blood hypertension (>140/80) in 7, hemoptysis in 3, prostatic cancer that was not in remission in 1 patient, a cutaneous fistula of a bone metastasis in 1 patient, and among the 9 patients with brain metastasis, 3 had not received any focal treatment for the brain lesions. Disease progression at lenvatinib initiation was not assessed in 28 patients, and finally, 18 patients had received more than one systemic treatment with TKI.
Efficacy
After a median follow-up of 7 months (range, 0.4–14.6) after the initiation of lenvatinib treatment, the median duration of treatment was 6 months (range, 0.1–15). At that time, 32 (43%) patients had discontinued treatment and 43 (57%) were still receiving lenvatinib. Three patients received lenvatinib for more than 12 months, and 36 received lenvatinib for 6 to 12 months. The initial treatment dose was 24, 20, 18, 14, and 10 mg/day in 54 (72%), 11 (15%), 1 (1%), 8 (11%), and 1 (1%) patients, respectively. The reasons leading to initiation of treatment with a lower dose were comorbidities in 1, age in 2, alteration of performance status in 9, and unknown reasons in the 9 other patients. Forty-four patients (59%) had a lenvatinib dose reduction after a median time of 63 days. The last lenvatinib dose was 24 mg/day for 20 patients (27%). During the whole period of treatment, the median dose was 20 mg/day.
Morphological evaluation with CT scans during lenvatinib treatment was available for 65 patients (87%). Among the 10 patients who had no morphological assessment, 7 were treated for less than 3 months (2 deaths related to DTC progression, 1 death related to aspiration pneumonia, 3 discontinuations for a toxic event [fall grade 3 with walking disability, fatigue grade 3 and pneumothorax grade 2], and 1 patient with a performance status grade of 4 related to DTC). Three other patients had no morphological assessment, among whom one patient was lost to follow-up.
Among the 75 treated patients, the best morphological response was a partial response (PR) in 23 (31%) patients, stable disease (SD) in 38 (51%) patients, progressive disease (PD) in 4 (5%) patients and was unknown in the absence of evaluation in 10 (13%). There was no complete response. Median time to best morphological response was 3 months (range, 0.4–12.7). Twenty-three (52%) of the 44 patients with initial symptoms related to DTC had clinical improvement of their symptoms (8 patients had a complete clinical response). Symptoms improved in the 3 patients with hemoptysis at baseline. During treatment, serum thyroglobulin levels decreased in 32 patients (43%), increased in 4 patients (5%), was not informative in 2 patients because of antibodies (3%), and was unavailable in 37 patients (49%). Among the 4 patients with an increase in thyroglobulin levels, 2 had a PR and 2 had a SD.
Among the 17 patients (23%) who would have been eligible for inclusion in the SELECT trial, the best morphological response was PR in 8 patients (47%), SD in 8 patients (47%), and was not evaluable in 1 patient; none of these patients had PD as best response.
Among the 54 patients who were initially treated with a lenvatinib dose of 24 mg/day, PR and SD were observed in 17 (31%) and 28 (52%) patients. In the 21 patients initially treated with a lenvatinib dose <24 mg/day, PR and SD were observed in 6 (28%) and 10 (48%) patients, respectively.
Among the 24 patients who received lenvatinib as first-line therapy, PR and SD were observed in 10 (42%) and 12 (50%) patients, respectively. The best morphological response was unknown in 2 (8%). In the 51 patients treated after at least one previous form of therapy, PR, SD, and PD were observed in 13 (25%), 26 (51%), and 4 (8%) patients, respectively. The best morphological response was unknown in 8 (16%). The characteristics of these two groups of patients were not similar, and no statistical comparison was performed.
Among the 3 patients with brain metastasis who did not receive focal treatment before lenvatinib initiation, one patient experienced progression of brain metastasis after 3 months, brain EBRT was performed, and lenvatinib treatment was continued; 1 patient experienced diffuse progression of the disease after 2 months (but morphological brain evaluation was not available); and 1 patient died after 2 days of treatment because of DTC progression.
