
Abstract
Background:
Recent intervention studies have suggested that selenium (Se) is an effective treatment for autoimmune thyroiditis (AIT). However, the exact effect of Se on AIT is unclear as well as the mechanism of action. The aim of the present study was to explore the effect of Se on thyroid peroxidase antibody (TPOAb) titers in patients with AIT and to analyze the potential impact of the genetic background on the effect of Se supplementation.
Methods:
This was a randomized, placebo-controlled, double-blind trial. Three hundred and sixty-four patients with elevated TPOAb (>300 IU/mL) were recruited and randomized to receive Se yeast 200 μg/day supplementation or placebo. Urinary iodine concentration, serum thyrotropin, free thyroxine, TPOAb, Se, malondialdehyde, and serum glutathione peroxidase activity were measured at baseline and follow-up. Ninety-six patients were genotyped for single nucleotide polymorphism r25191G/A in the selenoprotein P (SEPP1/SELENOP) gene.
Results:
The median urinary iodine concentration was 182 μg/L. Serum Se increased significantly (p < 0.001) after Se treatment. TPOAb titer decreased by 10.0% at 3 months and by 10.7% at 6 months after Se supplementation, while there was a moderate increase in TPOAb titers over the follow-up period in patients receiving placebo. Glutathione peroxidase activity significantly increased (p < 0.001), and malondialdehyde significantly decreased (p < 0.001) after 6 months of Se supplementation. TPOAb titers decreased to variable extents in patients with different genotypes of single nucleotide polymorphism r25191G/A after Se supplementation. Serum TPOAb titers in patients with the AA genotype showed a more significant decrease (by 46.2%) than those with the GA and GG genotypes (by 14.5 and 9.8% respectively) at 3 months of Se supplementation (p = 0.070).
Conclusions:
Se supplementation significantly reduced TPOAb titers in patients with AIT, and there may be an important genetic component influencing interindividual differences in the decrease in TPOAb titers.
Introduction
A
The trace element Se is an essential nutrient for human health (12 –16). Its biological functions are mediated in most cases by 25 genes encoding selenoproteins of the human selenoproteome (12). Well-characterized selenoenzyme families are functionally expressed in thyrocytes including glutathione peroxidases (GPx), thioredoxin reductases (TrxR), selenoprotein P (SEPP1), and iodothyronine deiodinases. These selenoenzymes influence thyrocyte function by acting as antioxidants, thereby modifying redox status and thyroid hormone metabolism (13 –16). SEPP1 is one of the best-known plasma selenoproteins. As SEPP1 is predominantly produced in the liver and later secreted in the plasma, it can act as a Se transporter, transporting Se from the liver to other tissues. Some recent studies have found that a single nucleotide polymorphism (SNP r25191g/a) within the human SEPP1 (SELENOP) gene may act as an indicator of Se status and the response to supplementation, and thus of susceptibility to Se deficiency diseases (17 –19).
Our aim was to conduct a prospective, multicenter, randomized, blinded, placebo-controlled study in patients with AIT in China to evaluate whether supplementation with 200 μg/day of Se yeast either alone or in combination with L-T4 has any effect on serum TPOAb titers or thyroid function tests in patients with clinical or subclinical AIT. Furthermore, we explored whether polymorphisms in the SEPP1 gene are associated with the effect of Se supplementation on TPOAb titers via SNP r25191g/a genotype detection.
Materials and Methods
Subjects
Three hundred sixty-four patients from fivr different areas in China, including Shenyang, Beijing, Jinan, Dalian, and Guangzhou, were included in this study. Patients from all five cities were iodine sufficient at baseline, with a median urinary iodine concentration (UIC) of 169 μg/L, 156 μg/L, 185 μg/L, 154 μg/L, and 174 μg/L, respectively. Inclusion criteria were: (1) women aged from 15 to 70 years; (2) elevated serum TPOAb (>300 IU/mL); (3) thyroid hormone levels within the reference range—though thyrotropin (TSH) levels could be above the upper normal level (subclinical hypothyroidism); (4) patients not receiving any medication that can affect Se bioavailability or peripheral conversion of T4 to T3 or medications that could influence thyroid autoimmunity including corticosteroids, preparations containing vitamins or trace elements, amiodarone, propranolol, penicillamine, interferon alpha, lithium, antidepressants, or antipsychotic drugs; and (5) nonsmokers. The study was registered in the Clinical Trial Registry (ChiCTR-TRC-00000155). The medical ethics committee of the First Hospital of China Medical University approved this study, and all subjects provided informed consent prior to participation (protocol number [2008]29).
