
Abstract
Background:
Whether iodized salt increases the risk of thyroid disease has been strongly debated in China, especially in the urban areas of coastal regions, in recent years. This study aimed to investigate the status of iodized salt in terms of urinary and serum iodine concentration in urban coastal areas, and to explore further whether consumption of iodized salt or non-iodized salt is associated with autoimmune thyroid disease (AITD).
Methods:
The data source was SPECT-China, a cross-sectional study in East China. A total of 1678 subjects were enrolled from 12 communities in downtown Shanghai. The type of salt consumed, the urinary iodine concentration (UIC), serum iodine, thyroid peroxidase antibodies (TPOAb), and thyroglobulin antibodies (TgAb) levels were obtained. AITD was defined as serum TPOAb and/or TgAb >60 kIU/L (TPO/TgAb [+]).
Results:
The prevalence of AITD was 10.5% in men and 21.4% in women. The median UIC and serum iodine concentration were 106.4 μg/L and 60.9 μg/L, respectively. Among all the subjects, 46.4% consumed non-iodized salt; the prevalence of iodine deficiency among those subjects was significantly higher than that of the subjects who consumed iodized salt (54.2% vs. 40.1%; p < 0.001). Consumption of non-iodized salt was positively associated with AITD in all participants (odds ratio [OR] = 1.49 [confidence interval (CI) 1.15–1.95]; p = 0.003) and in women (OR = 1.63 [CI 1.20–2.21]; p < 0.01) after multivariable adjustment. Additionally, the association between low UIC and AITD was observed among all subjects (OR = 1.50 [CI 1.10–2.05]; p = 0.01) and in women (OR = 1.45 [CI 1.02–2.07]; p = 0.038).
Conclusions:
In coastal areas, which are believed to be rich in iodine, consuming non-iodized salt still led to lower UIC levels and a higher prevalence of iodine deficiency. The consumption of non-iodized salt and low UICs might be a risk factor for AITD, especially for women, which should be further confirmed by longitudinal studies.
Introduction
A
Iodine is an essential micronutrient for the synthesis of thyroid hormones. Iodine deficiency (ID) in early life impairs cognition and growth, and also has many adverse effects throughout the human life-span (4). During the past two decades, remarkable progress has been achieved in the global effort to eliminate ID. Currently, >70% of the population worldwide has access to iodized salt, up from 20% in 1990 (5). However, the salt iodization program is fragile and requires long-term commitment from governments. In several countries where ID had been once eliminated, salt iodization programs fell apart, and ID has now re-emerged, for example in Australia (6), New Zealand (7), and the United Kingdom (8). It is mainly due to the reluctance of the food industry in these countries to use iodized salt (5).
ID was once common in China. Therefore, a mandatory universal salt iodization (USI) program was launched in 1996, and was successful in dramatically decreasing the prevalence of endemic goiter in China. However, because the number of patients with thyroid diseases has dramatically increased in recent years, some concerns about the USI have circulated, especially among coastal residents in urban areas (9). It is unknown whether the higher prevalence of reported thyroid disorders is due to an actual increase in incidence or to the application of more accurate diagnostic procedures. Currently, there is a heated debate regarding whether it is necessary to continue the USI program (10 –12). It is of great value to investigate further the association between iodized salt and thyroid autoimmunity 20 years after the introduction of USI. In addition, some studies have also suggested that milk intake may be positively associated with urinary iodine concentration (UIC), implying that milk consumption could partly improve iodine nutrition (8,13).
The aim of this study was to investigate the current UIC and serum iodine concentrations (SIC) in an urban Chinese population. Additionally, the study aimed to explore whether iodized salt is associated with AITD and to evaluate the effects of milk consumption on the prevalence of AITD.
Materials and Methods
Study population
The data source was SPECT-China (ChiCTR-ECS-14005052;

Flow chart of the inclusion and exclusion of participants.
The study was approved by the Ethics Committee of Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine, and was performed in accordance with the Declaration of Helsinki. Prior to the data collection, all participants signed written informed consent forms.
