
Abstract
Introduction:
Whether pediatric patients with differentiated thyroid carcinoma (DTC) are at risk of developing treatment-related adverse effects on cardiac function is unknown. We therefore studied in long-term survivors of pediatric DTC the prevalence of cardiac dysfunction and atrial fibrillation in relation to treatment variables, and the association between cardiac dysfunction and plasma biomarkers.
Methods:
In this nationwide prospective multicenter study, cardiac assessments were performed in 66 adult survivors of pediatric DTC (age at diagnosis ≤18 years and follow-up ≥5 years after diagnosis) treated in the Netherlands between 1970 and 2009. Assessment included echocardiography, plasma biomarkers (N-terminal pro-brain natriuretic peptide, high-sensitive troponin-T, galectin-3), and 24-hour Holter electrocardiography. Echocardiographic measurements were compared with retrospective data of 66 sex- and age-matched unaffected Dutch controls. Diastolic dysfunction was defined as an early diastolic septal and/or lateral tissue velocity (e′) less than 2 SD of mean age-adjusted reference data.
Results:
The survivors (86.4% women) had at DTC diagnosis a median age of 16 years. Median follow-up was 17 years. Left ventricular ejection fraction <50% was found in one survivor, and median global longitudinal systolic strain was near normal. Diastolic dysfunction was present in 14 asymptomatic survivors (21.2%). Overall, diastolic function of survivors was lower compared with controls (e′mean 14.5 versus 15.8 cm/s, P = 0.006). Older attained age and higher waist circumference were associated with decreased diastolic function, whereas thyrotropin levels and cumulative administered radioiodine dose were not. In survivors, biomarkers were not associated with diastolic dysfunction; atrial fibrillation was not observed.
Conclusion:
While systolic function is unaffected, diastolic dysfunction is frequently observed in asymptomatic long-term survivors of pediatric DTC, which may suggest early cardiac aging.
Introduction
P
Late cardiac effects of treatment in survivors of pediatric DTC have yet to be assessed. Detailed insight into possible late adverse events is needed to improve treatment guidelines and follow-up strategies in the still growing population of survivors of pediatric DTC. We therefore studied: (i) the prevalence of cardiac dysfunction in long-term survivors of pediatric DTC in relation to treatment variables including TSH level during follow-up, (ii) the association between cardiac dysfunction and plasma biomarkers (N-terminal pro-brain natriuretic peptide (NT-proBNP), high-sensitive troponin-T (hs-troponin-T), galectin-3), and (iii) the prevalence of AF in this patient group.
Patients and Methods
Study design and population
This study is part of a nationwide Dutch study on pediatric DTC, previously described in detail (12). For this study on cardiac endpoints, subjects who met the following inclusion criteria were invited to participate: (a) PTC or FTC diagnosed between January 1970 and August 2009; (b) age at diagnosis ≤18 years; (c) age at cardiac evaluation ≥18 years; (d) treatment in the Netherlands; and (e) surviving at least five years after diagnosis. Exclusion criteria were a history of other malignant disease prior to DTC diagnosis, pregnancy at time of evaluation, and thyroid hormone withdrawal or recombinant human TSH stimulation <3 months before evaluation. Reference data for echocardiography were derived from the recommendations of the American Society of Echocardiography (13 –15). Echocardiographic measurements were also compared with those of an external control group, derived from another Dutch cohort study that included unaffected siblings of childhood-cancer survivors. Each survivor was matched with a control subject based on sex and, as best as possible, age at time of cardiac assessment. Details on the methodology of the control group are described elsewhere (16). The Institutional Review Board of the University Medical Center Groningen approved the study. Written informed consent was obtained from all subjects. Assessments of survivors were performed between November 2012 and September 2014 and included medical history, a health and risk factor questionnaire, a physical examination, echocardiography and blood sampling. Assessments of controls were performed between August 2004 and April 2007.
