
Abstract
Background:
In pregnant women with Graves' disease, maternal thyrotropin receptor antibodies (TRAb) can cross the placenta and induce fetal or neonatal thyrotoxicosis. Symptoms of fetal thyrotoxicosis are tachycardia, intrauterine growth restriction, and intra-uterine death. Recommendations on an upper limit of TRAb concentrations below which intensive fetal monitoring can be safely omitted vary between different guidelines. The objective of this study was to define an evidence-based cutoff level for maternal TRAb necessitating additional fetal monitoring during pregnancy.
Methods:
A literature search was performed to identify studies on pregnant women with Graves' disease and fetal and/or neonatal thyrotoxicosis. Only studies that reported TRAb were included.
Results:
From a total of 229 identified titles, 20 articles could be included in the analysis. A total of 53 cases of fetal and/or neonatal thyrotoxicosis were described. The lowest level of maternal TRAb leading to neonatal thyrotoxicosis was 4.4 U/L, which corresponds to 3.7 times the upper limit of normal. The level of evidence for this threshold is moderate to low.
Conclusion:
In women with Graves' disease, intensive fetal monitoring is recommended when maternal TRAb concentrations are >3.7 times the upper limit of normal. This cutoff level should be interpreted with caution, since evidence is limited.
Introduction
G
The lifetime risk of developing Graves' disease is approximately 3% (3). During pregnancy, Graves' disease is relatively uncommon, occurring in 0.1–0.2% of all pregnancies (4 –6). TRAb are immunoglobulin G class antibodies, which may cross the placenta and can also influence the fetal thyroid gland (7). Maternal TRAb levels are highest in the first trimester of pregnancy and gradually fall in the second and third trimesters (8). When the fetal thyroid is functional, it can respond to TRAb, causing excess fetal production of thyroid hormone. Typically, fetal hyperthyroidism due to cross-placental passage of TRAb develops at or after week 20 of pregnancy. Therefore, the moment of TRAb sampling during pregnancy is important to predict the fetal consequences (9). Fetal and/or neonatal thyrotoxicosis occurs in 1.0–5.0% of children born to a mother with Graves' disease (10). The risk of fetal and/or neonatal thyrotoxicosis rises with higher maternal TRAb concentrations (11). Complications of fetal and neonatal thyrotoxicosis include intra-uterine growth retardation, congestive heart failure, craniosynostosis, and intra-uterine death (3,12).
Thyroid antibodies are present in most women with active Graves' disease and can still be present in women with a history of Graves' disease (2). Therefore, current guidelines advise measuring maternal TRAb in pregnant women with Graves' disease or a history of Graves' disease (13,14).
When TRAb levels are elevated, intensive fetal monitoring is indicated to detect fetal thyrotoxicosis (15). The condition of the fetus is monitored by sequential ultrasounds to detect signs of fetal thyrotoxicosis, including tachycardia (>160 bpm), hydrops, oligohydramnios, goiter formation, premature bone ossification, and growth restriction (2,16). Early detection and treatment of fetal and neonatal thyrotoxicosis is important to prevent adverse pregnancy outcomes.
The American Thyroid Association (ATA) recommends a threshold for maternal TRAb of three times the upper limit of normal (ULN) (14). This recommendation is based on a French study by Abeillon-du Payrat et al. who recommended a threshold of >5 IU/L and a ULN of 3.3 (17). These findings were confirmed in a study by Besançon et al., who recommend a threshold of two times the ULN, without further specification of TRAb levels (18).
The Endocrine Society describes a threshold for maternal TRAb of two to three times the ULN (13). This is based on five studies (2,11,19 –21). None of these studies express TRAb levels in IU/L. Nachum et al. performed umbilical blood sampling in those mothers with elevated TRAb values, but no correlation between TRAb values and neonatal thyrotoxicosis was given (4). Mortimer et al. expressed the TRAb levels in percentages, and they described maternal TRAb levels, leading to neonatal thyrotoxicosis, of 4.6 times the ULN (21). In both studies, the ULN is above the described ULN of the Endocrine Society. Mitsuda et al. expressed the TRAb levels in percentages measured at delivery. In four cases, neonatal thyrotoxicosis occurred in mothers with TRAb levels below the ULN at delivery (20). In the remaining studies, no TRAb levels were described. In these studies, different assays were used.
In summary, the recommendations of the ATA and the Endocrine Society are based on a limited number of different reports of varying quality. The level of evidence for the recommendation will likely improve with a systematic review of the literature.
