
Abstract
Background:
The purpose of this study was to evaluate health-related quality of life (HRQoL) of community thyroid cancer survivors in Hangzhou, China, and to explore the important correlates defining HRQoL.
Methods:
All thyroid cancer patients who met study criteria in 183 communities were invited to participate (N = 1551). A self-administered questionnaire including collection of personal information and HRQoL instruments was completed by each participant (n = 970), with a response rate of 62.5%. HRQoL was assessed using the Short Form 36 Health Survey and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire. Data for comparison were derived from a representative Hangzhou community sample (N = 1790). After bivariate analyses, multiple linear regression analyses were conducted to investigate independent associations between socio-demographic variables, clinical characteristics, life-style behaviors, and HRQoL.
Results:
Information from 965 participants was available for analysis. A total of 92.1% were diagnosed with papillary thyroid cancer, known as the most common type of thyroid cancer. In general, thyroid cancer survivors have impaired quality of life compared to the age- and sex-matched reference population using the Short Form 36 Health Survey. Thyroid cancer survivors reported the highest level of fatigue and insomnia. Multivariable regression analyses showed that being employed, higher education, and per capita disposable income (24,000–56,000 ¥ per year), and undertaking 30 minutes of moderate physical activity at least five days a week were independent correlates of high physical component summary scores, while being overweight or obese and having a higher dose of levothyroxine intake per day had a negative influence. Being employed, higher per capita disposable income (>56,000 ¥ per year), undertaking 30 minutes of moderate physical activity at least five days a week, and eating more fruit were positively associated with mental component summary scores, while females and patients having more surgeries reported lower mental component summary scores. The global quality of life scale scores were associated with education, employment status, marital status, per capita disposable income, physical activity per week, fruit intake per day, and type of surgery.
Conclusion:
Although patients with thyroid cancer have a very good prognosis overall, in this study, they often experienced more problems than the community reference population, independent of their age and sex. Sex, education, marital status, employment status, weight status, per capita disposable income, number of surgeries, type of surgery, physical activity per week, fruit intake, and levothyroxine intake per day are important correlates of HRQoL of thyroid cancer survivors. Awareness of these relevant factors could help healthcare professionals provide better supportive care.
Introduction
T
Given the longevity of thyroid cancer patients, studies focusing on HRQoL have been conducted. Unfortunately, as of yet, no studies have been conducted in China, and previous findings have been mixed (11). Some studies found a worse HRQoL of thyroid cancer survivors compared to reference groups (5,9,12,13), whereas other studies found a similar HRQoL (1,14). This may be partly due to studies being limited by small sample sizes, lack of appropriate HRQoL instruments available, the absence of healthy control groups, or lack of information regarding specific details about thyroid cancer stage, type of thyroid surgery, and radioiodine treatment (13). The influence of response shift (a change in an individual's values, internal standards, and conceptualization of HRQoL) (15) may also be an issue in some cases. As cancer survival rates improve, there is also growing interest in the role of life-style in HRQoL (16). To date, research has shown that physical activity is positively associated with HRQoL across several cancer groups (17). Thus, there is reason to believe that an unhealthy life-style may itself diminish the HRQoL of cancer patients.
The primary purpose of this study was to compare HRQoL of community thyroid cancer survivors with Hangzhou norms using the Short Form 36 Health Survey (SF-36) (18). Another disease-specific instrument (EORTC QLQ-C30) developed by the European Organization for Research and Treatment of Cancer (EORTC) was also employed to evaluate HRQoL of thyroid cancer survivors and to document their specific complaints. Second, the aim was to explore influential factors of patients' HRQoL including socio-demographics, clinical characteristics, and life-style behaviors, thus helping healthcare professionals provide better supportive care.
