
Abstract
Background:
Tall-cell variant (TCV) is widely believed to be a more aggressive subtype of papillary thyroid carcinoma (PTC). Despite the significance of TCV with respect to risk stratification and therapeutic decision making, its diagnosis is subject to inter-observer variability. This study aimed to determine the level of agreement among expert pathologists in the identification and reporting of TCV.
Methods:
Seventeen surgical resections for thyroid cancer containing the diagnostic term “tall cell” in their pathology reports and 22 cases diagnosed as classical PTC were selected. Cases were digitalized, and 14 expert pathologists reviewed the scanned slides blinded to the original interpretation. Each pathologist designated each case as TCV or not and answered multiple questions about diagnostic histopathologic features of TCV.
Results:
The overall strength of agreement for identifying TCV was fair (Fleiss kappa 0.34), and the proportion of observed agreement was 0.70. Of 22 cases originally diagnosed as PTC classical variant, 15 (68%) were reclassified as TCV by at least one expert pathologist. It was noted that four different definitions for TCV were used by the participants based on various combinations of cell height to width (H:W) ratio and the percentage of tumor cells showing that specific ratio. All pathologists agreed that the diagnosis of TCV does not rely solely on a specific H:W ratio.
Conclusions:
Pathologic reporting of TCV varies among pathologists. This disagreement is a result of the lack of unanimous diagnostic criteria and variation in individual pathologists' interpretations. These discrepancies lead to over- and under-diagnosis of TCV, which has significant implications in patient management. It is imperative to understand this variability in diagnosis TCV as it relates to risk stratification and interpretation of clinical studies related to this histologic subtype of PTC. Further studies are needed to reach consensus on the diagnostic criteria of TCV.
Introduction
T
Prior studies have shown that the identification of histological prognostic factors in PTC (i.e., extrathyroidal and extranodal extension) suffers from inter-observer variability (3,4). Thus, this study aimed to determine the level of agreement among expert pathologists in the identification and reporting of TCV. Moreover, the study strove to identify areas for improvement in the clinical interpretation and pathological assessment of this variant of PTC typically regarded to be aggressive.
Methods
After Institutional Review Board approval, 17 surgical thyroid resections containing the diagnostic term “tall cell” (i.e., TCV or tall-cell features) in their pathology reports and 22 cases diagnosed as classical PTC were selected. The classic PTC cases were selected randomly, and none of them contained the diagnostic term “tall cell” in their reports. All 39 cases originated from the pathology department of Mount Sinai Beth Israel from 2004 to 2015, and all resections were performed by one surgeon. All available hematoxylin and eosin–stained slides were reviewed, and 89 representative slides from the primary tumor were selected (average of two slides per case). The slides were de-identified and digitalized using a Pannoramic 250 Flash III scanner (3DHISTECH Ltd.) at 40 × magnification. The scanned slides were sent out through hard drives to the participating pathologists, and the cases were reviewed on CaseViewer 2.1 (3DHISTECH Ltd.).
Fourteen board-certified pathologists from the United States and Canada with subspecialty expertise in thyroid pathology reviewed the scanned slides and were blinded as to the original histological interpretation. Each pathologist was required to answer multiple questions about diagnostic histopathologic features, the first being whether they designated each case in the cohort as TCV (Table 1).
TCV, tall-cell variant.
Data were collected and analyzed. A Fleiss generalized kappa coefficient for determining reliability among multiple rates was calculated to evaluate the agreement of TCV between the participating pathologists. All Fleiss kappa coefficient calculations were performed on a freely downloadable Microsoft® Excel spreadsheet (
A review limited to English literature to tabulate the historical evolution of TCV was performed. Studies were included if at least one of the authors was a pathologist and if a histological definition of TCV was provided. Meta-analysis and population-based studies were excluded. Key reference books such as the Classification of Endocrine Tumors of the World Health Organization were also included in the literature review.