Patients were divided into two groups according to their thyroid function status: Group 1 (n = 313) had subclinical AIT, defined as positive TPOAb with euthyroidism (n = 242) or subclinical hypothyroidism (n = 71) and not receiving L-T4 replacement therapy. Group 2 (n = 51) comprised women diagnosed with clinical AIT (overt clinical hypothyroidism and positive TPOAb) and who achieved normal thyroid function with L-T4 therapy. Patients from both groups were randomized for treatment with Se or placebo: 153 patients in group 1 (G1-S) and 28 patients in group 2 (G2-S) received high-Se yeast (200 μg/d Se) for 6 months, while 160 patients in group 1 (G1-P) and 23 patients in group 2 (G2-P) received placebo yeast for the same time period. Clinical and laboratory examinations of patients were performed at baseline, and at 3 months and 6 months after starting treatment. The follow-up rate was more than 80%. All 96 patients receiving Se supplementation from the Shenyang area signed an informed consent form to carry out genotyping.
Methods of sampling and laboratory testing
Blood samples were obtained from each participant on the morning after fasting overnight at baseline, and after 3 and 6 months of Se supplementation. All sera obtained were immediately analyzed for TSH, free thyroxine (FT4), and TPOAb concentrations using a chemiluminescence immunoassay (Diagnostic Products Corporation, Los Angeles, CA). The functional sensitivity of the TSH assay was 0.02 mIU/L. The intra-assay coefficients of variation (CV) for the serum TSH, FT4, and TPOAb assays were 1.57–4.12%, 2.24–6.33%, and 2.42–5.63%, respectively. The interassay CVs were 1.26–5.76%, 4.53–8.23%, and 5.23–8.16%, respectively. The reference ranges for TSH and FT4 were 0.3–4.8 mIU/L and 10.3–24.5 pmol/L, respectively. Serum Se was measured using inductively coupled plasma mass spectrometry, and the intra- and interassay CVs were 5% and 8%, respectively. Glutathione peroxidase (GPX3) activity was measured using DNTP, and the intra- and interassay CVs were <8% and <10%, respectively. Malondialdehyde (MDA) was measured using an MDA assay kit, and the intra- and interassay CVs were 3.5% and 4.1%, respectively (TBA method, Nanjing Jiancheng Bioengineering Institute).
DNA extraction from whole blood and genotyping
DNA was isolated from whole blood using FlexiGene DNA Kits (Qiagen, Hilden, Germany). All patients were genotyped for rs7579 in the SEPP1 gene using a TaqMan Assay with a 7500 HT (Genecore Biotec, Shanghai, China).
Statistical analysis
Data analyses were performed using SPSS software (version 16.0. SPSS Inc. Cary, NJ, USA). Since serum Se, the percentage change in serum Se, and FT4 concentrations were normally distributed, a paired samples t-test and a one-way ANOVA were used for intragroup and intergroup comparisons, respectively. Since TPOAb titers, the percentage change in TPOAb, and TSH were not distributed normally, a Wilcoxon Signed Rank test was used for comparison of repeat measurements, and Mann–Whitney U tests or a Kruskal–Wallis test were used for comparisons between or among groups, respectively. A p-value less than or equal to 0.05 was considered statistically significant.
Results
Characteristics of patients
The mean age (SD) of the 364 patients enrolled in the study was 41.4 (13.1) years. All patients were female with a median UIC of 182 μg/L. Patients did not experience any adverse effects of Se treatment. There were no significant differences in age, ethnicity, or median UIC between patients in the Se group and the placebo group (Table 1).
Demographic Characteristics of Patients with Autoimmune Thyroiditis
SE, selenium; L-T4, levothyroxine.
Serum Se concentrations
Baseline Se concentrations were found to be within the reference range in all patients (group 1, 100.8 ± 19.3 μg/L; group 2, 91.6 ± 19.9 μg/L). At baseline, there were no significant differences in Se concentrations between the groups of Se-treated and placebo-treated patients (Table 2). Se concentrations in groups G1-S and G2-S significantly increased after supplementation with respect to the baseline (p < 0.01), and no changes in Se levels were observed in the placebo groups throughout the entire study. Se concentrations at 3 and 6 months in Se-treated groups (G1-S and G2-S) were significantly higher than those in the placebo groups (G1-P and G2-P, p = 0.000).