Median PFS was 10 months (95% CI) (Fig. 1). The 6- and 12-month survival rates were 89% and 79% respectively (Fig. 2). At the end of the study, 11 patients had died. Death was related to DTC in 9 patients, to aspiration pneumonia in 1 patient, and to pneumothorax in 1 patient. At the end of the study (from the start of lenvatinib), more than the half of the patient are still alive so median OS is not reached.

Progression-free survival (PFS) from the time of lenvatinib initiation. Forty-two patients were still treated with lenvatinib at the end of the study.

Overall survival from the time of lenvatinib initiation.
Safety and tolerability
Lenvatinib was transiently interrupted for adverse events (AEs) in 23 patients (31%), for focal treatment of progressive distant metastases in 6 patients, infection in 2 patients, suspicion of progression in 1 patient, unavailability of lenvatinib in 2 patients, and unknown reason in 1 patient.
Thirty-two patients discontinued treatment, including 11 for disease progression, 12 for AEs, 3 for symptoms related to disease without morphological progression, and 6 for other reasons: 1 patient for surgery of metastases, 1 patient for aspiration pneumonia, 1 patient for pulmonary embolism (uncertain relationship to treatment), 1 patient for severe cholecystitis, 1 patient for anal abscess, and 1 patient for infection after total hip arthroplasty not related to lenvatinib. Two patients died of disease progression less than 1 week after lenvatinib initiation (Fig. 3).
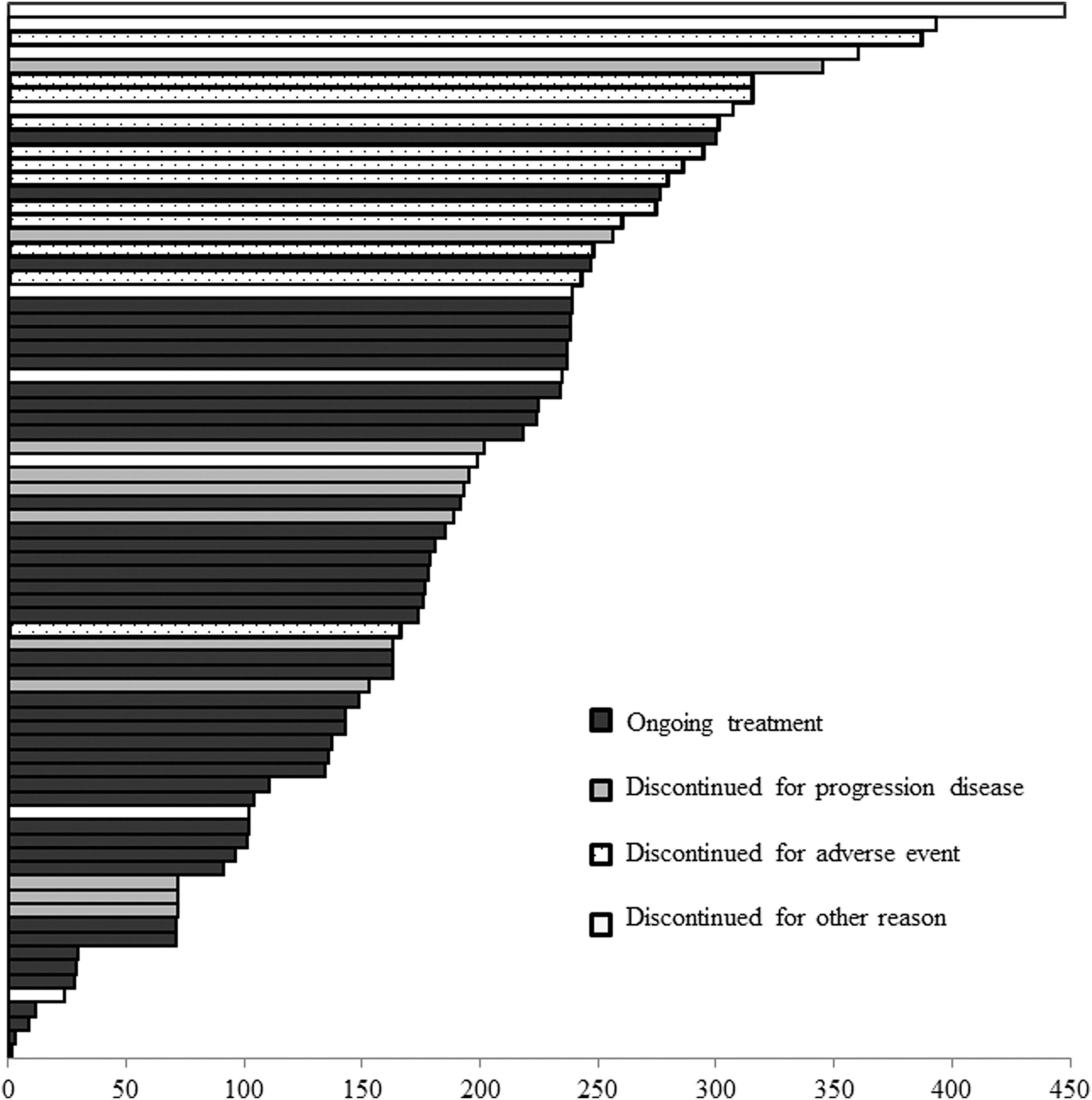
Duration of treatment (in days) and causes of discontinuation: 11 for disease progression, 12 for adverse events, and 9 for other reasons.
The incidence of treatment-related AEs (all grades) was 95%. Seventy-one patients (93%) experienced 375 AEs related to lenvatinib. The incidence of treatment-related adverse events of grade 3 or higher was 48% (36 patients). Fifty-six AEs led to discontinuation of treatment in 23 patients. The most frequent AEs related to treatment (30% or more) were fatigue in 46 patients (61%), hypertension in 50 patients (67%), weight loss in 44 patients (59%), diarrhea in 34 patients (45%), and anorexia in 27 patients (36%) (Table 2). The most frequent AEs leading to discontinuation of