Clinical and cardiac examinations
A single physician (M.K.H.) performed the physical examinations. Echocardiographic image acquisition was performed locally according to a pre-specified image acquisition protocol. Images were stored digitally in Digital Imaging and Communications in Medicine format for offline central analysis at the Groningen Imaging Core Laboratory on an EchoPac analysis system, software version BT12 (General Electric, Horton, Norway). Echocardiographic evaluation consisted of LV dimensions and volumes. Where appropriate, results were indexed for body surface area. Assessment of LV systolic function consisted of LV ejection fraction (LVEF), according to Simpson's biplane method of discs. When image quality was insufficient for reliable endocardial border definition, the LVEF was estimated (so called “eyeballing LVEF”). Systolic dysfunction was defined as a LVEF <50% (17). In addition, global longitudinal systolic strain (GLSS), which is a sensitive tool to measure myocardial deformation, was evaluated as a measure for systolic LV function. GLSS measurements were performed by two experienced operators (Y.H. and F.B.), independently of each other, using two-dimensional speckle tracking technique. The mean of both GLSS measurements was taken for analysis. GLSS was measured at the apical two-chamber, four-chamber, and long-axis views and was derived from the average of 18 segmental peak systolic strain values (i.e., six segments for each apical view). If more than one segment could not be measured accurately, the longitudinal strain measurements were not included in the analysis. Strain measurements were available only for the survivors. Assessment of LV diastolic function consisted of transmitral inflow measurements (early and late mitral valve inflow, deceleration time, and isovolumetric relaxation time), and early diastolic tissue velocities. Diastolic dysfunction was defined as an early diastolic septal and/or lateral tissue velocity (e′) less than 2 SD of mean age-adjusted reference data (13). Early diastolic tissue velocities of the survivors were measured using pulsed-wave tissue Doppler Imaging (PW-TDI), while in the control group color-coded TDI (CC-TDI) was used (16). E′ values were converted as follows: e′(PW-TDI) = 1.25 + 1.17 × e′(CC-TDI) (18). E′ mean was calculated as the mean of septal and lateral e′. Finally, right ventricular (RV) systolic function was assessed with tricuspid annular plane systolic excursion (TAPSE) among the survivors. The operator who performed the echocardiographic measurements in the survivors also performed these measurements in the control group.
Electrocardiographic evaluation consisted of 24-hour Holter electrocardiography (ECG) monitoring using an ambulatory Seer Light Extend recorder. Analysis was performed centrally by a single certified analyst (J.R.) using MARS analysis software (General Electric). Operators were blinded for medical characteristics of the survivors for both echocardiographic and electrocardiographic evaluations.
Laboratory measurements
Fasting blood samples of the survivors were collected concomitantly with the cardiac assessments. The following biomarkers were selected: NT-proBNP, a sensitive marker to exclude heart failure, hs-troponin-T, a marker of cardiac damage, and galectin-3, a cardiac fibrosis marker (19–20). Measurements of cardiac biomarkers and TSH were performed at a central laboratory (University Medical Center Groningen). TSH, NT-proBNP and hs-troponin-T were measured in serum with an electrochemiluminescence immunoassay according to a sandwich principle on a Modular E170 immunoassay analyzer (Roche Diagnostics, Mannheim, Germany). Galectin-3 was measured in EDTA-plasma using a chemiluminescent sandwich based microparticle immunoassay on an Architect immunoassay analyzer (Fujirebio Diagnostics Inc, USA for Abbott Laboratories, Wiesbaden, Germany). The reference range for TSH was 0.5 to 4.0 mU/L. NT-proBNP ≥125 ng/mL, hs-troponin ≥14 ng/L, and galectin-3 ≥ 17.8 ng/mL were considered clinically relevant.
Study definitions
Medical history, diagnosis, and treatment details were obtained from survivors' medical records, as recently described in detail (12). Follow-up was calculated from the date of diagnosis until the date of the patient's last known assessment. In all survivors, last assessment was the study visit with cardiac evaluation. All available historical TSH values were collected from the laboratory reports. Blood pressure was measured on both arms with subjects in sitting position in a quiet room at the time of the clinical visit. The mean of left and right arm measurements was used for analysis. Survivors were classified as having hypertension on the basis of a systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, and/or the use of antihypertensive drugs. The waist circumference was measured both at the point of the smallest circumference of the abdomen and at the midpoint between the top of the iliac crest and the lower margin of the last palpable rib. For analysis, we took the mean of both measurements. All measurements were done by the same person (M.K.H.). Diabetes mellitus was defined as fasting blood glucose level >7.0 mmol/L and/or the use of glucose lowering medication. Hypercholesterolemia was defined as fasting cholesterol >6.5 mmol/L and/or use of lipid-lowering medication. History of cardiovascular disease was defined as coronary artery disease, peripheral artery disease, abdominal aorta aneurysm, or cerebrovascular disease. History of AF was defined as documentation of this condition and/or prescription of antithrombotic drugs for this condition. Smoking status was obtained from a questionnaire completed by the survivor. Current AF was defined as AF present during 24-hour Holter ECG monitoring.