The aim of this study was to determine an evidence-based threshold for maternal TRAb above which additional fetal monitoring is necessary to detect fetal and/or neonatal thyrotoxicosis. To achieve this aim, a systematic review of the literature was performed.
Methods
Literature search
Relevant studies, published until June 2016, were identified by searching PubMed using the terms “thyrotropin-binding inhibitory immunoglobulin” AND “fetus” AND “thyrotoxicosis” (for a detailed description of the search, see Supplementary Data; Supplementary Data are available online at
Eligibility criteria
Studies were included if (i) the study involved pregnant women with Graves' disease or pregnant women after previous treatment for Graves' disease, (ii) maternal TRAb levels were measured during pregnancy, (iii) fetal and/or neonatal thyrotoxicosis was present, and (iv) a clear description on how fetal and/or neonatal thyrotoxicosis was diagnosed was provided in the study.
Studies were excluded if (i) maternal TRAb levels were expressed as a percentage, (ii) a bio-assay was used to measure maternal TRAb, or (iii) only a recommendation for a cutoff level was given. Only studies in English, Dutch, and German were included.
In the search strategy, initially studies that reported TRAb as % inhibition were excluded because it was assumed that radioimmunoassays are largely replaced by other immunoassays without radioisotopes. An additional analysis on the studies that were initially excluded (n = 17) was performed.
Literature selection and data extraction
Titles and subsequently abstracts of the studies were screened by two independent reviewers: I.H.S. (fourth-year medical student) and M.D. (MD and PhD student). In case of disagreement, a third reviewer (P.B.) was consulted for the decision on inclusion or exclusion for full-text evaluation. Relevant studies were read full text, and a selection was made based on the predetermined inclusion and exclusion criteria. After consensus, the remaining articles were included for critical appraisal and assessed independently by two reviewers (I.H.S. and M.D.).
Data analysis
Data about the size, age, and disease status (past or present Graves' disease, treated or untreated) of the study population and the occurrence and diagnosis of fetal and/or neonatal thyrotoxicosis were collected. In the included studies, assays of different generations were used to determine maternal TRAb. Three generations of radio-receptor assays are available at this moment. The type of assay used to determine maternal TRAb levels was also recorded if reported in the article.
Methodological quality assessment
Quality assessment of the studies was performed with a corresponding assessment tool. For case reports and case series, the “Quality assessment tool for case-series studies,” developed by the National Institute for Health and Care Excellence (NICE), was used (