Measurements
A structured questionnaire was designed to obtain general information, which included demographic characteristics, lifestyle-related risk factors, and a personal or family history of thyroid disease. The questionnaire was administered face-to-face by well-trained investigators from Shanghai Ninth People's Hospital. Current smoking was defined as having smoked at least 100 cigarettes in one's lifetime and currently smoking cigarettes (16). Current drinking was defined as alcohol intake more than once per month during the past 12 months (16). Consuming milk once or less per week was defined as having no habit of milk consumption, while consuming milk twice or more per week was defined as having a habit of milk consumption (17). The item “For the past three years, which type of salt was consumed in your family?” was used to collect information about the type of salt consumed. Three options for this item were provided: (i) only iodized salt, (ii) non-iodized salt, and (iii) both. The number of subjects who consumed both types of salt was small (n = 31), and they were classified in one of the other two groups according to the type of salt they currently used: iodized salt or non-iodized salt. Weight and height were measured with the participants wearing light clothing and no shoes. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (18).
Spot urine and blood samples were obtained from each participant in the morning after an overnight fast. Serum thyroid peroxidase antibodies (TPOAb), thyroglobulin antibodies (TgAb), total thyroxine (TT4), total triiodothyronine (TT3), free triiodothyronine (fT3), free thyroxine (fT4), and thyrotropin (TSH) were measured using the chemiluminescence immunoassay (Immulite 2000; Siemens, Munich, Germany). AITD was defined as serum TPOAb and/or TgAb positivity (>60 IU/mL; TPO/TgAb[+]) (19).
UIC was determined with arsenic cerium catalytic spectrophotometry (WS/T 107.1–2016). The Chinese National Laboratory for Prevention and Treatment of Iodine Deficient Disorders provided the external reference samples. The total circulating iodine levels were measured with an inductively coupled plasma mass spectrometer (ICP-MS). A 200 μL serum aliquot was added to a 3.8 mL diluent containing Triton X-100 (0.1%) and nitric acid (1%). The aliquot was then vortexed with 20 μL of an internal standard solution for detection (no. 7900; Agilent Technologies, Santa Clara, CA).
For 915 participants, table salt samples of at least 20 g were collected, and then sealed and stored at room temperature away from light until they were measured. The concentration of iodine was measured using the colorimetric titration method.
Statistical analysis
Statistical analysis was carried out using SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY). General characteristics are summarized as the median with interquartile range (IQR) for continuous variables or as proportion for categorical variables. Mann–Whitney's U-test and the Kruskal–Wallis test were used for comparison of two or more groups of non-normal data. Pearson's chi-square tests were performed to compare categorical variables.
The adjusted associations of type of salt, milk consumption, UIC, and SIC with AITD were analyzed with binary logistic regression analyses. The results are expressed as odds ratio (OR) and confidence intervals (CIs). The following variables were selected as covariates: age, sex, educational status, current smoker, current drinker, BMI, and TSH. Educational level is an important socioeconomic covariate and is commonly adjusted in epidemiological studies. In the present study, those who consumed non-iodized salt were more likely to have a higher educational level. BMI was adjusted, since obesity can enhance the risk of thyroid autoimmunity (20). Current drinking was adjusted because emerging evidence has suggested that alcohol is a modulator of the immune system, and alcohol consumption may protect against autoimmune hypothyroidism (21).
In a sensitivity analysis, AITD was also defined as TPOAb- and/or TgAb-positive status combined with characteristic ultrasonographic features (diffuse hypoechogenicity of the thyroid parenchyma and/or heterogeneous echogenic pattern of the thyroid gland; TPO/TgAb[+] and US[+]) (22). Thyroid ultrasonography was performed by two certified US doctors using B-mode US imaging (MINDRAY M7) with a 10 MHz linear array probe.