Methods
Patients and data collection
This study is a population-based survey among thyroid cancer survivors registered within the Chronic Disease Surveillance System, which compiles data of all individuals newly diagnosed with chronic disease in Zhejiang Province, China. All the thyroid cancer patients were recruited in 183 communities randomly selected from five districts in Hangzhou. To be included, participants had to be at least 18 years old and diagnosed with thyroid cancer before May 2014 in order to ensure that cancer treatment was completed at the time of the survey (November 2014). Patients with other malignant tumors or serious cognitive impairment were excluded.
Aside from providing their personal information, eligible patients were asked to complete the SF-36 and EORTC QLQ-C30. For those who could not read or write, the investigator read to the participant without subjective interpretation. Informed consent was obtained from each study participant after a full explanation of the purpose and nature of data collection and storage. This study was approved by the Zhejiang University School of Medicine Ethics Committee.
Study measures
Socio-demographic, clinical characteristics, and life-style behaviors
Socio-demographic and clinical information was collected via self-report and registry records. Registry data included date of birth, sex, and date of diagnosis. Self-reported data included height and weight, marital status, education, employment status, per capita disposable income, histology, stage of disease at diagnosis, type of surgery, number of surgeries, radioactive iodine therapy, time since diagnosis, and levothyroxine intake per day. Life-style behaviors of participants included physical activity and fruit and vegetable intake, which were also obtained by self-report. “How many days per week do you have 30 minutes of moderate physical activity (such as brisk walking and doing housework)?” rated on a four-point response scale (1 = 0, 2 = 1–2 days, 3 = 3–4 days, 4 = at least 5 days). Fruit and vegetable intake was assessed with one item respectively, asking about the number of portions of fruit and vegetable consumed per day (including examples of a portion size) (19).
Chinese version of the SF-36
The SF-36 is a generic health status instrument designed for use across a wide range of chronic disease populations (20). This self-administered questionnaire consists of 36 items and assesses eight dimensions: physical functioning (PF), role limitations due to physical problems (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and mental health (MH), which can be aggregated to produce physical and mental component summary scores (PCS and MCS, respectively) (21). All SF-36 scales are scored ranging from 0 to 100, with higher scores indicating a better health status. The PCS and MCS are standardized on the basis of a normative general population data set, with the mean set at 50 (standard deviation [SD] = 10), and higher summary scores indicate a better health status as well.
Chinese version of the EORTC QLQ-C30
As there is not a valid, specific HRQoL instrument for thyroid cancer patients in Chinese, the EORTC QLQ-C30 was used to assess cancer-specific quality of life. This 30-item HRQoL questionnaire consists of a global quality of life (QL) scale, five functional scales—physical, role, cognitive, emotional, and social—and three symptom scales—fatigue, pain, nausea and vomiting—and a number of single items assessing common symptoms—dyspnea, loss of appetite, sleep disturbance (insomnia), constipation, diarrhea, and perceived financial impact of the disease (22). The time frame of the questions is the previous week, and each item is scored on a four-point response scale ranging from 1 = “not at all” to 4 = “very much,” with the exception of QL, which is scored on a seven-point modified linear analogue scale ranging from 1 = “very poor” to 7 = “excellent.” After linear transformation, all scales and single item measures range from 0 to 100. A higher score on the functional scales and QL means better functioning and HRQoL, whereas a higher score on the symptom scales means more complaints.
Statistical analysis
The SF-36 and EORTC QLQ-C30 instruments were scored according to the respective scoring methods (23,24). Incomplete questionnaires were handled as per the developer's recommendations. Data derived from descriptive statistical analyses were presented in the form of percentages for categorical variables and of the means and SD for continuous variables.
Mean SF-36 scores of the present study were compared to those of a large Hangzhou general population group (23) (N = 1790) using a one-sample t-test, considering the effect of age and sex.
To identify the determinants of HRQoL, first the effects of participants' characteristics on each SF-36 and EORTC QLQ-C30 scale/item were examined with one-way analysis of variance or the nonparametric Kruskall–Wallis test for categorical variables, depending on the distribution of the variables. The relationship between continuous variables and quality of life scores was examined with Pearson correlation analysis.