Results
The overall strength of agreement for identifying TCV was fair (Fleiss kappa 0.34), and the proportion of observed agreement was 0.70. Out of the 39 cases, unanimous agreement for TCV was reached in only two (5%) cases. Of 22 cases originally diagnosed as PTC classical variant, 15 (68%) were reclassified as TCV by at least one expert pathologist. Among the original cases containing the diagnostic term “tall cell,” the individual rates of diagnosing TCV ranged from 29% to 82% by expert pathologists. (Supplementary Table S1 shows which cases were designated as TCV by the 14 expert pathologists; Supplementary Data are available online at
It was noted that four different definitions for TCV were used by the expert panel based on the various combinations of cell height to width (H:W) ratio and the percentage of tumor cells showing that specific ratio (Table 2). Eleven (79%) considered a cell to be “tall” if its height was at least three times (3:1) its width (Fig. 1). Among those pathologists, six designated a tumor as TCV if it was comprised of ≥30% tall cells, while five employed the threshold of ≥50%. A H:W ratio criteria of 2:1 (Fig. 2) was used by three panelists, and the tall-cell cutoff value was ≥50% for two and ≥30% for one.
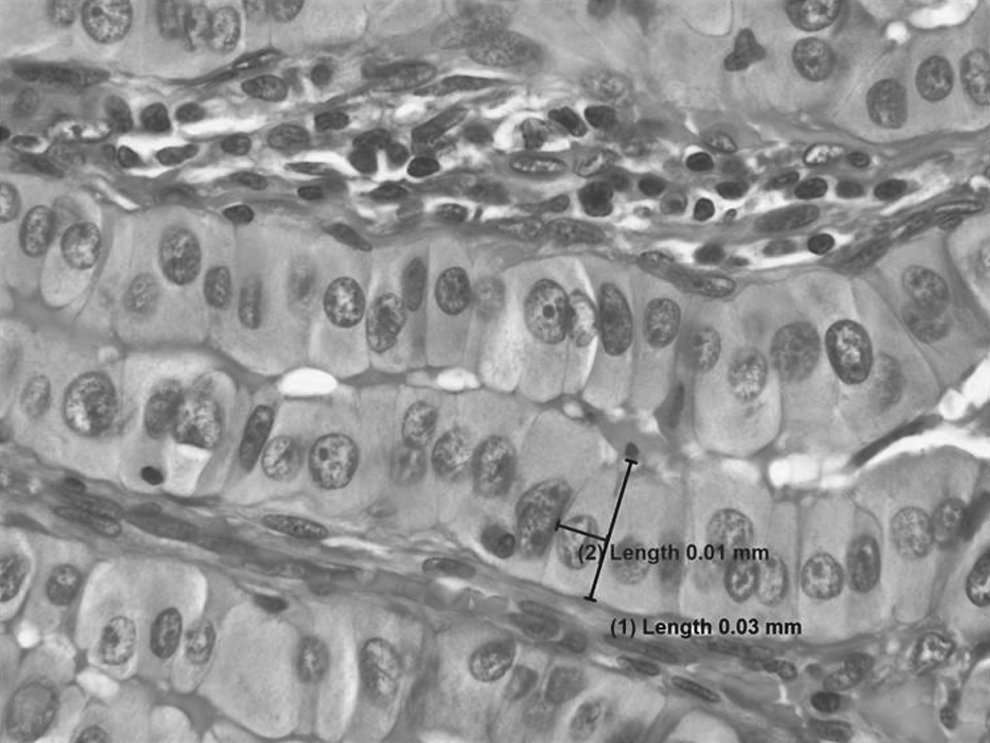
“Tall” cell showing a height (0.03 mm) three times its width (0.01 mm). Measurements obtained using Olympus cellSens Standard software at 60× magnification (hematoxylin and eosin [H&E] stained slide).