Statistical analysis
Data are presented as mean plus or minus standard deviation, geometric mean, or median and range. Groups were compared using chi-square or Fisher's exact tests (if conditions for chi-square test were not met) in case of categorical variables. T-tests were performed for normally distributed continuous variables. Mann-Whitney U tests were performed for non-normally distributed continuous variables. Missing or unknown values were excluded from statistical testing. The TSH level for each year of follow-up was expressed as the geometric mean of all eligible TSH values during that year as previously described (12). The TSH value measured as part of this study was included in the calculation of the TSH level during the last year of follow-up. The TSH level during the entire follow-up was defined as the overall geometric mean of the calculated TSH levels per year (7,12). For the survivors, a univariate linear regression analysis of the association between each treatment modality with diastolic function, expressed as e′mean (the mean of septal and lateral e′), was succeeded by a multivariate regression analysis. In this analysis, we entered the variables of which we considered the associations with cardiac outcome measures to be biologically plausible and/or the variables which were associated (p < 0.10) with diastolic function in univariate analyses. The model was subsequently reduced to the variables remaining significant in multivariate analysis (p < 0.05). All tests were two sided. A p-value of <0.05 was considered statistically significant. IBM SPSS Statistics version 22 for Windows (IBM, Armonk, NY) was used for statistical analyses.
Results
Characteristics of survivors and controls
As shown in the study flowchart (Fig. 1), 74 of the 105 survivors of pediatric DTC included in our previous study were eligible for participation in the present study. Of this group, 66 (89.2%) survivors agreed to participate in the echocardiographic evaluation, and 65 of them also underwent a 24-hour Holter ECG. Cancer-related characteristics are provided in Table 1. Median follow-up was 17 years (range 5 to 43 years). Most survivors had a history of PTC (83.3%); the remaining 16.7% had FTC. All survivors had undergone total thyroidectomy and 64 (97.0%) of them received radioiodine as ablation therapy and/or during follow-up. Median cumulative radioiodine activity administered during initial treatment and follow-up was 5.81 GBq (1.22 to 35.15 GBq). Of all survivors, both historical TSH values and TSH levels at time of cardiac evaluation were available for analysis. Median (geometric mean) TSH level during follow-up was 0.17 mU/L (range 0.02 to 2.84 mU/L). TSH was suppressed to below 0.10 mU/L during the entire follow-up in 21 survivors (31.8%). Median TSH at evaluation was 0.25 mU/L (range 0.01 to 14.6 mU/L). As shown in Table 2, the majority of survivors (86.4%) were female. Median age at cardiac evaluation of the survivors was 33 years (range 19 to 60 years), whereas the controls were aged 28 years (range 19 to 51 years) at evaluation (p = 0.027). Heart rate was significantly lower in survivors as compared with controls (p = 0.003). Survivors had a significantly higher fasting glucose (mean 5.0 vs. 4.5 mmol/L, p < 0.001). However, none of the survivors or controls had diabetes mellitus. Two (3.0%) survivors vs. no controls had hypercholesterolemia. Hypertension was present in 9 (13.9%) survivors and 4 (6.1%) controls (p = 0.144). Finally, survivors were more often non-smokers as compared with controls (p = 0.017).