Results
Iodine content of salt used, UIC, and SIC in the population
The median iodine content of the salt samples was 26.3 mg/kg (IQR 24.1–28.7 mg/kg). The distribution of UICs in the study population is shown in Figure 1. The median urinary iodine excretion in the sample was 106.4 μg/L (IQR 71.5–158.5 μg/L). Urinary iodine measurements indicative of ID (UIC <100 μg/L) were present in 46.8% of the study population. Meanwhile, 9.4% and 5.5% of the population showed more than adequate (UIC 200–299.9 μg/L) and excess iodine intake (UIC ≥300 μg/L), respectively. In addition, participants who consumed non-iodized salt had a significantly higher proportion of ID; this was true for both men (49.0% vs. 37.5%; p = 0.03) and women (57.4% vs. 41.5%; p < 0.001; Fig. 2). The median SIC was 60.9 μg/L (IQR 22.4–147.4 μg/L).
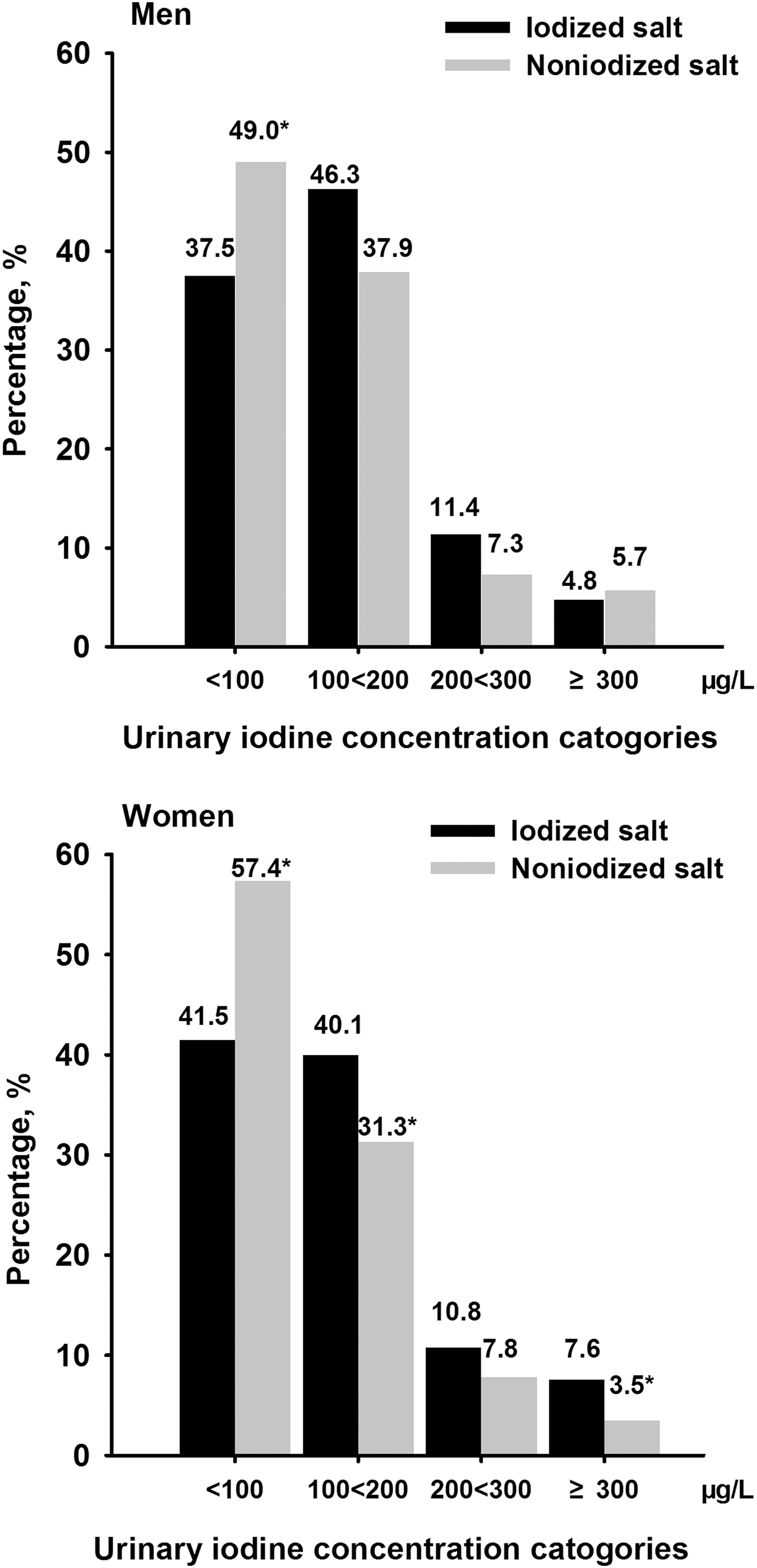
Sex-specific distribution of urinary iodine concentration stratified by the type of salt used. *p < 0.05 versus iodized salt group.
