
Abstract
Background:
The extent of metastatic lymph node (LN) invasion was not considered in the postoperative stratification of the recurrence risk of papillary thyroid carcinoma (PTC) in the 2015 American Thyroid Association (ATA) guidelines, and the recommended risk stratification cannot be applied to individuals. A nomogram based on these risk factors was developed based on the risk factors to predict individual recurrence risk.
Methods:
Data from 1788 PTC patients at the West China Hospital and 306 cases from the Shang Jin Nan Fu Hospital between August 2013 and July 2015 were included in this study. The 1788 cases were randomized into two groups—the training set (896 cases) and the testing set (896 cases)—and 306 cases were used as the external evaluation set.
Results:
Univariate and multivariate analyses identified the following independent prognostic factors associated with recurrence in the three independent sets and the combined set (p < 0.01): LN invasion in the capsule or organ, more than five metastatic LNs, and a largest metastatic LN diameter >3 cm. Importantly, PTC patients showed significantly different recurrence rates depending on the extent of LN invasion in the three sets and in the combined set (p < 0.001). The nomogram was developed based on the risk factors in the training set and was validated in the independent testing and validation sets.
Conclusion:
The largest LN metastasis diameter, number of metastatic LNs, and the extent of extranodal invasion had significant prognostic value for predicting the risk of recurrence. Based on the characteristics of the thyroidal PTC lesion and metastatic LNs, the nomogram showed good prediction of recurrence in individual PTC patients.
Introduction
P
Many studies have included the number and the largest diameter of LN metastases and extranodal extension (5), but other important characteristics of PTC recurrence or persistent disease, such as the degree of extranodal extension (i.e., invasion of the internal jugular vein or carotid artery), associated with an increased risk of recurrent/persistent disease (4,6,7) are not included in the risk for structural PTC recurrence. Therefore, it was hypothesized that LN metastasis should be subdivided into multiple strata in order to refine recurrence predictions (8). Additionally a nomogram was established to predict PTC recurrent/persistent disease in the lateral compartment in PTC patients by obtaining a specific estimate of risk.
Methods
The present study enrolled three independent sets of PTC patients from two independent medical centers. The inclusion criteria were an age between 18 and 70 years and histologically confirmed PTC. The exclusion criteria were other thyroid cancers, including medullary/follicular/anaplastic thyroid carcinomas, and other previous neck cancers. Ultimately, 1788 patient with PTC who underwent thyroid surgery at West China Hospital (Wuhou, Sichuan, China) from August 2013 to July 2015 (excluded cases before this period due to high rate of lost follow-up and after that due to short term follow-up) were included in the study and randomized into two groups using the sealed envelope method (
The patient list was filtered and derived from the computer center. Missing clinical information was retrospectively collected for each patient from the HIS Medical System. The pathology reports were independently reviewed by two thyroid pathologists, and the characteristics of the thyroidal PTC lesion were recorded according to the AJCC 7th edition/TNM classification system for differentiated thyroid carcinoma (2). However, LN metastasis is only divided into two grades (N1a and N1b) by the AJCC system, which may not be sufficient to include all factors involved in LN metastasis and to predict recurrence precisely. Therefore, the focus was primarily on metastatic LN characteristics, including the numbers and the locations of the overall dissected LNs and the metastatic LNs. The cutoff values for metastatic LN numbers and the largest diameters were based on the stratification system for the risk of persistent/recurrent disease in the 2015 ATA guidelines (2). It was hypothesized that metastatic LN extranodal invasion can be divided into subgroups similar to thyroidal PTC lesions according to the TNM stage using the following five grades: no invasion (grade 0); capsular invasion (grade 1); minimal extension into perithyroidal soft tissues (grade 2); invasion of the subcutaneous soft tissues, larynx, trachea, esophagus, recurrent laryngeal nerve, vagus nerve, or accessory nerve (grade 3); and invasion into the prevertebral fascia or encasing the carotid artery/vein or mediastinal vessels (grade 4).
The main surgical protocols for PTC at the two centers include unilateral lobectomy with routine ipsilateral central compartment LN dissection, total thyroidectomy with at least ipsilateral central compartment LN dissection, and therapeutic lateral compartment LN dissection (with fine-needle aspiration cytology or a thyroglobulin assessment to confirm metastasis). The details of the surgical procedures and postoperative adjuvant therapies were introduced in a previous study (9). Every suspicious metastatic LN was evaluated to determine the metastasis status, and the largest diameter was measured by two independent experienced pathologists. The extent of the invasion was mainly based on the intraoperative findings (operative documents) and microscopic observations.