The statistically significant variables were then allowed to enter into the multiple linear regression model, and dummy variables were created when appropriate. Dichotomous variables were explored for the regression analysis in order to simplify the relationships. A series of multiple linear regression analyses (stepwise method) were explored to investigate the independent associations between socio-demographics, clinical characteristics, life-style behaviors, and summary scores, including PCS, MCS, and QL scores after checking the assumptions of distribution and independence of the residuals as well as multicollinearity. Normality was assessed by visual inspection of the P-P plot. Linearity and homoscedasticity was investigated by visual inspection of the plot of the predicted values and standardized residuals. The independence of residuals was tested by the Durbin–Watson statistic, which varies between 0 and 4; values <1 or >3 are reason for concern (25). A variance inflation factor (VIF) of greater than 10 was used to identify possible multicollinearity among independent variables (26). All statistical analyses were performed using IBM SPSS Statistics for Windows v19.0 (IBM Corp., Armonk, NY), and a p-value of ≤0.05 was considered statistically significant.
Results
Recruitment results
During the study period, a total of 1551 thyroid cancer patients fulfilled the inclusion criteria (Fig. 1). Of these, 970 thyroid cancer survivors agreed to participate, resulting in a 62.5% response rate. Most refusals were due to lack of interest in research, lack of time, unverifiable addresses, and death prior to the study. Five participants were dropped from subsequent analyses (one because of incomplete responses in the EORTC QLQ-C30, and four medullary thyroid cancer survivors because their sample size was too small to justify analyzing them separately), leaving a total of 965 cases for statistical analysis.
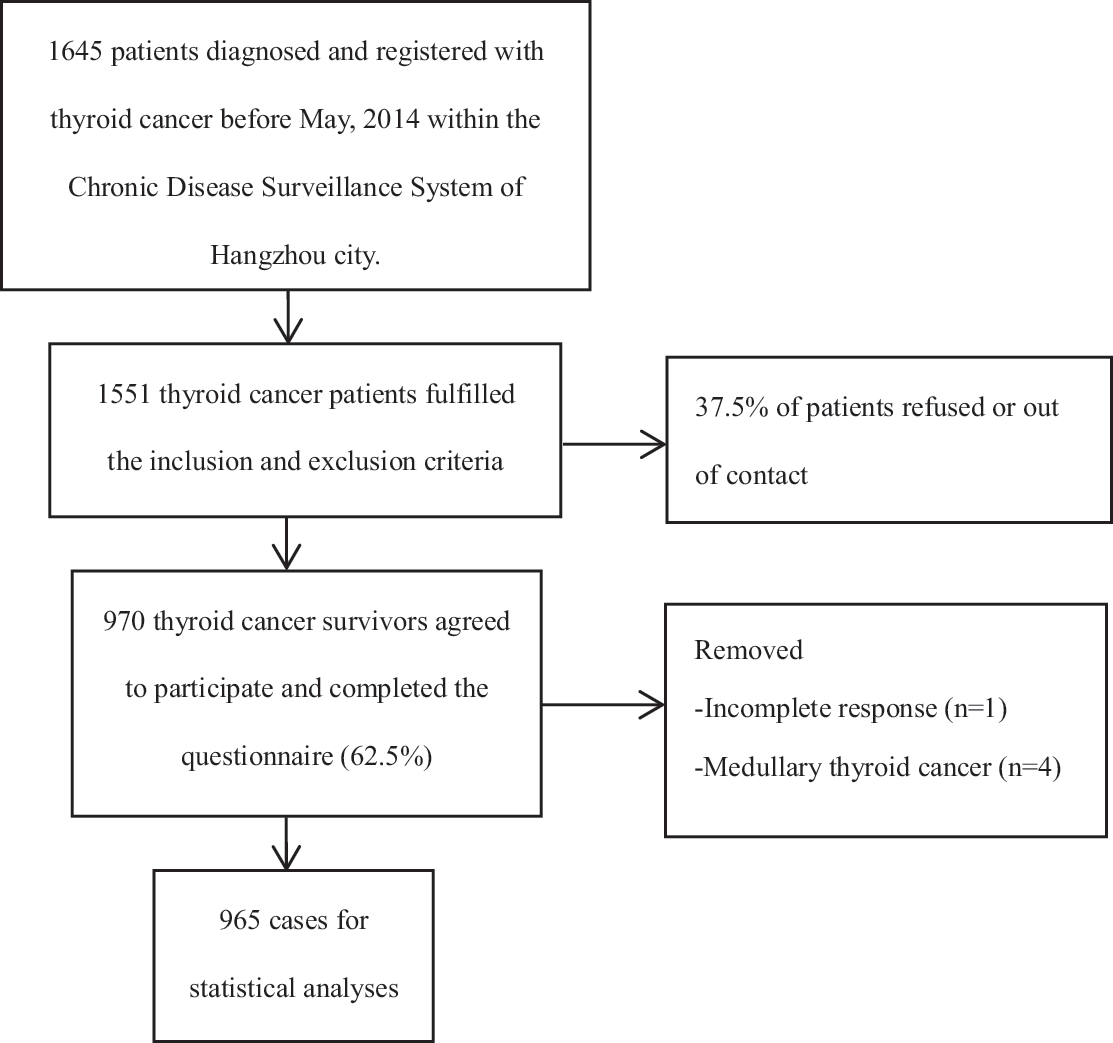
Flowchart of the data collection process.
Participant characteristics and life-style variables
The socio-demographic, clinical characteristics, and life-style data are detailed in Table 1. The mean age of all participants was 49.7 years (SD = 12.3 years), and the female:male ratio was 4:1. The large majority (92.0%) of the participants were married, and about half were employed. The per capita disposable income was categorized as <24,000 ¥, 24,000–56,000 ¥, and >56,000 ¥ (27), with two missing values.