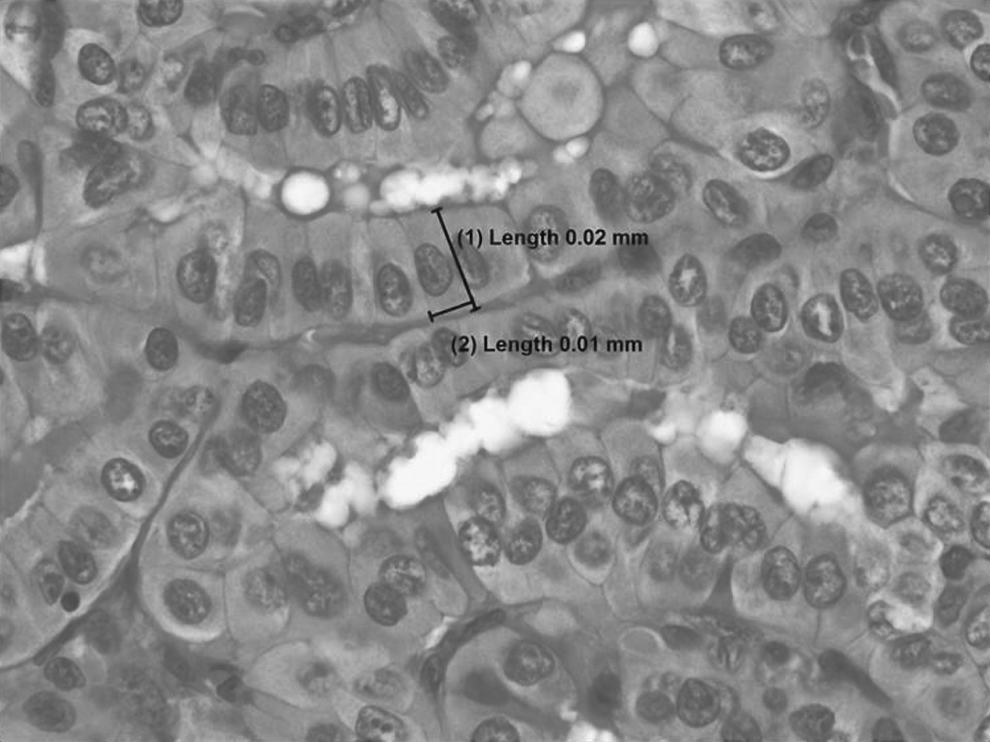
“Tall” cell showing a height (0.02 mm) two times its width (0.01 mm). Measurements obtained using Olympus cellSens Standard software at 60× magnification (H&E stained slide).
Since different definitions for TCV were utilized by the participants, the strength of agreement among the two groups with more pathologists (C and D) was also calculated. When using definition C, the inter-observer agreement was fair (Fleiss kappa: 0.32), while the agreement amount group D was moderate (Fleiss kappa: 0.46).
In addition to the H:W ratio and the percentage of tumor cells showing that specific ratio, all pathologists unanimously answered that they use other histological features to identify TCV. Elongated “tram-track” follicles, eosinophilic cytoplasm with distinct cell borders, and prominent/exaggerated nuclear features of PTC were consistently listed by the participants as histological diagnostic criteria necessary for TCV (Fig. 3A–C). It was also noted that the histological features of TCV varies, depending on the plane of sectioning of the tumor (Fig. 3D). None of the panelists reported the use of ancillary studies for the diagnosis of TCV, except one, who mentioned that the immunohistochemical reactivity for BRAFV600E is typically seen in TCV.
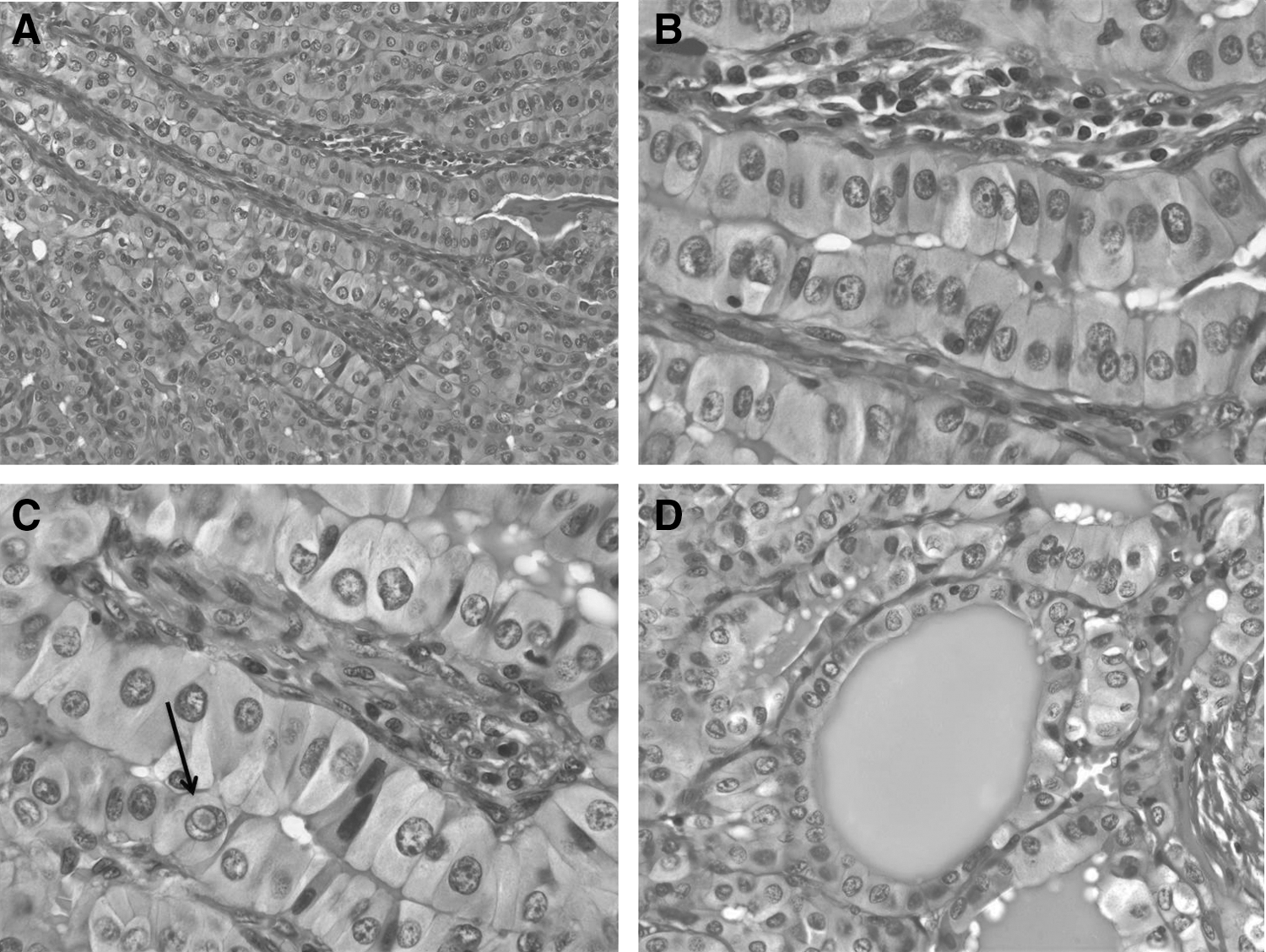
Additional histological features of tall-cell variant (TCV) of papillary thyroid carcinoma (PTC). (
All panelists reported using the terminology PTC with tall-cell features (TCF) when a tumor composed of tall cells did not reach their percentage criteria. When the latter scenario is encountered, five participants mentioned that, in addition, they document in the pathology report the approximate percentage of tall cells present in the tumor. Moreover, one pathologist reported using the term PTC with TCF only when the tumor is comprised of 30–50% of tall cells.
Table 3 shows selected articles and key reference books showing the evolution of the histological definition of TCV.
PTC, papillary thyroid carcinoma; ETE, extrathyroidal extension; TCF, tall-cell features.
Discussion
This study highlights the lack of agreement in the identification and reporting of TCV of PTC among expert pathologists, which has important clinical implications. According to current ATA clinical practice guidelines, a diagnosis of TCV places patients in an “intermediate risk” category for which radioactive iodine (RAI) adjuvant therapy should be considered (1). Consequently, depending on the pathologist, a given patient may or may not be advised to undergo additional therapy. The impact can be significant in patients with PTC who undergo lobectomy alone as their initial surgical procedure and who lack other histological features of the intermediate risk category (microscopic extrathyroidal extension [ETE], vascular invasion, more than five pathologic N1 with all involved lymph nodes <3 cm in largest dimension).