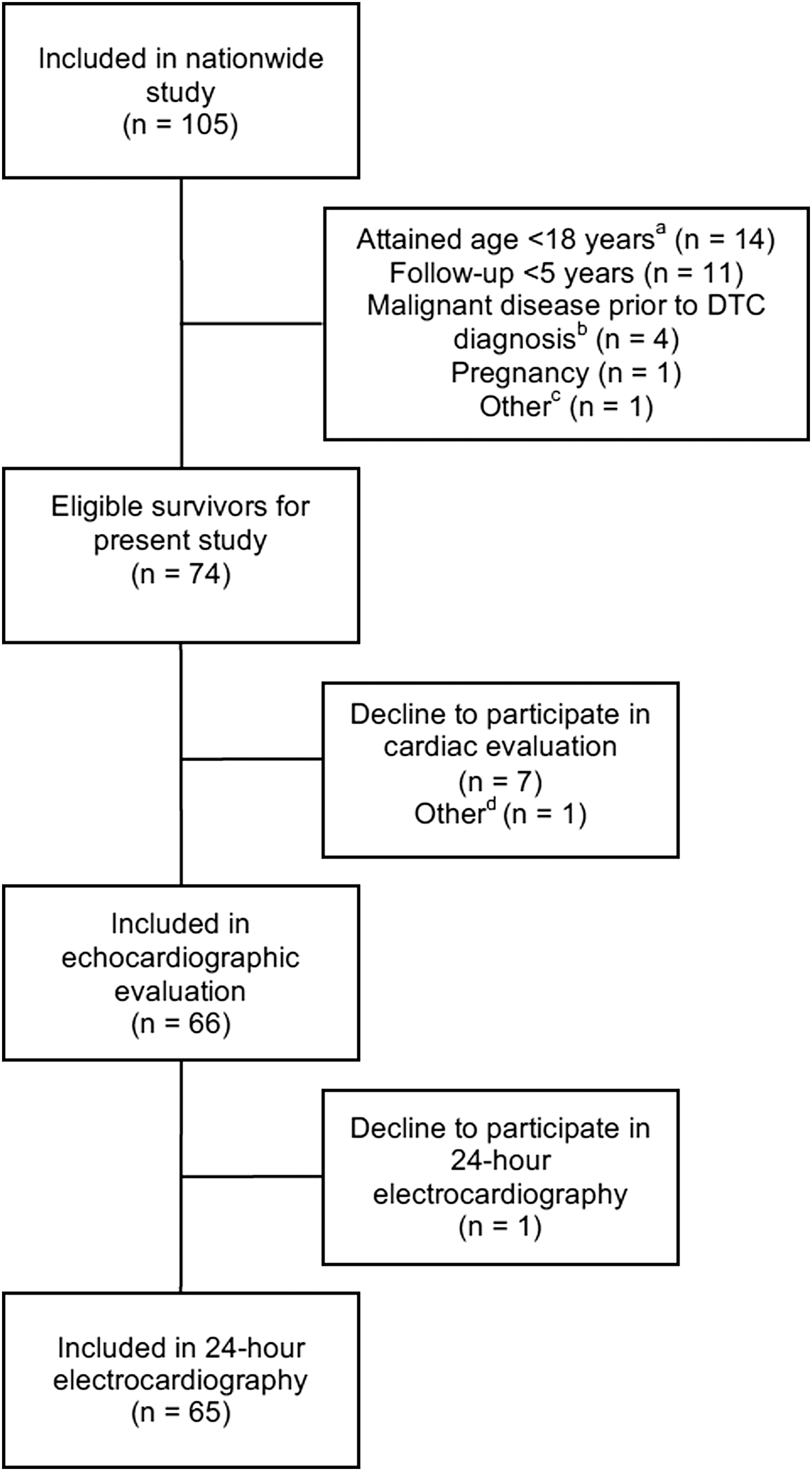
Study flow chart, showing final number of included survivors, reasons for noneligibility for the present study of subjects who participated in the nationwide project (12), and reasons for nonparticipation of eligible survivors. DTC, differentiated thyroid carcinoma. a12 survivors aged <18 years at evaluation had a follow-up <5 years. They were registered as attained age <18 years. bOne survivor <18 years at evaluation had a malignant disease prior to DTC diagnosis. He was registered as malignant disease prior to DTC. cOne survivor was excluded because of supposed malignancy prior to DTC. She gave informed consent for medical chart evaluation as part of the nationwide study. When her medical charts were reviewed, it was found that she was irradiated to the neck because of a benign condition. dOne survivor sent her informed consent after the closure date for the cardiac evaluation.
Radioiodine (131I) administration within 6 months after initial treatment.
Administered 131I activity during initial treatment and follow–up; activity unknown in 1 survivor, and 2 survivors did not receive 131I treatment. Therefore, n = 63 instead of n = 66.
One survivor received radiotherapy directed to the neck for a benign condition prior to DTC diagnosis.