treatment were weight loss (14%), anorexia (11%), fatigue (11%), diarrhea (11%), and hypertension (11%). Twenty serious adverse events were reported in 12 patients (16%): fatigue in 4 patients, weight loss in 4, diarrhea in 3, anorexia in 2, hypertension in 1, myocardial infarction in 1, pneumothorax in 2, posterior reversible encephalopathy syndrome in 1, and vomiting in 1 patient. Two patients experienced a pneumothorax that occurred at 71 and 204 days after initiation of lenvatinib treatment, respectively; both had diffuse lung metastases. One patient discontinued lenvatinib at the time of discovery of the pneumothorax and died 4 days later. The other patient continued lenvatinib without dose reduction and the pneumothorax persisted till the end of the study despite chest drainage.
Infections: 12 patients with 15 infections: pulmonary infection (5), urinary infection (3), oral mucositis (2), cutaneous metastasis infection (2), anal abscess (1), dental infection (1), and varicella zoster infection (1).
AE, adverse events.
Discussion
Lenvatinib has recently been approved by the FDA, EMA, and the French authorities to treat DTC patients with advanced and progressive disease that is refractory to RAI. This is the first national study on the use of lenvatinib treatment in real life, outside the frame of any clinical trial. During the ATU period, in a one-year period of time, all French patients treated with lenvatinib were prospectively registered and data were retrospectively analyzed. The 75 consecutively treated patients were managed in 27 medical centers, either belonging to the TUTHYREF network or connected to a center of this network. During this period of time, there was no alternative way to have access to the drug. The number of new patients treated with this medication in France was one per million. However, treatment alternatives mostly within trials were available at that time, and may have significantly decreased the number of candidate patients for lenvatinib treatment. The decision of treatment was discussed within the national or local multidisciplinary tumor board. Treatment and follow-up procedures were heterogeneous according to local clinical practices. The follow-up from initiation of lenvatinib treatment was only 7 months.