Diagnostic histopathology of thyroid tumors is inherently variable due to subjective in interpretation by pathologists. Multiple studies have demonstrated this to be an intrinsic and inevitable phenomenon in the field of thyroid pathology (3 –6). Thus, poor diagnostic agreement for the identification of TCV is in part secondary to individual pathologists' interpretative thresholds. In addition, it is evident from this study that despite the known prognostic significance of TCV, no consensus diagnostic criteria have been established by pathologists. The four different definitions used by the participants reflect the historical evolution of TCV (Table 3).
TCV of PTC was first characterized as a distinct and aggressive variant by Hawk and Hazard in 1976. However, descriptions of PTC with tall-cell morphology in the literature date back to 1948 (7,8). In their seminal article on the many histological appearance of PTC, Hawk and Hazard introduced the concept that a tall cell exhibits a height at least twice its width (8). During the 1980s and 1990s, different publications using the same H:W ratio proposed by Hawk and Hazard perpetuated the idea that TCV is a more aggressive subtype of PTC (9 –12). A source of confusion was created in the late 1990s, when studies started utilizing a 3:1 ratio as the defining H:W ratio for classification as a tall cell (13). The 3:1 ratio was later adopted by the 2004 World Health Organization (WHO) classification (14). Since then, studies have used either a 2:1 or a 3:1 ration to define a tall cell (15 –19). These ratios are typically not derived by quantitative measurement, but rather by the subjective architectural and morphological appearance to the pathologist. Additionally, there is marked variability in the literature with regard to the proportion of tall cells needed to designate a PTC as TCV ranging from 30% to “virtually all tumor” among different publications (813,15 –19). The criteria proposed by the upcoming WHO classification strives to meet consensus and indicates that TCV is composed of >30% of cells that are two to three times as tall as they are wide (20).
All participants in this study consistently use the term TCF when a tumor demonstrates features of tall cells but does not reach their cutoff percentage criteria. However, the definition of TCF is more nebulous than the one of TCV, and few studies have addressed its clinical significance (13,17 –19). Ganly et al. defined as TCF as a tumor harboring between 30% and 50% tall cells, and showed that TCF and TCV have similar clinicopathologic features (18). Nevertheless, the TCF threshold proposed by Ganly et al. falls into the TCV category by other authors. In addition, three publications have shown that tumors that demonstrate as little as 10% of tall cells behave aggressively (17,19,21).
It should be appreciated that the percent of the volume of a tumor that is considered to be composed of tall cells is also an estimate, since most studies have used visual determinations based on representative sections of a lesion. Currently, there are no guidelines addressing the amount of thyroid tumor that needs to be submitted for histological evaluation. Tumor sampling varies from institution to institution, with some submitting lesions in toto, but many, if not most, examine only representative sections. Therefore, in this study, as well as in general practice, the 30% or 50% cutoff was applied to the sampled tumor and not to the entire tumor volume.
Importantly, as highlighted by all participants, the designation “tall cell” is not limited to a specific H:W ratio and percentage criteria. Other histological diagnostic criteria are necessary for the diagnosis of TCV, including elongated “tram-track” follicles, eosinophilic cytoplasm with distinct cell borders, and prominent/exaggerated nuclear features of PTC. These features have not received enough attention as defining criteria and are necessary for the histological diagnosis of TCV (22). It is particularly important to distinguish TCV from the oncocytic variant of PTC, as studies have shown that oncocytic variant of PTC is not more aggressive than conventional PTC (23,24). In contrast to the TCV, the cells in the oncocytic variant of PTC tend to have a more intensely granular eosinophilic cytoplasm, are typically not two to three times tall as wide, do not consistently have distinct cell borders, and lack elongated “tram track” appearing follicular growth pattern. Consequently, careful and accurate measure of cell height and width is needed to overcome this dilemma.
Independent of definition, multiple studies have reinforced the widespread consensus that TCV has a worse prognosis compared to classic PTC (8 –13,16 –19). Even meta-analysis and a population study using Surveillance, Epidemiology, and End Results data that did not control for strict histological inclusion criteria have shown that TCV is associated with older age at presentation, higher frequency of ETE (both gross and microscopic), and lymph node and distant metastases (25 –27). It is important to note that this concept has been challenged. Some publications have also shown that when age and ETE are controlled for, TCV did not alter prognosis (15,28). These conflicting and opposing outcome data, which have brought into question the true clinical significance of TCV, can in part be explained by the findings that identification and reporting TCV is inconsistent and dependent on individual pathologist's criteria. Therefore, it has to be acknowledged that the prognostic significance of TCV is not definitively settled, and better outcome studies based on stringent diagnostic criteria and standardized reporting are necessary. It is beyond the scope and the design of this study to correlate the findings with clinical outcome. The cases were selected randomly and have short follow-up. In addition, the marked inter-observer variability and lack of unanimous diagnosis criteria for TCV would have represented a major confounding source in any analysis relative to outcome.