DTC, differentiated thyroid carcinoma.
Fasting blood glucose missing in three survivors and three controls.
In one survivor blood pressure was measured on the right arm only; this measurement was taken for analysis.
Echocardiography
Echocardiographic results are presented in Table 3. LV mass index and left atrial volume index (LAVI) were comparable in survivors and controls. Regarding LV systolic function, median LVEF of survivors and controls was 58.8% (range 48.0 to 73.0%) and 60.0% (range 44.0 to 65.0%), respectively. In 11 survivors (16.7%) an eyeballing (estimated) LVEF was determined. One survivor had a LVEF <50%, while 5 controls had a LVEF <50% (p = 0.109). Using sex-specific reference values from the American Society of Echocardiography, one (11.1%) male survivor and one male control had a LVEF <52% (p = 1.000), and 6 (10.5%) female survivors, and 13 (23.6%, 2 missing) female controls had LVEF <54% (p = 0.065) (14). GLSS was available for 19 survivors. Median GLSS was −19.6% (range −24.2 to −17.6%). A GLSS of −18% is considered the lower limit of the normal range for the equipment and software used in this study. Two survivors (10.5%) had a GLSS > −18%, namely a GLSS of −17.6% and −17.7%, respectively, suggesting (near) normal systolic function in the survivors (14). Median TAPSE, which represents a measure of RV systolic function, was 25.0 mm (range 17.0 to 33.7 mm) (14). TAPSE values suggestive of RV dysfunction (i.e., <17.0 mm) were not observed.
Left ventricular mass calculated with Devereux formula.
Left atrial volume index available for 56 survivors and 15 controls.
Left ventricular ejection fraction could not be measured in 3 controls.
Isovolumetric relaxation time available for 55 survivors and all controls.
E/A ratio, ratio early diastolic mitral valve inflow to late diastolic mitral valve inflow; E/e′ ratio, ratio early diastolic mitral valve inflow to mean of septal and lateral early diastolic tissue velocity.
Diastolic dysfunction (using a strict definition) was present in 14 survivors (21.2%; median follow-up 21.4 years (range 6.8 to 42.9 years)), when compared with reference values from the literature (13). To verify this finding in the Dutch situation, we compared the diastolic function of the survivors with that of the controls. In the control group (n = 66), we found diastolic dysfunction in 10.6% of the participants (versus 21.2% of the survivors, p = 0.096). Echocardiographic measurements are depicted in Table 3. Both septal and lateral e′ were decreased compared with controls (p = 0.005 and p = 0.011, respectively), which confirms decreased diastolic function compared with controls. Early and late mitral valve inflow velocities were also lower in survivors compared with controls (both p < 0.001). Seven survivors and one control had an LAVI >34 mL/m2; however, especially in many controls, LAVI was lacking (Table 3).
As shown in Table 4 and Supplemental Table S1 (Supplementary Data are available online at
Unstandardized coefficient β.
e′mean, diastolic function expressed as mean of septal and lateral early diastolic tissue velocity.
Plasma biomarkers
Plasma levels of NT-proBNP, hs-troponin-T, and galectin-3 did not differ between survivors with and without diastolic dysfunction (Table 5). The number of survivors with a NT-proBNP >125 ng/L or galectin-3 > 17.8 ng/mL also did not differ between survivors with and without diastolic dysfunction.
hs-troponin-T, high-sensitivity troponin-T; NT-proBNP, N-terminal pro-brain natriuretic peptide.
Twenty-four-hour Holter electrocardiography
Twenty-four-hour Holter ECGs of 65 (98.5%) survivors were available for analysis. All survivors showed sinus rhythm; AF was not observed.
Discussion
This is the first nationwide study on late cardiac effects in survivors of pediatric DTC, showing frequent diastolic dysfunction in 21.2% of asymptomatic survivors after a median follow-up of 17 years, when compared with reference values from the literature and to a matched Dutch control group (13,16). As diastolic function declines with age, our findings may suggest early cardiac aging in survivors of pediatric DTC (15). This is important, as diastolic dysfunction may be the first manifestation of more overt heart failure (17). We do believe that the fact that we did not find a statistically significant difference between survivors and controls with respect to prevalence of diastolic dysfunction (p = 0.096) might be due to the small numbers of studied subjects using a strict definition of diastolic dysfunction. Since we found significant differences when comparing the mitral valve inflow and diastolic tissue velocities, we conclude that the high percentage of diastolic dysfunction in survivors and the significant differences in echocardiographic measurements between survivors and controls might be clinically relevant.