Serum Se Concentration, TPOAb Titers and Thyroid Function in Different Groups During Se Treatment
p < 0.05, ** p < 0.01 vs. baseline; ## p < 0.01 vs. 3 months after Se.
AIT, autoimmune thyroiditis; IQR, interquartile ratio; Se, selenium; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin.
In addition, there were no significant differences in Se concentrations between euthyroid patients or those with subclinical or clinical hypothyroidism at baseline (101.93 ± 24.42 μg/L, 96.75 ± 23.93 μg/L, and 91.64 ± 19.88 μg/L, respectively). Se concentrations at 3 and 6 months in both euthyroid and subclinically hypothyroid Se groups were significantly higher than in the placebo groups (p < 0.01).
The effect of Se supplementation on TPOAb titers in group 1 (subclinical AIT group)
At baseline, the median TPOAb titers were similar between the Se-treated and placebo groups. After Se supplementation, TPOAb titers significantly decreased at 3 months by 10.0% and at 6 months by 10.7% compared with baseline levels in the Se group (Table 2), whereas there were no obvious changes in the G1-P group during the whole period. The percentage change in TPOAb from baseline to 6 months was higher in the G1-S group than in the G1-P group, and the difference approached significance (p = 0.105, Table 2), but no significant difference in TPOAb titers was observed between the G1-S and G1-P groups at 3 months and 6 months after treatment.
Although group 1 was divided into 2 subpopulations according to thyroid function, euthyroidism, and subclinical hypothyroidism, for further analysis, the results were similar to those in the whole population of group 1 (Supplementary Table S1; Supplementary Data are available online at
It is noteworthy that patients in the G1-S group did not all respond to Se supplementation; 61% of patients exhibited a decrease in TPOAb at 3 months and 63% showed a decrease at 6 months. We analyzed some characteristics of the non-responders to Se supplementation. We found that they had lower TPOAb titers (724.5 vs. 1170, p = 0.003) and Se concentrations (104.7 ± 30.4 vs. 93.1 ± 18.8, p = 0.043) than the responders at baseline, but there were no significant differences between responders and non-responders to Se supplementation in terms of age and TSH levels. We also performed a correlation analysis and found no significant correlation between the TPOAb response and variation of plasma Se levels after supplementation with Se.
The effect of Se supplementation on TPOAb titers in group 2 (clinical AIT group)
At baseline, the mean TPOAb titers were similar in the Se group and the placebo group. TPOAb titers significantly decreased at 3 months and 6 months after Se supplementation compared to baseline (p = 0.005 and p = 0.007, respectively) (Table 2). In the Se group, TPOAb levels showed an overall decrease of 27.6% at 3 months and of 16.7% at 6 months after supplementation. There were no changes in the placebo groups during the whole study period.
Meanwhile, the TPOAb titer in the Se group at 3 months was lower than that in the placebo group, with a difference that approached significance (p = 0.08). However, the difference between the Se group and the placebo group disappeared at 6 months.
The effect of Se supplementation on thyroid function in the subclinical and clinical AIT groups
Serum concentrations of TSH and FT4 in both groups during the study period are presented in Table 1. There were no significant differences between the Se group and the placebo group at any time during the study.