General characteristics and thyroid disease spectrum stratified by the type of salt used
Table 1 shows general characteristics and the thyroid disease spectrum stratified by the type of salt used. A total of 46.4% of subjects consumed non-iodized salt. Compared to those who consumed iodized salt, subjects who consumed non-iodized salt showed significantly lower UIC in both females and males (p < 0.001) but a comparable SIC. Meanwhile, women and men who consumed non-iodized salt had a higher educational level (p < 0.05). The prevalence of AITD, either defined by TPO/TgAb(+) or TPO/TgAb(+) and US(+), was significantly higher in the non-iodized salt group compared to the iodized group in women but not in men.
Data are summarized as median (interquartile range) for continuous variables, or as number with proportion for categorical variables.
p < 0.05 versus iodized salt group.
UIC, urinary iodine concentration; SIC, serum iodine concentration; BMI, body mass index; TSH, thyrotropin; TT3, total triiodothyronine; TT4, total thyroxine; fT3,free triiodothyronine; fT4, free thyroxine; TPO, thyroid peroxidase; TgAb, thyroglobulin antibodies.
General characteristics stratified by TPO/TgAb positivity
General characteristics in terms of TPO/TgAb positivity are presented in Table 2. The study population comprised 1678 subjects with a mean ± SD age of 61 ± 11 years, 17.4% of whom had prevalent TPO/TgAb(+). The prevalence of TPO/TgAb(+) was 10.5% in men and 21.4% in women. Compared to subjects in both the TPOAb and TgAb negative (TPO&TgAb[–]) group, those with AITD had significantly lower UIC in women (87.8 μg/L [IQR 65.3–149.7 μg/L] vs. 106.6 μg/L [IQR 71.5–157.5 μg/L]; p = 0.032] but not in men. The SIC was comparable between the two groups for both sexes. Women with positive thyroid antibodies were more likely to consume non-iodized salt (54.4% vs. 43.3%; p = 0.003) and to have significantly higher levels of serum TSH.
Data are summarized as median (interquartile range) for continuous variables, or as number with proportion for categorical variables.
p < 0.05 versus TPO/TgAb(+).
Associations of type of salt and milk consumption with AITD
The associations of iodized salt and milk consumption with AITD were estimated (Fig. 3). After adjusting for age, sex, educational status, current smoking, current drinking, BMI, and TSH, non-iodized salt (OR = 1.494 [CI 1.145–1.949]; p = 0.003) was individually associated with AITD in all participants. However, in the sex-specific analysis, this association was only significant in women (OR = 1.628 [CI 1.201–2.207]; p < 0.01). No association was found between milk consumption and AITD in either sex.