All patients agreed to participate in at least two years of follow-up in the outpatient center. The main clinical outcomes were evaluated and recorded, including classification of the response to therapy, with a particular focus on the structural incomplete response responsible for up to 85% of recurrence cases, 11% of disease-specific deaths, and 50% of distant metastases according to the ATA guidelines (2).
Statistical analyses
Statistical analyses were performed using IBM SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY). Univariate and multivariate regression analyses were used to identify independent prognostic factors in the three sets of patients. A p-value of <0.05 was defined as the criterion for variable deletion when performing backward stepwise selection. Based on the identified risk factors, a nomogram of risk factors associated with recurrence was established with the R software studio (R Foundation, Vienna, Austria). The predictive performance of this model was evaluated and validated using the concordance index (C-index). Receiver operating characteristic (ROC) curves were used to evaluate and compare the recurrence prediction abilities for thyroidal PTC lesions and metastatic LNs. A p-value of <0.05 in a two-tailed test indicated a significant difference.
Results
Patients and PTC characteristics
The characteristics of the three sets of patients are summarized in Table 1. The patients were divided into two groups based on age, using 45- and 55-year-old cutoff values according to the 7th and 8th AJCC staging systems. A few patients underwent BRAFV600E mutation testing, and the mutation rates were 39.8%, 41.3%, and 36.8% in the training, testing, and validation sets, respectively. The metastatic LN invasion rates in the capsule were 39.3%, 40.0%, and 37.9%, respectively, in the three sets, and the metastatic LN invasion rates into the surrounding tissues or organs were 27.6%, 28.9%, and 29.4%. Overall, these three sets of patients were comparable relative to the PTC patient demographic and tumor characteristics.
PTC, papillary thyroid carcinoma; SD, standard deviation; T, tumor invasion depth; N, lymph node involvement, TNM, tumor, node, metastasis; LN, lymph node.
Univariate and multivariate analysis of recurrence
The univariate Cox regression analysis included potential risk factors defined in the previous ATA reports and guidelines. The study focused on the PTC and metastatic LN characteristics shown in Table 2. The factors that were significantly associated with PTC recurrence were male sex and being in the training set but not being in the testing and validation sets. The T classification was only significant in the training and testing sets. Other factors that were significant in the three sets included the tumor number, tumor size, number of metastatic LNs, the largest LN diameter, and metastatic LN capsular and organ invasion (p ≤ 0.001). Variables were included in the multivariate analysis if they potentially predicted PTC recurrence. A tumor size ≥2 cm with LN capsular invasion in the training set, multiple foci of PTC in the testing set, and pathological LN metastasis in the validation set were not significant (p > 0.05). As shown in Table 3, in the pooled analysis, LN invasion in the capsule or into other organs, more than five metastatic LNs, and a largest metastatic LN diameter of >3 cm were also identified as independent prognostic factors associated with recurrence in the combined set. These results support the hypothesis that metastatic LN characteristics can be used to predict PTC recurrence.
p < 0.05; ** p < 0.01.
Excluding the pN0 cases.
Including the pN0 cases.
HR, hazard ratio; CI, confidence interval; T, tumor invasion depth; N, lymph node involvement.
p < 0.05; ** p < 0.01.
Comparison of the thyroidal PTC lesion and metastatic LN characteristics for recurrence prediction
For this comparison, the three sets were included as a pool based on the multivariate analysis results shown in Figure 1. Metastatic LNs showed better predictive ability (larger area under the ROC curve) than that of PTC lesions for PTC recurrence (PTC largest diameter vs. metastatic largest LN diameter [area under the curve (AUC): 0.729 vs. 0.836; Fig. 1A], number of PTC foci vs. total metastatic LN number [AUC: 0.580 vs. 0.902; Fig. 1B], PTC capsule invasion vs. metastatic LN capsule invasion [AUC:0.597 vs. 0.678; Fig. 1C], and organ invasion by the PTC vs. metastatic LN organ invasion [AUC: 0.625 vs. 0.765; Fig. 1D]). Taken together, these results indicate that the metastatic LN characteristics show greater value for the prediction of PTC recurrence than the PTC lesions in the thyroid.