Oxidant and antioxidant indexes
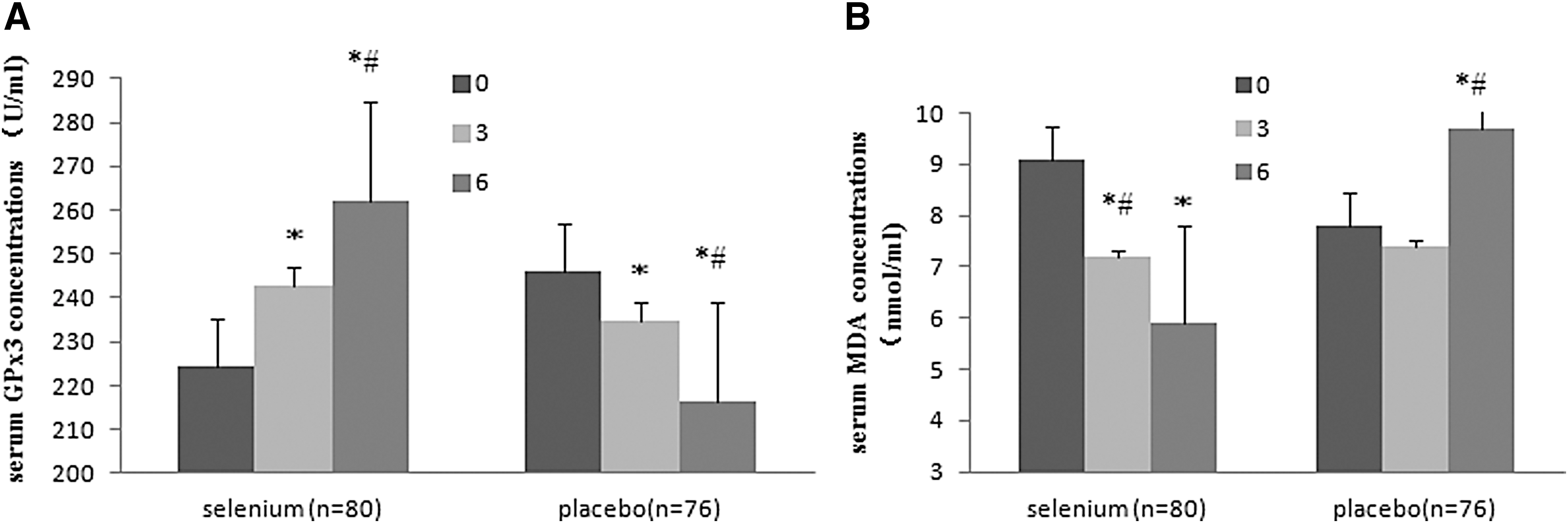
The antioxidant (GPX3 activity) and oxidant (MDA) indexes in 156 patients from Shenyang were analyzed at study entry, at 3 months after Se supplementation, and at the end of the treatment (Fig. 1).
(
There were no significant differences in GPX3 activity and MDA levels between the Se group and the placebo group at study entry. However, there was a significant increase in serum GPX3 activity in patients during the first 3 months of Se treatment (p < 0.001, n = 80). A further increase in GPX3 levels was also observed during the subsequent 3 months of Se treatment (p < 0.001, n = 80). A significant decrease in serum GPX3 activity was observed in the placebo group 6 months after placebo supplementation (p < 0.001, n = 76).
The amount of serum MDA decreased at 3 months and 6 months after Se supplementation compared with baseline (p < 0.001, n = 80), while there was a significant increase of serum MDA in the placebo group (p = 0.026, n = 76).
Characteristics of 96 AIT patients based on SEPP1 genotypes
Ninety-six patients [mean (SD) age 40.0 (12.5) years] from the Shenyang area with AIT were subjected to genotyping for SNP r25191G/A in the SEPP1 gene. The numbers of patients with euthyroidism, subclinical hypothyroidism, and clinical hypothyroidism were 52, 16, and 28, respectively. The total cohort of 96 consisted of 35 (36.5%) GG, 54 (56.2%) GA, and 7 (7.3%) AA genotypes for SNP r25191G/A, and the minor allele frequency was 35.4%. The genotype frequency deviated from Hardy-Weinberg equilibrium (HWE) (chi-squared = 5.06, p = 0.024).
Serum Se concentrations significantly increased (p < 0.05) in all genotype groups. However, there were no differences in serum Se concentrations among the 3 different genotypes at baseline, 3 months, or 6 months (Table 3).
Serum Se Concentration and TPOAb Titers in Different Genotypes of Single Nucleotide Polymorphism r25191G/A in the SEPP1 Gene
Comparison between three genotypes.
Three months vs. baseline.
Six months vs. baseline.
SNP, single nucleotide polymorphism.
Associations of the SNP r25191G/A genotype and TPOAb titers in 96 patients with AIT
At baseline, the median serum TPOAb titer of the patients was 935.5 IU/mL. Se supplementation for 3 months and 6 months decreased serum TPOAb titers to 764.0 IU/mL and 786 IU/mL, respectively, and both titers were significantly lower than at baseline (p = 0.001 and p = 0.013, respectively). There were no significant differences in serum TPOAb titers at baseline, 3 months, or 6 months among the three SNP r25191G/A genotypes. Overall, serum TPOAb titers decreased by 14.6% at 3 months and 15.9% at 6 months after Se supplementation. However, serum TPOAb titer in the subjects with the AA genotype decreased to a greater extent (by 46.2%) than in individuals with the GA and GG genotypes (by 14.5 and 9.8%) at 3 months of Se supplementation, and this difference approached significance (p = 0.070, Table 3), but the difference was not apparent at 6 months.