Our results confirm the efficacy of lenvatinib that was previously reported in phase 2 and phase 3 trials (3,5). Median PFS was 10 months (not reached by 8 patients) in our study versus 18.3 months in the SELECT study. The intention to treat analyses showed a lower objective response rate than in the phase 3 study (31% versus 64.8%). However, only 17 patients (23%) would have been eligible for inclusion in the SELECT trial. Among these 17 patients, the best morphological response was PR in 8 patients (47%), SD in 8 patients (47%), and was not evaluable in 1 patient; there was no PD. Thus, differences in terms of response rate between this study and the phase 2 and 3 studies probably arise from different characteristics in patient populations. Similar differences in results between phase 3 trial and real-life have been reported with other drugs (6,7). Strict clinical trial entry criteria result in the selection of patients with a better prognosis than the entire pool of all patients. Results are then used in clinical practice, but clinicians should be aware that they cannot be transferred to real life. In contrast, similar overall response rates were 28% in the 21 patients treated with an initial daily dose lower than 24 mg (10–18 mg/day) and 31% in the 54 patients initially treated with 24 mg.
The inferior overall response rates and PFS from this real-life study in patients that were sicker and more heavily pretreated than in the previous phase 2 and phase 3 trials suggest that lenvatinib treatment should be initiated when patients are still in good general condition with a limited tumor burden to take full advantage of its efficacy.
Our study confirms that AEs are frequent. The incidence of treatment-related AEs of all grades was 95%. Dose reductions and drug interruptions were respectively 67.8% and 82.4% in the SELECT study, and 59% and 31%, respectively in this study. Differences in terms of frequencies (48% in this study and 76% in SELECT study) of high-grade AEs, dose reductions, and drug interruptions might be related to lower initial doses of lenvatinib used in the present study. Lenvatinib was discontinued because of AEs in 16% of patients. The incidences of fatigue and of weight loss were higher than in the SELECT study. Hypertension and palmar-plantar erythrodysesthesia syndrome occurred with similar frequencies. Nausea, stomatitis, and vomiting were less frequent. Proteinuria was probably underestimated in our study because urinary analysis was not routinely performed in all patients.
In our study, the only unexpected significant adverse event was a pneumothorax (3,5,8 –10) that occurred in 2 patients with multiple lung metastases. A pneumothorax also occurred during lenvatinib treatment in one of the 10 patients with anaplastic cancer who were excluded from the analysis. Angiogenesis inhibitors are known to cause tumor cavitation in lung tumors (11), and pneumothorax is a known AE occurring with TKI treatment such as pazopanib with a prevalence of 10.3%, with only 2 cases of tumor cavitation among 6 patients with pneumothorax (12). Among the 2 patients with pneumothorax in our study, there was no cavitation, but in one patient there was a necrosis of a lung metastasis with a bronchial fistula associated with the pneumothorax.
Finally, infections were frequent but the relationship with lenvatinib treatment is unknown, because leucopenia was rarely observed.
In conclusion, this retrospective study on the use of lenvatinib in real-life practice confirms that lenvatinib is an effective drug for patients with rDTC. AEs are frequent and should be closely monitored. Most AEs were managed with dose modification and medical therapy.
Footnotes
Acknowledgments
We would like to thank the following physicians for their participation to the study: Bardet Stéphane, De La Fouchardière Christelle, Digue Laurence, Docao Christine, Drui Delphine, Haissaguerre Magalie, Illouz Frédéric, Joly Charlotte, Kelly Anthony, Linassier Claude, Litique Valère, Niccoli Patricia, Roudaut Nathalie, Schneegans Olivier, Schvartz Claire, Senellart Hélène, Zanetta Sylvie, and Zerdoud Slimane.
Author Disclosure Statement
The TUTHYREF network received unrestricted research support from EISAI.