BMI, body mass index; SD, standard deviation.
Height and weight were collected for calculation of body mass index (kg/m2), which was classified as underweight, normal weight, overweight, and obese (28). For all participants, the mean portions of fruit and vegetable intake per day were 1.4 and 3.5 portions, respectively.
There are nine missing values for histology data. Of the respondents, 92.1% were diagnosed with papillary thyroid cancer, known as the most common type of thyroid cancer. Two hundred and sixty-five participants underwent total thyroidectomy, and 297 participants also had neck dissection. Radioactive iodine therapy was administered in 15.2% of the participants. In addition, the mean time since diagnosis of thyroid cancer survivors was 2.6 years (SD = 3.6 years; range <1–10 years), and the mean dose of levothyroxine intake per day was 91 μg (SD = 34 μg). As 73.2% of the participants were uncertain about their stage of cancer, this variable was removed from further analysis.
HRQoL of thyroid cancer survivors
SF-36: thyroid cancer survivors versus Hangzhou reference population
The SF-36 scale and summary scores of thyroid cancer survivors (M ± SD) are described in Table 2. Compared to sex- and age-matched reference groups (23), male patients reported lower GH and MCS scores in the 25–34 age group, lower RP and RE scores in the 45–54 age group, while comparable or higher scores were found in other age groups. Female patients seemed to experience more problems than their male counterparts. In six of eight scales, female patients reported lower scores among at least one age group compared to the reference groups. In summary scores, lower PCS scores among 35–44 and 45–54 age groups and lower MCS scores among all age groups except 25–34 and ≥65 age groups were found in female patients. In all scales of the SF-36, thyroid cancer survivors reported higher or comparable SF and MH scale scores, lower scores in BP and VT scores in 45–54 female patients, and lower scores in PF, RP, GH, and RE scores in at least three age/sex groups.