In our cohort, increasing attained age and waist circumference were associated with decreased diastolic function, which are established risk factors for diastolic dysfunction (17). We hypothesized that TSH would also be associated with diastolic dysfunction, as has been shown earlier by Smit et al. (9). Remarkably, this was not the case. A possible explanation for the different results may be related to the age of the survivors included in the studies. In our cohort, survivors were almost 17 years younger than in the cohort studied by Smit et al. Another explanation may lie in the degree of TSH suppression. The baseline TSH and six months follow-up TSH values reported in the study of Smit et al. (0.05 mU/L and 0.02 mU/L, respectively) were lower than in our study (0.17 mU/L) (9). However, the definition of TSH suppression and the number of TSH values available to support the TSH suppression are quite different in both studies. In our study, we used all available TSH values, and it revealed that TSH was suppressed to below 0.10 mU/L only in one-third of the survivors during the entire follow-up. In contrast, in the study by Smit et al. the TSH value during yearly follow-up was used to confirm suppression. Thus, it is unclear whether the results of these two studies can be compared. Although it has been shown that the degree of TSH suppression is related to cardiovascular mortality, it may be that diastolic dysfunction is triggered by TSH suppression per se rather than the level of TSH suppression (7). Increasing attained age, which could also be interpreted as a measure for longer duration of TSH suppression, was associated with decreased diastolic function in our cohort. Smit et al. included patients with a mean duration of TSH suppressive therapy (TSH <0.4 mU/L) of 12 years (9). In our study, median follow-up was 17 years. However, the assumption that attained age is a measure for duration of TSH suppression should be interpreted with caution as factors like potential nonadherence and prescriber factors may have impacted actual duration of TSH suppression. Furthermore, in our cohort all survivors used only levothyroxine (T4) as thyroid hormone replacement. It has been shown in thyroidectomized rats on T4 that circulating triiodothyronine (T3) does not always reflect tissue T3 levels in the heart (21). Tissue T3 has been proposed to elicit adverse cardiovascular effects when elevated (22). Therefore, it remains questionable whether the plasma TSH level is an adequate measure for cardiac tissue hyperthyroidism. Recently, an association between higher free T4, but not TSH, and increased risk of sudden cardiac death was shown (23). Unfortunately, free T3 and T4 levels during follow-up were not available for our study.
Systolic function was assessed by measurement of the LVEF and GLSS. GLSS has been shown to be of great additional value in detecting subclinical myocardial changes in adult cancer survivors, changes which can precede LVEF decreases and overt heart failure (8,24). In our cohort, systolic function was unaffected. In contrast to our findings, Abdulrahman et al. observed subtle systolic dysfunction using two-dimensional speckle tracking echocardiography in adult survivors of DTC (10). Moreover, the same group found a significantly lower LVEF compared with controls, although LVEF remained within the reference range (9). The explanation for the different results may be, again, that survivors in our cohort were younger than those in the other studies.
Our finding of frequent diastolic dysfunction is in line with findings in other cohorts of long-term childhood cancer survivors (16,25 –29). In those cohorts, systolic dysfunction has also been described (16,25 –29). However, as survivors in those cohorts were treated with anthracyclines and/or mediastinal radiotherapy, the mechanisms that trigger cardiac dysfunction may differ.
The question remains which factors explain the diastolic dysfunction found in our cohort. The development of diastolic dysfunction is a multifactorial process (17). Patients have their individual cardiovascular risk factors, which make them more or less inclined to develop diastolic dysfunction. We hypothesize that thyroid cancer treatment causes more rapid cardiac function deterioration by superposing the traditional risk factors also associated with decreased diastolic function in our cohort. Additionally, a subtle hyperdynamic state caused by the subclinical hyperthyroidism may contribute to the development of diastolic dysfunction. This hyperdynamic state arises as thyroid hormones stimulate the β-adrenergic signaling, leading to positive chronotropic and inotropic effects (30).