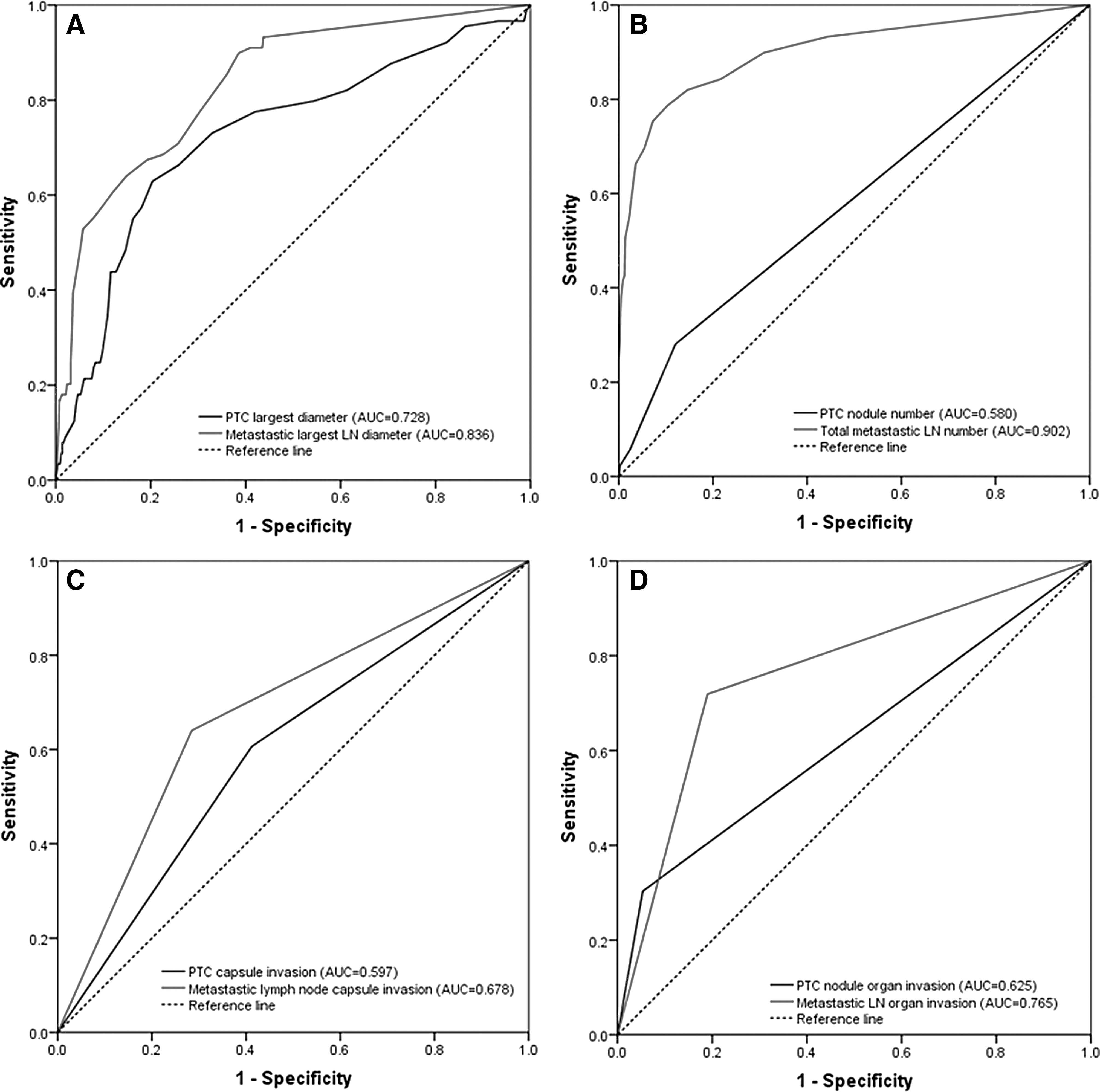
Comparison of the effectiveness of thyroidal papillary thyroid carcinoma (PTC) lesion and metastatic lymph node (LN) risk factors for the prediction of PTC recurrence. In the combined cohort, the largest diameter (
Relationship between PTC lesions in the thyroid gland and metastatic LN
Next, the relationship was evaluated between the PTC lesion with the largest diameter in the thyroid gland and the LN with the largest diameter metastasis, as shown in Figure 2. No linear relationships were found in the training set (Fig. 2A; R 2 = 6.557E-6), the test set (Fig. 2B; R 2 = 0.057), or the validation set (Fig. 2C; R 2 = 0.051). When all three sets were combined into a pool, no linear relationship was observed (Fig. 2D; R 2 = 0.001). These results indicate that metastatic LN nodule diameters are independent of the largest PTC lesion in the thyroid gland. Therefore, an independent evaluation of metastatic LN characteristics, including the extent of invasion, is essential.