Sex- and age-matched reference population was adopted from a previous survey in Hangzhou using a multi-stage stratified random sampling approach (23). Nine “Jiedao” (sub-district neighborhood) were randomly selected from three districts (central, sub-central, and suburb), three for each. Two communities from each “Jiedao” and 70 households from each community were randomly selected. The total sample size was 1800, with 200 in each “Jiedao.” All residents ≥14 years old and living in a sampled household for at least six months were eligible to participate until the quota for each “Jiedao” was met. A total of 1790 returned questionnaire were regarded as valid.
The scores of thyroid cancer survivors are significantly lower than reference population (p ≤ 0.05).
The scores of thyroid cancer survivors are significantly higher than reference population (p ≤ 0.05).
No male patients in this age group.
SF-36, the Short Form 36 Health Survey; PF, physical functioning; RP, role limitations due to physical problems; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role limitations due to emotional problems; MH, mental health; PCS, physical component summary; MCS, mental component summary.
EORTC QLQ-C30: disease-specific HRQoL of thyroid cancer survivors
As shown in Table 3, survivors reported a relatively good HRQoL, with the mean scores of all five functioning scales >90. The general symptom ratings suggest few physical health problems, with the exception of problems with fatigue (mean score = 14.8) and insomnia (mean score = 12.9).
A higher score indicates better functioning.
A higher score indicates more symptoms.
Correlates of HRQoL, including socio-demographic and clinical and life-style variables
Among thyroid cancer survivors, significant differences in summary HRQoL scores (the PCS and MCS scores of the SF-36 and the QL scores of the EORTC QLQ-C30) were found between different subgroups on all categorical correlates except histology types, and the correlations between continuous variables and summary HRQoL scores were also significant (Table 4).
Significant differences in quality of life scores among variable groups with analysis of variance or Kruskall–Wallis test (p ≤ 0.05).
Significant correlation between continuous variables and quality of life scores with Pearson correlation analysis (p ≤ 0.05).
The assumptions for linear regression were met for the data. Linearity, homoscedasticity, and normal distribution of residuals were validated in the models. The d-values for the Durbin–Watson test were 1.75, 1.70, and 1.68 for PCS, MCS, and QL scores, respectively. The VIFs were <10, indicating multicollinearity was not observed in the models.
Multivariable analyses were then performed to identify these variables with a significantly independent impact on HRQoL. The PCS, MCS, and QL were dependent variables, and independent variables of the models were age, sex (male as reference), education (more than high school vs. high school and below), marital status (married vs. not married), employment status (employed vs. not employed), vegetable intake per day, fruit intake per day, time since diagnosis, levothyroxine intake per day (μg), per capita disposable income (<24,000 ¥ as reference), weight status (normal weight as reference), 30 minutes of moderate physical activity per week (30 minutes of moderate physical activity ≥5 days a week vs. <5 days), radioactive iodine therapy (no as reference), type of surgery (hemithyroidectomy as reference), and number of surgeries (once as reference).
Being employed, higher education and per capita disposable household income (24,000–56,000 ¥ per year), and doing 30 minutes of moderate physical activity on at least five days a week had a positive influence, while being overweight or obese, and a higher dose of levothyroxine intake per day had a negative influence on PCS scores. Being employed, higher per capita disposable income (>56,000 ¥ per year), doing 30 minutes of moderate physical activity on at least five days a week, and eating more fruit per day were independent correlates of higher MCS scores, while females and patients having more surgeries reported lower MCS scores. With regard to QL, higher QL scores were statistically associated with higher education, being employed and married, higher per capita disposable income (>56,000 ¥ per year), doing 30 minutes of moderate physical activity on at least five days a week, and eating more fruit per day. In addition, survivors who underwent total thyroidectomy and neck dissection reported significantly lower QL scores compared to those who underwent hemithyroidectomy. Age, vegetable intake, time since diagnosis, and radioactive iodine therapy appeared not to be significant correlates of HRQoL (Table 5).
p ≤ 0.05; b p ≤ 0.01.
NA, no entry into the models.