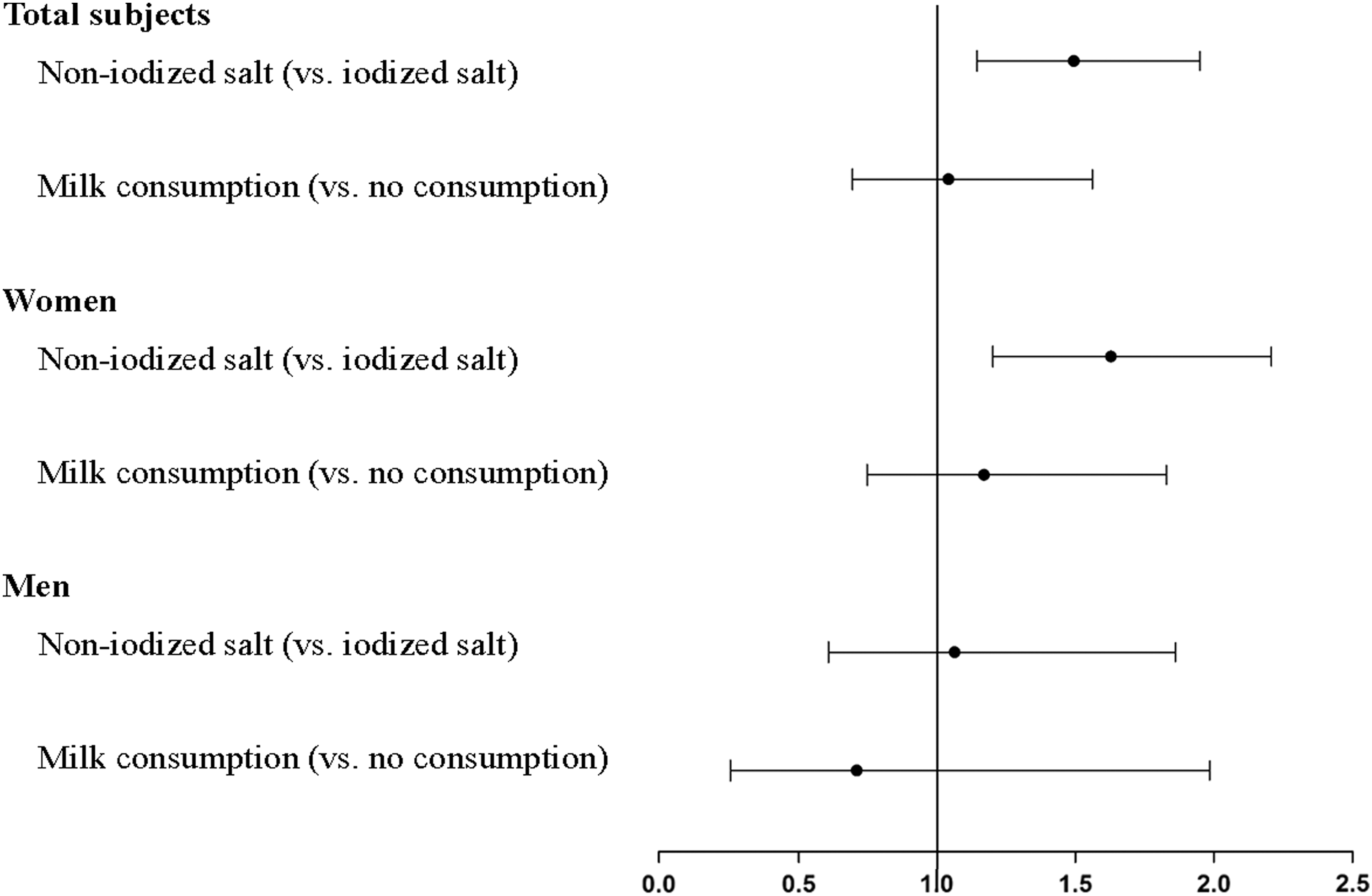
Adjusted associations of type of salt, milk consumption with autoimmune thyroid disease stratified by sex. Data are reported as odds ratios (confidence intervals). Binary logistic regression analyses (forward stepwise) were performed. Adjustment for age, sex, educational status, current smoker, current drinker, body mass index, and serum thyrotropin.
Associations of UIC and SIC with AITD
The association between UIC and AITD is shown in Table 3. After multivariable adjustment, compared to participants with adequate iodine nutrition, those with iodine deficiency had an increased risk of TPO/TgAb(+) (OR = 1.503 [CI 1.102–2.048]; p = 0.010). Meanwhile, subjects with more than adequate and excess iodine nutrition did not have an increased risk of TPO/TgAb(+). However, when the subjects were stratified by sex, a significant association between low UIC and risk of TPO/TgAb(+) was observed only in women (OR = 1.453 [CI 1.020–2.069]; p = 0.038).
Data are odds ratios [confidence intervals]. Binary logistic regression analyses (forward stepwise) were performed.
Adjustment for age, sex, educational status, current smoker, current drinker, BMI, and TSH.
Urinary iodine concentrations: low, <100 μg/L; adequate, 100 to <200 μg/L; more than adequate, 200 to <300 μg/L; excessive, ≥300 μg/L.