This study did not find an association between plasma levels of NT-proBNP, hs-troponin-T, or galectin-3 and diastolic dysfunction. An explanation for this may be that the diastolic dysfunction in our cohort was subclinical and therefore too mild to induce changes in plasma biomarkers. This implies that by measuring cardiac biomarkers alone, survivors with asymptomatic diastolic dysfunction could not be identified in our cohort.
AF was not observed using 24-hour ECG monitoring. In a cohort of adult survivors of DTC, an increased AF risk was described, independent of AF risk factors (11). However, in our study, survivors are significantly younger and therefore had fewer risk factors for AF.
The strength of this study is that it is the first study of cardiac function in long-term survivors of pediatric DTC, and includes data on cardiovascular risk factors available for all subjects. Furthermore, detailed data on tumor and treatment characteristics (including both historical and current TSH values) and outcome were available for all survivors. Assessment of GLSS was included in cardiac evaluation. Moreover, cardiac measurements were performed centrally, and interobserver variation was minimized, as the operator who performed all echocardiographic measurements in the survivors also performed these measurements in the control group (16).
Some limitations require comment. First, due to small patient numbers this study may suffer from a lack of power and therefore mild cardiac effects may be missed. Second, due to a different age distribution in both cohorts, the controls were slightly younger than the survivors despite matching and therefore the diastolic dysfunction cannot exactly be dissociated from the effects of ageing per se. However, as reference data of the American Society of Echocardiography are adjusted per 20 years, in our opinion, an age difference of less than 5 years is acceptable (13). Third, control data were collected between 2004 and 2007, whereas the data of the survivors were collected between 2012 and 2014 using different echo techniques, which may introduce bias. However, both methods are strongly correlated and therefore important differences in diastolic function due to the different echo techniques are not expected (18). Fourth, biomarkers were available only for the survivors. Finally, various TSH assays were used. However, we expect that the assay differences had limited influence on the results because the lower limits of the reference ranges remained more or less stable. As discussed earlier, free T3 and T4 levels during follow-up were not available for our study.
In conclusion, diastolic dysfunction was observed in 21.2% of long-term survivors of pediatric DTC using a strict definition of diastolic dysfunction, whereas systolic function remained unaffected in the majority of survivors. Increasing attained age and waist circumference were associated with decreased diastolic function, while TSH levels during follow-up were not. Since diastolic dysfunction is more common in the elderly, our findings suggest early cardiac aging in survivors of pediatric DTC. Indeed, the median age of survivors with diastolic dysfunction was only 38 years. Although diastolic dysfunction was subclinical, it is clinically relevant as it may be the first manifestation of more overt heart failure (17). Therefore, assessment and treatment of cardiovascular risk factors may require additional attention in this patient group as is already the case in other cancer survivors. An echocardiography might be easy accessible in the follow-up of survivors of pediatric DTC if clinically indicated. However, since this is the first study on cardiac dysfunction in survivors of pediatric DTC our data need to be confirmed in other cohorts. Moreover, follow-up studies are necessary to explore the longitudinal course of the diastolic dysfunction and potential intervention targets in survivors of pediatric DTC and to unravel pathophysiological mechanisms. Finally, it should be emphasized that cardiology follow-up together with regular communication between endocrinologists and cardiologists is required and that staging is mandatory before long-term, sometimes life-long, suppression treatment is implemented.
Footnotes
Acknowledgments
We are grateful to our colleagues in the Netherlands for referring patients to this study. We thank F. Boersma, Groningen Imaging Core Laboratory, for her help with the echocardiographic measurements and J. Haaksma and J. Rabbers, Department of Cardiology, University Medical Center Groningen, for their assistance with logistics and analysis of the 24-hour Holter ECGs. We thank the staff members of the cardiology departments of the participating centers for their collaboration.
This work was supported by the Stichting Kinderen Kankervrij (Foundation Children Cancer-Free, the Netherlands, project no. 81). C.M. Ronckers is supported by the Dutch Cancer Society.
The clinical trial registration number for this work is Netherlands Trial Registry (NTR) 3448.
This paper was presented in part at the 15th International Thyroid Congress, October 18–23, 2015, Orlando, Florida, and at the 39th Annual Meeting of the European Thyroid Association, September 3–6, 2016, Copenhagen, Denmark.
Author Disclosure Statement
No competing financial interests exist.