Results
Results on literature search
A total of 227 studies were identified. All studies were screened based on title and abstract, and 162 studies were excluded. The majority of the excluded studies did not report TRAb concentrations or were in a language other than Dutch, English, or German. After full-text screening, 18 studies could be included in the final analysis. All references of the included studies were checked for relevance, and two additional studies were included. The study selection process is summarized in Figure 1.
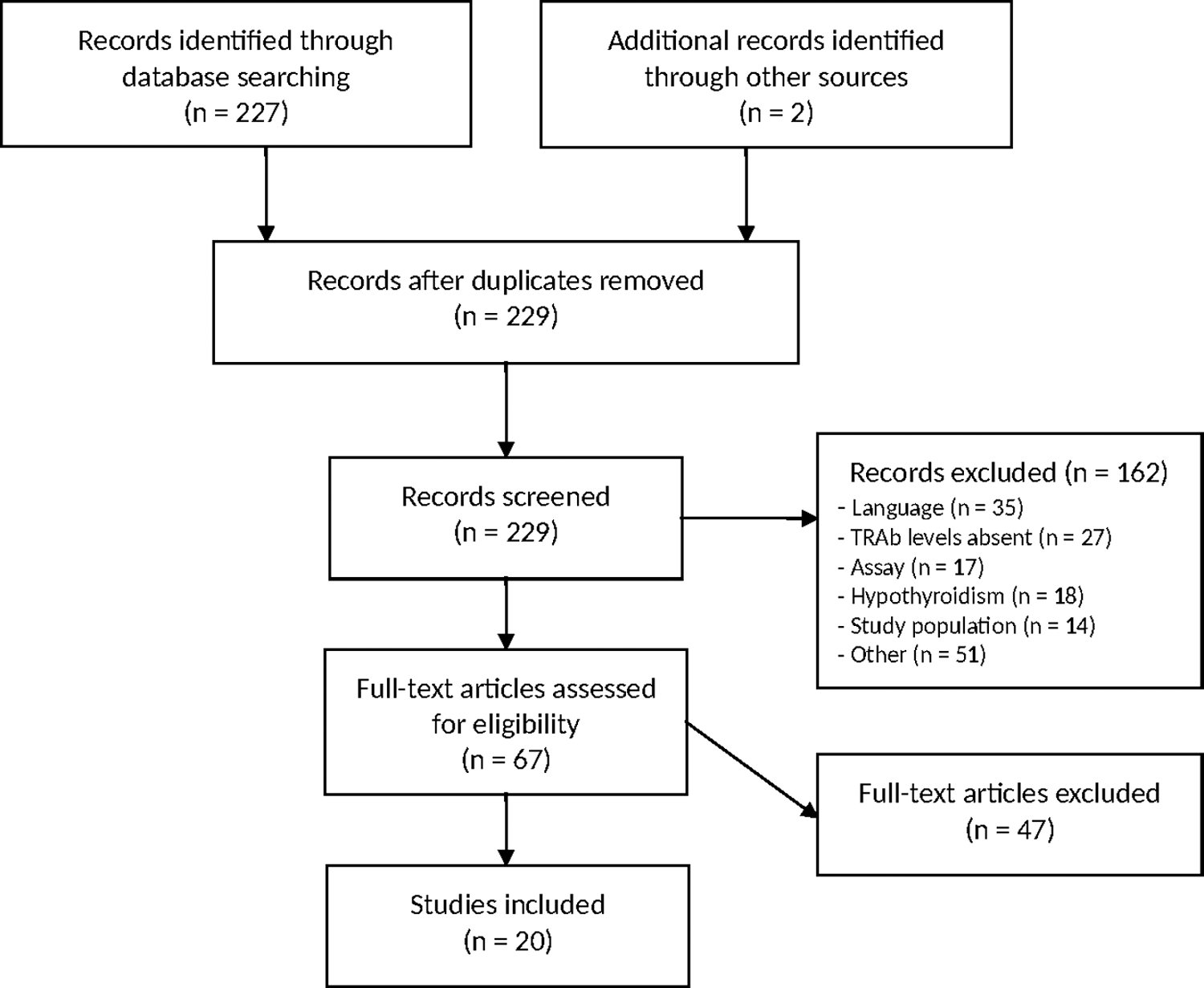
Study selection process.
TRAb concentrations
The selected articles are summarized in Tables 1 and 2. The lowest level of maternal TRAb leading to neonatal thyrotoxicosis was 4.4 U/L. This level was measured by a second-generation assay in the third trimester of pregnancy.
TSH, thyrotropin; fT4, free thyroxine; fT3, free triiodothyronine; T1, T2, and T3, trimesters 1, 2, and 3; ATD, antithyroid drugs; FH, fetal hyperthyroidism; NH, neonatal hyperthyroidism; US, ultrasound.
Cohort studies
Six cohort studies were included. Abeillon-du Payrat et al. performed a retrospective study on 42 pregnant women with (treated) Graves' disease. Maternal TRAb levels were analyzed in 33 women during the first trimester, in 32 women during the second trimester, and in 34 women during the third trimester of pregnancy. Nine of the 47 neonates were born with thyrotoxicosis. The TRAb levels of the mothers who gave birth to neonates with thyrotoxicosis were between 5.6 and 258.0 IU/L (>3.7 times the ULN). The TRAb levels of mothers who gave birth to neonates without thyrotoxicosis were between <0.4 and 60 IU/L (17).
Clavel et al. performed a prospective study on 35 pregnant women with Graves' disease. Maternal TRAb levels were analyzed in the third trimester of pregnancy. Of the 35 neonates, seven were born with thyrotoxicosis. The TRAb levels of the mothers who gave birth to neonates with thyrotoxicosis were all >40 U/L (>4 times the ULN) (7).
Uenaka et al. performed a prospective study on 35 pregnant women with Graves' disease. Maternal TRAb levels were determined in the third trimester of pregnancy. Of 31 neonates who were born, five had neonatal thyrotoxicosis. The corresponding maternal TRAb levels were between 9.2 and 512.0 IU/L (>9.2 times the ULN) (23).
Elston et al. performed a retrospective study on 29 pregnant women with treated Graves' disease. A total of 49 pregnancies were described, and maternal TRAb levels were measured in 17 pregnancies. Only one of the 49 neonates had thyrotoxicosis. The maternal TRAb level was 32 U/L (21 times the ULN) (24).