OR, odds ratio; CI, confidence interval.
Moreover, no association was found between SIC and AITD in either sex (Table 4).
Data are odds ratios [confidence intervals]. Binary logistic regression analyses (forward stepwise) were performed.
Adjustment for age, sex, educational status, current smoking, current drinking, BMI and TSH.
Serum iodine concentration:
Pooled: 10th–90th percentile, 32.8–106.8 μg/L; <10th percentile, ≤32.7 μg/L; >90th percentile, ≥106.9 μg/L.
Women: 10th–90th percentile, 33.1–112.9 μg/L; <10th percentile, ≤33.0 μg/L; >90th percentile, ≥113.0 μg/L.
Men: 10th–90th percentile, 31.5–98.1 μg/L; <10th percentile, ≤31.4 μg/L; >90th percentile, ≥98.2 μg/L.
Sensitivity analysis
In a sensitivity analysis, AITD was also defined as TPO/TgAb(+) and US(+). The association of non-iodized salt (OR = 1.518 [CI 1.021–2.258]; p < 0.05) and iodine deficiency (OR = 1.759 [CI 1.085–2.852]; p < 0.05) with TPO/TgAb(+) and US(+) remained significant in women.
Discussion
This study found that 46.4% of the subjects consumed non-iodized salt, and 46.8% had ID. The consumption of non-iodized salt and the presence of low UICs was significantly associated with a higher prevalence of TPO/TgAb(+). This indicates that consuming non-iodized salt may contribute to the high proportion of ID; subjects who consumed non-iodized salt had a lower UIC and may have an increased risk of AITD. Maintaining the USI program at an appropriate level is still important for preventing ID in coastal areas of China, an area that was previously believed to be rich in iodine (9).
The median UIC of residents of downtown Shanghai was 106.4 μg/L, showing an adequate iodine intake. Nevertheless, and rather surprisingly, 46.8% of the adults in this study had ID. According to the study conducted by the Shanghai Municipal Center for Disease Control and Prevention in 2009, 95.3% of participants used iodized salt (23). At that time, the median UIC of the general population of Shanghai was 146.7 μg/L, and 28.6% of the study population was iodine deficient (23). The present study indicates that urban dwellers in downtown Shanghai now have a lower UIC and larger proportion of ID, perhaps because of their preference for using non-iodized salt in recent years.
Why did so many residents in our study population (46.4%) consume non-iodized salt in an area under USI? Concerns about the thyroid health of populations in coastal provinces in the context of USI have circulated in the local media and international medical literature (24). In this study, those who consumed non-iodized salt were more likely to have a higher educational level. People with a higher academic background are more likely to be influenced by the available information and worry about their thyroid health. Some coastal city authorities have been unofficially allowing the sale of non-iodized salt, which formerly required a prescription, and there were calls for liberalizing provincial control of such sales (25). Meanwhile, because Shanghai is a coastal city, residents hold the viewpoint that since they have more opportunities to consume aquatic products containing sufficient iodine, they should never suffer from iodine deficiency. This study was consistent with a previous study showing that in an urban area of a coastal province, 47.4% of the participants used non-iodized salt (10).
The concept that seafood consumption alone can provide sufficient iodine may not be true. Actually, the environmental iodine levels in Shanghai are deficient (<10 μg/L) (11). Moreover, according to research conducted by the Shanghai Municipal Center for Disease Control and Prevention, iodized salt contributed 63.5% of the total dietary iodine in Shanghai (23). Aquatic products, which residents consider to be rich in iodine, contributed only 5.03% of the total dietary iodine (23). Thus, iodized salt is still the main vehicle for iodine supplementation in coastal populations.
It has been reported that milk is an important source of dietary iodine in Western countries (8,13,26). This is largely due to the presence of iodine in cattle feeds and the iodophors used for disinfection (26). However, the native iodine content of dairy products is low, and there is no iodine fortification of cattle fodder in China. Deng et al. reported that iodine content from milk accounted for only 0.4% of the UIC in China (27). Thus, milk may have a small effect on iodine intake in China.