Discussion
Although it is well known that patients with thyroid cancer mostly have a good prognosis, HRQoL has not been well studied, especially in the Asian population (5). This is the first study to evaluate HRQoL of community thyroid cancer survivors in China, and further identifies the important correlates of their HRQoL. A relatively high response rate of 62.5%, resulting in 965 participants, makes this study one of the largest to date to evaluate HRQoL in thyroid cancer survivors. The SF-36 was the most frequently used HRQoL instrument for studies looking specifically at patients with thyroid cancer (29). However, the generic instrument may not address those issues of relevance to particular groups such as disease symptoms or treatment side effects (20). Taking the above into account, administration of both the SF-36 and EORTC QLQ-C30 could not only compare HRQoL scores of thyroid cancer survivors with those of the general population, but also discover specific complaints of these patients.
Thyroid cancer survivors appear to have impaired quality of life compared to the age- and sex-matched reference population. Although this result is in accordance with other studies (5,9,12,13), this study includes a higher number of participants, adopts the generic SF-36 instrument suitable for both patients and general population, and uses a matched control group. The results of the EORTC QLQ-C30 also showed that thyroid cancer survivors reported a relatively good HRQoL, with the mean scores of all five functioning scales being >90, which is higher than those reported in many other cancer populations, including lung, colon, rectal, and breast cancer (30). Nevertheless, survivors did have some specific complaints. The most frequent complaints of thyroid cancer survivors were fatigue and sleep disturbances, consistent with other findings (11,30). One possible explanation for that is cancer-related fatigue, which is a symptom frequently experienced by survivors, regardless of tumor type or its treatment, and not likely to be relieved by rest (31,32). Psychological distress may also play a role, as an earlier study showed that psychological distress was strongly associated with fatigue (31). Another explanation is thyroid hormone disorders. The removal of the thyroid gland is accompanied by a lifelong dependence on levothyroxine, with dosing regimens often suppressing thyrotropin (33). However, substitution with levothyroxine may not replicate the physiological situation of the patient (31); being hypothyroid or hyperthyroid would affect the metabolic function of the body, leading to fatigue and sleep disturbances.
In multivariable analyses, female thyroid cancer survivors reported significantly lower MCS scores, perhaps due to sex-dependent different reactions to the cancer, but also due to sex-dependent different coping strategies (8). Overweight or obese survivors reported significantly lower PCS scores, indicating that more suffer from these morbidities or treatment. Meanwhile, a recent study showed that a higher BMI was significantly associated with an increased risk of papillary thyroid cancer (34). The results showed that survivors with a higher educational level had better HRQoL, which is in agreement with previous research (5,35,36). Higher educated patients possibly have a better understanding of the disease and look for appropriate care for their condition, which might lead to lower levels of anxiety and depression and better coping strategies (36). Survivors who were employed reported better HRQoL. In the light of this finding, returning to work as soon as possible should be a goal in the management of these patients (5). Furthermore, marital status and per capita disposable income were statistically associated with HRQoL, indicating that family support and financial support are both of great importance to thyroid cancer survivors.
Previous data showed that there was no difference in HRQoL scores between patients who underwent total thyroidectomy and patients who underwent hemithyroidectomy (1,37,38). Likewise, no difference between total and subtotal thyroid resection was found in this study. However, thyroid cancer survivors who underwent total thyroidectomy and neck dissection reported significantly lower QL scores compared to those who underwent hemithyroidectomy only, which is in line with the report by Almeida et al. (39). Survivors who underwent surgeries more than once reported significantly lower MCS, suggesting that they suffer more psychological discomfort. Studies showed that HRQoL is impaired after short-term follow-up (<5 years), but a longer duration of cure was associated with better outcome scores (8,12,40). In this study, HRQoL was not influenced by the time since diagnosis, which may be explained by the short mean duration since diagnosis of 2.6 years. A negative correlation was found between PCS scores and levothyroxine intake per day in accordance with a previous study (41). Exposure to excess thyroid hormone can lead to subclinical hyperthyroidism, which has potentially harmful effects on bone metabolism and the cardiovascular system (42) and is even associated with increased mortality due to cardiovascular diseases (43). It is important for thyroid cancer survivors to undergo regular medical checkups to adjust the dose of levothyroxine.