It is evident that there are many obstacles for the consistent identification and reporting of TCV. Consequently, endocrinologists and thyroid surgeons should be aware of the lack of agreement among pathologists in diagnosing TCV while interpreting clinical studies as well as individual patient pathology reports. Current clinical guidelines for PTC follow linear and binary pathways that do not take into consideration the ambiguity and uncertainty of the practice of thyroid histopathology. For example, in the discussion of aggressive variants of PTC in the 2015 ATA guidelines, there is no mention as to the variability in the definition of TCV. Furthermore, there are no specific recommendations for the clinical management of cases diagnosed as showing TCF (1).
Pathological examination of thyroid resections provides the foundation upon which most postoperative clinical decisions are formulated. Therefore, it is imperative that surgical pathologists recognize the significance of TCV with respect to risk stratification and therapeutic decision making. For a number of years, the College of American Pathologist (CAP) has made enormous improvements in the development and implementation of a protocol for the examination of specimens from patients with thyroid cancer (29,30). CAP synoptic protocols have achieved standardization in the terminology among pathology reports. Unfortunately, the CAP thyroid cancer protocol cannot solve the variation in pathologists' interpretation and lack of unanimous diagnostic criteria for TCV. However, the CAP could recommend that pathologists include in their reports the H:W ratio and tumor percentage criteria that they used to render the diagnosis of TCV. This may allow for important data collection and analyses that might justify a practice change in the future.
Regardless of great advances in the understanding of molecular pathogenesis of PTC, as of today, the diagnosis of TCV relies exclusively on conventional light microscopy. Data from The Cancer Genome Atlas (TCGA) has shown that most TCVs cluster together at the mRNA level and have a distinct molecular signature, including the highest frequency of BRAFV600E mutations (78%) and miR-21 expression (31). In addition, studies have shown that TERT promoter mutations significantly correlated with tall-cell morphology (21). This potential phenotypic–genotypic correlation opens different possibilities for the integration of molecular testing in the diagnosis of TCV.
Digital microscopy has advantages over the human eye in the identification and quantification of specific features in whole-slide images. Utilization of image analysis could represent a feasible solution to achieve agreement in the identification and reporting of TCV. Consequently, a computer-assisted approach could be developed to identify precisely all histological features necessary for the diagnosis of TCV. However, with the advent of digital pathology, tumor sampling will remain an issue.
Conclusion
Currently, the gold standard for the identification of TCV is histopathologic evaluation and interpretation of thyroid resection specimens. As reported in this study, this method is subject to significant inter-observer variability. In addition, there is no consensus as to the diagnostic criteria for TCV among pathologists. It is imperative for clinicians to understand this variability in interpretation and lack of concordance in reporting of thyroid surgical pathology specimens as it relates to specific patient care, as well as the implications for interpreting clinical studies related to this histologic subtype of PTC. Likewise, it is critical for surgical pathologists to recognize the significance of TCV with respect to risk stratification and therapeutic decision making. In addition, this study emphasizes the fact that TCV is more than just a specific H:W ratio. Future studies are envisioned that integrate data derived from stringent histological criteria, image analysis, molecular testing, and clinical outcomes in order to standardize the diagnosis, elucidate the real prognostic significance, and optimize the management of TCV of PTC.
Footnotes
Acknowledgments
The authors would like to thank the Head and Neck Surgery, Thyroid, Head and Neck Cancer (THANC) Foundation, and Mount Sinai Health System for its generous support of this research project; the Biorepository and Pathology Core at the Icahn School of Medicine at Mount Sinai for scanning the slides; and Ryan Starling (Moffitt Cancer Center) for outstanding secretarial support.
Author Disclosure Statement
The authors have nothing to disclose.