TPOAb titers did not decrease in 33% (31/94) and 34.2% (26/76) of subjects during 3 months and 6 months of Se supplementation, respectively. This indicates a lack of response to Se supplementation, and these patients are referred to as nonresponders. Noticeably, TPOAb titers significantly decreased after Se supplementation in all patients with the AA genotype, and none of the AA genotype patients were nonresponders. Although there were no significant differences in the proportion of responders amongst the 3 genotypes at 3 months and 6 months (p = 0.151 and 0.272), Cramer's V value was 0.201 and 0.185 respectively, which is considered as a medium effect (Table 4).
Associations of the SNP r25191G/A Genotypes in the SEPP1 Gene and the Proportion of Responders
Responders are defined as AIT patients with TPOAb decrement after Se supplementation.
Discussion
Recent intervention studies have suggested a combination of Se and L-T4 as an effective treatment in AIT. However, the exact effect of Se on AIT is as yet unclear, as is the mechanism of action. It is known that the selenoenzymes are capable of modifying cell redox status and thyroid hormone metabolism. The selenoenzymes GPx and TrxR play an antioxidative role by decreasing the formation of free radicals as well as by reducing hydrogen peroxide and lipid and phospholipid hydroperoxides, and thereby maintaining normal thyroid hormone metabolism. The intrathyroidal concentration of Se is important for the activity of these selenoenzymes. Low selenium status correlates with risk of goiter and multiple nodules in European women. A study from France showed that selenium may protect against goiter and thyroid tissue damage, and it also found a relationship between Se status and thyroid echostructure, suggesting that Se may also protect against autoimmune thyroid disease (20). A recent, large Chinese study showed that low Se status is associated with increased risk of thyroid disease; increased Se intake may reduce the risk in areas of low Se intake that exist not only in China but also in many other parts of the world (21). This suggests that Se may protect against autoimmune thyroid disease. It is assumed that even mild Se deficiency is an important environmental factor in the initiation or progression of autoimmune thyroiditis in people who are genetically susceptible to the development of organ-specific autoimmunity.
The links between Se and altered immune function and inflammation have prompted studies in humans to examine whether Se supplementation can modify autoantibody production in patients with AIT. Some clinical trials (1 –6) have shown that daily Se (selenomethionine or sodium selenite) supplementation of 200 μg produces a significant decline in TPOAb titer and a significant improvement in mood and/or general well-being. The duration of these supplementation regimens ranged from 3 to 12 months, and the TPOAb titer decreased by 11–56%. However, other studies suggest that there is no effect of Se supplementation on thyroid autoimmunity (22 –24). Several meta-analyses have come to different conclusions. A meta-analysis by Toulis et al. (7) compared four trials and concluded that routine Se supplementation in patients with Hashimoto thyroiditis is a promising adjuvant treatment option. A meta-analysis by Fan et al. (9) concluded that Se supplementation may be an effective complementary treatment for patients with AIT. A meta-analysis by Wichman et al. (11) found that Se supplementation reduced serum TPOAb levels after 3, 6, and 12 months in an LT4-treated AIT population, and after 3 months in an untreated AIT population. Whether these effects correlate with clinically relevant measures remains to be demonstrated. Two further meta-analyses by van Zuuren et al. (25) and Winther et al. (26) concluded that the evidence to support or refute the efficacy of Se supplementation in patients with Hashimoto's thyroiditis is neither complete nor reliable enough to help inform clinical decision making. Our prospective study, a randomized, placebo-controlled, double-blind trial conducted to explore the effect of Se yeast on serum TPOAb titers in patients with subclinical AIT and clinical AIT, found that the TPOAb titer significantly decreased after Se supplementation, while there was a moderate increase in TPOAb titers during the follow-up period in patients receiving placebo. Especially in clinical AIT, the degree of TPOAb decline was obvious. These results are similar with the findings of other trials.