AITD results from a dysregulation of the immune system that leads to an immune attack on the thyroid (1). In the general population, 10–15% of the healthy population have detectable thyroid autoantibodies (11,28). The prevalence of thyroid autoantibodies increases with age and is more common in women (29). In the present study population with a mean age of 60 years, the prevalence of TPOAb and/or TgAb positivity was 17.4%, with 10.5% in men and 21.4% in women.
The results regarding the association between iodine intake and thyroid autoimmunity are far from conclusive. Some studies have indicated that providing iodine supplementation for populations that were previously iodine deficient is associated with an increase in the prevalence of thyroid autoantibodies (30,31). However, Pedersen et al. (29) reported that in the 60–65 years age group, thyroid antibodies were more frequently found in moderate than in mildly iodine-deficient areas. Two population-based studies in older people aged 75–80 years have also demonstrated that thyroid autoantibodies occur more frequently if iodine deficiency is present, though the subjects were quite old and their immune capability may, in part, contribute to the increase in antibodies (19,32). It is worth noting that Shanghai has historically been considered a non-ID-endemic area (23). Moreover, it is well acknowledged that either insufficient or excess iodine intake may lead to thyroid disease (5,33). This factor may not be excluded from the association between iodine intake and thyroid autoimmunity, which warrants further investigation. The detailed mechanism of the relationship of ID with AITD is unknown. ID is significantly associated with an increase in oxidative stress (34). Recent evidence has shown that cytokines play an important role in the pathogenesis of AITD (1). Hence, it is hypothesized that the possible mechanism through which ID influences AITD may be through an inflammatory response.
This study also found that compared to the non-iodized salt group, subjects who consumed iodized salt had comparable SIC, and no association was found between SIC and thyroid antibodies. UIC is an excellent indicator of recent iodine intake because the kidney excretes >90% of dietary iodine within 24–48 hours in healthy, iodine-replete adults (5). In this study, it seems that serum iodine remained stable, regardless of whether urinary iodine concentrations were high. This finding helps explaining why WHO/ICCIDD/UNICEF recommend the use of UIC to reflect the iodine nutrition of a population.
We believe that the findings of this survey have great public-health importance for Shanghai. ID, unlike most micronutrient deficiencies, is not restricted to people in developing countries with poor diets. When salt iodization was discontinued, ID recurred in several industrialized countries (5). Thus, scholars in these countries strongly recommend the implementation of mandatory salt iodization (6,35). In downtown Shanghai, the UIC has fallen to marginal levels of iodine sufficiency (106.4 μg/L), and 46.8% of the subjects in the study population were iodine deficient. The concern is that without proper guidance, an increasing number of residents choose to use non-iodized salt.
One highlight of this study is that the iodine content of table salt and the UICs and SICs were all measured. Thus, the iodine status was comprehensively evaluated in the present study, in contrast to previous studies that mainly focused on UIC. This study does have some limitations. First, no causal relationship could be determined due to the cross-sectional design of the study. Second, data regarding the exact time when residents used iodized or non-iodized salt were not available. Future longitudinal studies with a large sample size should be performed. Third, information on family history data was not collected. However, since the subjects enrolled in this study have a mean ± SD age of 60 ± 11 years, their parents may have little knowledge about their thyroid health due to unfavorable medical conditions at that time.
In summary, a concerning number of subjects in downtown Shanghai have ID. Coastal adults who consume non-iodized salt, especially women, may have an increased risk of AITD. Serum iodine levels seemed to be stable, and no association was observed between SIC and AITD. At this point, maintaining USI is indispensable for the coastal urban Chinese population.
Footnotes
Acknowledgments
This study was supported by National Natural Science Foundation of China (81570726, 81600609); Shanghai JiaoTong University School of Medicine (2014); Science and Technology Commission of Shanghai Municipality (16410723200). The Fourth Round of Three-year Public Health Action Plan of Shanghai (15GWZK0202). The funders played no role in the design and conduct of the study; collection, management, analysis, and interpretation of data; or preparation, review, and approval of the manuscript.
Author Disclosure Statement
No potential conflicts of interest relevant to this article were reported.