Gietka-Czernel et al. performed a prospective study on 42 pregnant women with Graves' disease. Fetal thyrotoxicosis was detected in four instances by ultrasound. An evaluation of gestational age, fetal anatomy, growth parameters, viability, amniotic fluid volume, thyroid size and characteristics of possible fetal goiter, heart rate, and bone maturation was carried out. In two cases, fetal blood sampling was performed, due to confounding clinical data. Eventually, only three cases of neonatal thyrotoxicosis were described because of successful intra-uterine treatment of fetal thyrotoxicosis in one case. Maternal TRAb levels leading to fetal thyrotoxicosis were >9.2 IU/mL (>5.1 times the ULN), and TRAb levels leading to neonatal thyrotoxicosis were >35.5 IU/mL (>19.7 times the ULN) (16).
Kamijo et al. performed a prospective study on 47 pregnant women with Graves' disease. Maternal TRAb levels were determined in late pregnancy. Forty-seven neonates were born, and two of them had neonatal thyrotoxicosis. The corresponding maternal TRAb levels were 40.68 IU/L (26.7 times the ULN) and 89.79 IU/L (59.9 times the ULN) (8).
Case series and case reports
Fourteen case series and case reports were included in this review (25 –38). They all described one, two, or three cases of neonatal and/or fetal thyrotoxicosis. Maternal TRAb levels were analyzed in all studies. The maternal TRAb levels leading to fetal and/or neonatal thyrotoxicosis were between 4.4 and 800.0 U/L (corresponding to 4.4–198.5 times the ULN).
In order to diagnose fetal thyrotoxicosis, fetal ultrasounds were carried out in 11 studies (16,25 –31,33,37,38). In six studies, cordocentesis was performed (26,27,31,33,37,38). Neonatal thyrotoxicosis was diagnosed based on thyroid hormone levels in all studies. In 12 studies, clinical symptoms of neonatal thyrotoxicosis were also described (8,25 –27,29,30,32 –37). Ultrasounds of the neonatal thyroid gland were performed in three studies (31,36,37) (see Tables 1 and 2).
There was considerable heterogeneity in the diagnostic methods used for determination of thyrotoxicosis. Different generations of assays were used for determination of maternal TRAb levels in the studies. An overview of assays, manufacturers, and the corresponding normal value is provided in Supplementary Table S1.
Radioimmunoassays
The studies that were initially excluded (n = 17) were subsequently analyzed. All these studies used radioimmunoassays, and the results are listed in Supplementary Tables S2 and S3. Nine studies used radioimmunoassays to detect TRAb. The lowest threshold for fetal/neonatal thyrotoxicosis was 3.8 times the ULN for studies using radioimmunoassays to measure TRAb.
Methodological quality
Six observational studies were included (7,8,16,18,23,24). All other studies were case reports or case series (25 –38). Included studies are level II studies (cohort studies) and level IV studies (case series and case reports). Overall, the case series, case reports, and cohort studies included had a moderate risk of bias, based on the quality assessment reported in Supplementary Tables S4–S6. Since consecutive sampling is only described in one cohort study, presence of inclusion bias in the other studies is likely. Taking this into account, the level of evidence of this review is moderate to low.
Discussion
An evidence-based cutoff level for maternal TRAb in pregnant women with Graves' disease or after definitive therapy for Graves' disease was determined in this review. The lowest level of maternal TRAb leading to neonatal thyrotoxicosis found in the literature was 4.4 U/L and 3.7 times ULN. This level was measured by a second-generation assay manufactured by Brahms in the third trimester of pregnancy. The studies included in this review used different types of assays to determine TRAb levels, and TRAb levels were measured at different times in pregnancy. Additional screening is advised when TRAb levels exceed 4.4 U/L. This is 3.7 times the ULN (normal value of second-generation assay by Brahms <1.5 U/L).
The results of this study are in line with previous research. The review of van der Kaay et al. concluded that determining a cutoff value is not yet possible because of lack of assay harmonization. They advised laboratories measuring maternal TRAb to state clearly which assay is used because this information is essential to compare TRAb levels in different studies (39).
Abeillon-du Payrat et al. performed a retrospective cohort study on 42 pregnant women: 20 women with Graves' disease and 22 women with treated Graves' disease (17). They concluded that there is a risk of fetal and/or neonatal thyrotoxicosis when maternal TRAb are >5 IU/L. This statement is based on measurements of maternal TRAb in the second trimester. The cutoff value proposed by Abeillon-du Payrat et al. is slightly higher than the value found in the present review. This could be explained by the fact that the cutoff value found in this review is based on measurements in the third trimester instead of the second trimester.