Serum Se concentrations were within the reference range in our study, but we found that they were at the low end of the normal range. One view is that the baseline Se status of an individual is the most important parameter affecting the outcome of Se supplementation, which might disrupt the self-amplifying cycle of the endocrine–immune system interface and rectify the interaction of lymphocytes with thyroid autoantigens (27). Se deficiency is likely to constitute a risk factor for the feedforward derangement of the immune system-thyroid interaction, while Se supplementation appears to dampen the self-amplifying nature of this derailed interaction. In vitro studies have shown that Se reduces proinflammatory gene expression by increasing the formation of 15-deoxy-Δ12,14-prostaglandin J2, an inhibitor of the nuclear factor-κB cascade, and that it can suppress the expression of human leukocyte antigen-DR molecules on thyrocytes, which may reduce the development of thyroid autoimmunity (28). Moreover, any destructive inflammatory process is associated with a high level of proinflammatory cytokines, known to impair selenoprotein biosynthesis (29). Inflammatory processes occurring in the thyroid may therefore aggravate Se deficiency. In the present study, Se concentrations and GPX3 activity significantly increased after supplementation with respect to the baseline. We assume that these may play a role in oxidative defense and immune regulation by reducing the inflammatory response, but the exact mechanism of Se supplementation on AIT is still not understood.
Although it was demonstrated that Se supplementation could decrease TPOAb in patients with AIT, not all patients exhibited this decrease. A study by Duntas et al. also found that 53% of patients exhibited a marked decrease of TPOAb by 86% at 6 months, whereas 12% of patients did not show any decrease (2). Genetic factors could, in part, explain these inter-individual variations in the TPOAb titer response to Se supplementation in AIT patients. As the SEPP1 gene plays an important role in Se metabolism and the 3′ untranslated region is an essential regulatory site for gene expression, a SNP located in the 3′ untranslated region of SEPP1, rs7579, was chosen for further analysis (17). Therefore, the study cohort supplemented with Se was subjected to genotyping to determine whether this SNP plays a role in the response to Se supplementation. We found that genotype frequencies in this population supplemented with Se deviated from HWE. A SNP may be associated with a common disease when its allele frequencies deviate from HWE in a relatively small sample of patients (30). Thus, we speculate that there may be an association between rs7579 and the occurrence of TPOAb positivity and AIT. Several past studies have reported that rs7579 is associated with a variety of diseases and biological parameters, such as prostate cancer (31), aortic diseases (32), and the insulin sensitivity index (33). In the future, case-control studies may be needed to determine a possible association between rs7579 and thyroid autoimmune status.
In previous studies, it was shown that rs7579 affects selenoprotein activity in lymphocytes as well as the response of SEPP1 to Se supplementation (17). A recent study reported that the SNP rs3877899 in the SEPP1 gene, in combination with rs7579, is associated with changes in Se status during pregnancy and in GPX3 activity after Se supplementation (34). Moreover, Meplan et al. have reported that rs7579 affects the 60 kDa isoform of SEPP1 in plasma. Given that this isoform contains more selenocysteine residues, it could modulate the availability of Se, thereby facilitating selenoprotein synthesis (35). It has also been noted that the proportion of the 60 kDa isoform is greater in the presence of the A allele than the G allele (36). In our study, we found that TPOAb titers decreased to the greatest extent after Se supplementation in the AA genotype compared with the GA and GG genotypes. Additionally, 100% of AA individuals showed an obvious decrease in TPOAb titers after Se supplementation, whereas only around 60% of GA and GG individuals did. Despite our finding that polymorphisms in the SEPP1 gene may be associated with the effect of Se supplementation on TPOAb titers, our study has some limitations. It is a preliminary study, and only participants from a single center were genotyped. The small sample size is a further limitation, since the results simply demonstrate an association rather than a definite causal relationship. Therefore, multicenter studies with large sample sizes need to be conducted to further confirm the results of this study.
In conclusion, Se supplementation significantly reduced TPOAb titers in patients with AIT. This may be partly explained by changes in antioxidant capacity, and there may be a genetic component that influences interindividual differences in the extent to which TPOAb titers change in response to Se supplementation.
Footnotes
Acknowledgments
We are indebted to those patients who participated in this study and gratefully acknowledge the help of doctors from the First Affiliated Hospital of China Medical University, Hospital of Shandong Province, the General Hospital of the People's Liberation Army, Second Affiliated Hospital of Zhongshan University, and the First Hospital of Dalian Medical University.
The study was supported by the National High Technology Research and Development Program of China (863 Program, No. 2007AA02Z4Z1), National Science Foundation of China (No. 81200571), Research Fund for the Doctoral Program of Higher Education of China (No. 20122104120001), and Natural Science Foundation of Liaoning Province (No. 201202293).
Author Disclosure Statement
We hereby confirm that this manuscript has not been published and is not being considered for publication elsewhere. Each of us acknowledges that he or she participated sufficiently in the work to take public responsibility for its content. We state that we have no potential conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.