Another noteworthy finding of this study is that life-style behaviors played an important role in HRQoL of thyroid cancer survivors, which has been reported in cancer groups (44). According to the American Cancer Society Recommendations (45), cancer survivors are advised to (i) undertake at least 150 minutes of moderate physical activity per week, (ii) consume at least five servings of fruits and vegetables per day (5-A-Day), and (iii) not smoke. Descriptive data indicated that about 43.6% of thyroid cancer survivors met the recommendations for physical activity, which is higher than breast cancer survivors and endometrial cancer survivors (44,46). This study found a consistent positive association between physical activity and HRQoL. Exercise may improve HRQoL in thyroid cancer survivors by improving physical fitness, controlling treatment-related side effects, and providing a positive distraction from distressing events. This study also revealed that thyroid cancer survivors who ate fruit every day reported significantly better HRQoL scores. Thus, interventions to increase physical activity and fruit intake should be warranted and may have additive effects on HRQoL of thyroid cancer survivors.
Despite these interesting findings, there are some limitations that need consideration. First, the sample does not represent a general thyroid cancer population. Participants had completed cancer treatment at the time of the survey, and most participants were diagnosed with papillary thyroid cancer. Four medullary thyroid cancer survivors were dropped because their sample size was too small to justify analyzing them separately, thus making it more difficult to compare subgroups, and this may further compromise the generalization of the results. Nevertheless, this distribution may likely reflect the incidence pattern of thyroid cancer rather than any biased selection of patients. Second, disease stage was removed from analysis because 73.2% of the participants were uncertain about their stage of cancer. It is assumed that this is a lower risk, as 84.8% of participants did not receive radioactive iodine therapy, and there have been studies that showed controversial results about the relationship between HRQoL and disease stage (11,31,35,47). Third, this study is a population-based survey where socio-demographic and all clinical characteristics (except date of diagnosis) and life-style behaviors were self-reported. There is a chance of recall bias of clinical information for events that happened several years ago, especially for histology category or type of surgery. Also, self-report assessments used for the life-style behaviors are typically inferior to validated assessments or objective indicators. Fourth, the model explains a relatively small proportion of the variation, and other variables (such as anxiety and depression) (9) and longer duration (8,12,40) could be further examined. Lastly, the study was cross-sectional, which could not draw causal inferences concerning the relationship between targeting variables and HRQoL, but bidirectional effects are likely. Does the variable of interest predict effects on various domains of quality of life for thyroid cancer survivors or does the good quality of life help to explain the characteristics of subjects? A previous study revealed that quality of life improvements have a bidirectional relationship with increased physical activity and vocational status for coronary heart disease patients (48). Life-style habits may influence subsequent quality of life. However, the reverse association, in which HRQOL influences subsequent behavior, may also be true. It is plausible that poor HRQoL may lead to unhealthy life-style habits, such as smoking and lack of exercise (49). Thyroid cancer survivors who have higher HRQoL may be more likely to have a greater understanding of their condition and take advantage of educational resources (50). Further longitudinal studies are needed to examine causation of observed association and tailor better intervention for community thyroid cancer survivors.
Although patients with thyroid cancer have a very good prognosis overall, they often experience more problems than a community reference population, independent of their age and sex. Sex, education, marital status, employment status, weight status, per capita disposable income, number of surgeries, type of surgery, physical activity per week, fruit intake per day, and levothyroxine intake per day are important correlates of HRQoL of thyroid cancer survivors. Awareness of these relevant factors could help healthcare professionals provide better supportive care.
Footnotes
Acknowledgments
We would like to express our gratitude to all staff for their health survey and data collection efforts. We would also like to thank all of the patients for their participation. This study is supported by a grant from Hangzhou Municipal Science and Technology Bureau (No. 20130733Q33).
Author Disclosure Statement
The authors have declared no conflicts of interest.