The ATA recommends a cutoff level for maternal TRAb of three times the ULN, and the Endocrine Society recommends a TRAb cutoff level two to three times the ULN, based on current literature (13,14). This is in line with the results of this review.
Strengths and weaknesses of this study
This is the first review in which all available literature on maternal TRAb levels and the development of fetal and/or neonatal thyrotoxicosis is summarized. A comprehensive search was performed in the PubMed database with the assistance of a clinical librarian. The selection based on title and abstract was carried out by two independent researchers. A third researcher was asked for advice in case of a disagreement. Furthermore, the quality of all included articles was assessed using validated checklists.
The included cohort studies describe a prevalence of neonatal thyrotoxicosis of 2–20%. A prevalence of 20% is exceptionally high from a clinical perspective and strongly suggests inclusion bias. On the other hand, fetal thyrotoxicosis may not always be recognized as a cause of intra-uterine fetal death, leading to underestimation. Considering the relatively low incidence of fetal death in the third trimester, the extent of underestimation is very limited.
The use of different generation assays in included studies made it difficult to compare the obtained data. Currently, available assays can be subdivided in two main groups: bio-assays and radio-receptor assays (39). Bio-assays are functional assays, measuring the stimulatory or inhibitory activity of antibodies. Radio-receptor assays detect maternal TRAb, without differentiation between stimulatory or inhibitory activity. All radio-receptor assays are based on the competitive binding of TSH receptors. They can be subdivided in three generations (40). In this review, only studies using radio-receptor assays were included. These assays are used most frequently internationally because of their wide availability (39). Bioassays are important tests to determine the stimulating or blocking capacity of TRAbs. However, they are not widely available, and they time-consuming and expensive. Therefore, a strategy achievable in daily practice is suggested: screening at-risk patients by measuring TRAbs. If the patient is euthyroid, a maternal serum determination of thyroid-stimulating immunoglobulin (TSI) could be valuable, but there are no data available to support the assumption that screening for fetal/neonatal can be omitted with TSI assays if the TRAb shows no stimulatory effect.
A complicating factor is the difference between same generation assays manufactured by different companies. The included studies used assays of different manufacturers. Some assays expressed TRAb levels in U/L, while other assays provided TRAb levels in IU/L, U/mL, or percentages. Reference ranges also differed between assays of different manufacturers.
In some studies, the assay used for measurement of maternal TRAb levels was not clearly described. The heterogeneity and the frequently poor documentation of the assays used in studies complicated the comparison of results. Therefore, conclusions have to be interpreted with caution.
Another limitation of this study is the definition of fetal/neonatal thyrotoxicosis, which has been used in the included studies. In all studies, neonatal thyrotoxicosis was diagnosed based on elevated levels of free thyroxine (fT4) and/or free triiodothyronine (fT3) and suppressed TSH levels. Sometimes, clinical symptoms of neonatal thyrotoxicosis were described or ultrasounds of the neonatal thyroid gland were performed. The definition of Graves' disease also differed between studies. In some studies, women were included based on clinical symptoms or medical history, while other studies included women if fT4 and/or fT3 were elevated and TSH levels were suppressed or TRAb levels were positive.
Normal values of thyroid hormone levels in pregnancy differ from normal values in non-pregnant women (41). This was taken into account in seven studies, in which reference ranges for pregnant women were used (18,24,26,30,31,36,37). In four studies, reference ranges of non-pregnant women were used for pregnant women (16,27,28,38). This could also create a difference in definition of Graves' disease used in various studies.
Implications for research and clinical practice
Future research is needed to determine an evidence-based threshold for maternal TRAb above which additional screening for fetal and/neonatal thyrotoxicosis is necessary. The heterogeneity of studies must be reduced by the use of one general assay and by determination of TRAb levels at more specific moments in pregnancy. Additional research is necessary to determine the most appropriate moment for assessment of maternal TRAb levels.
Conclusion
The lowest level of maternal TRAb, measured with a second-generation assay and leading to neonatal thyrotoxicosis was 4.4 U/L or a ULN of 3.7. This review presents a thorough and clear overview of all available literature. Considering the low to moderate level of evidence, this conclusion should be interpreted with caution.
Footnotes
Author Disclosure Statement
The authors have no potential conflicts of interest to disclose.