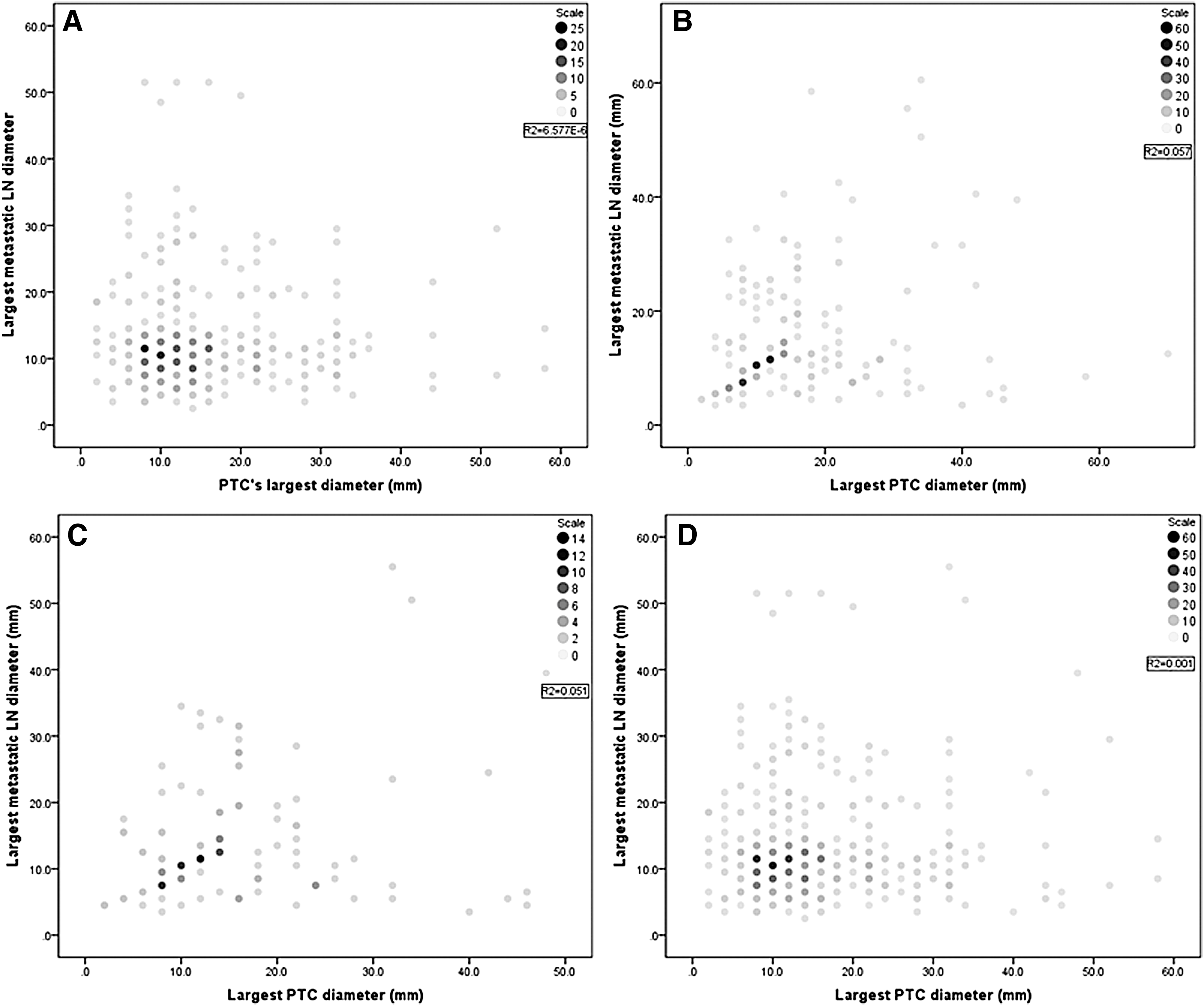
Linear correlation analysis between the PTC lesion and largest diameter of metastatic LN. No linear relationship was observed in the training (
PTC recurrence-free survival
Based on the hypothesis, the PTC tumor-free survival rates were compared among the five subgroups (based on the metastatic LN invasion grade) in the testing, training, validation, and combined sets, as shown in Figure 3A–D. Significant differences were observed among these subgroups in the three sets and in the combined set (p < 0.001). Grade 3 or 4 LN invasion may significantly increase the risk of PTC recurrence or metastasis. The PTC-free survival rate comparison further confirmed the necessity of assigning PTC cases with LN metastases to subgroups and validated the accuracy of the classification.
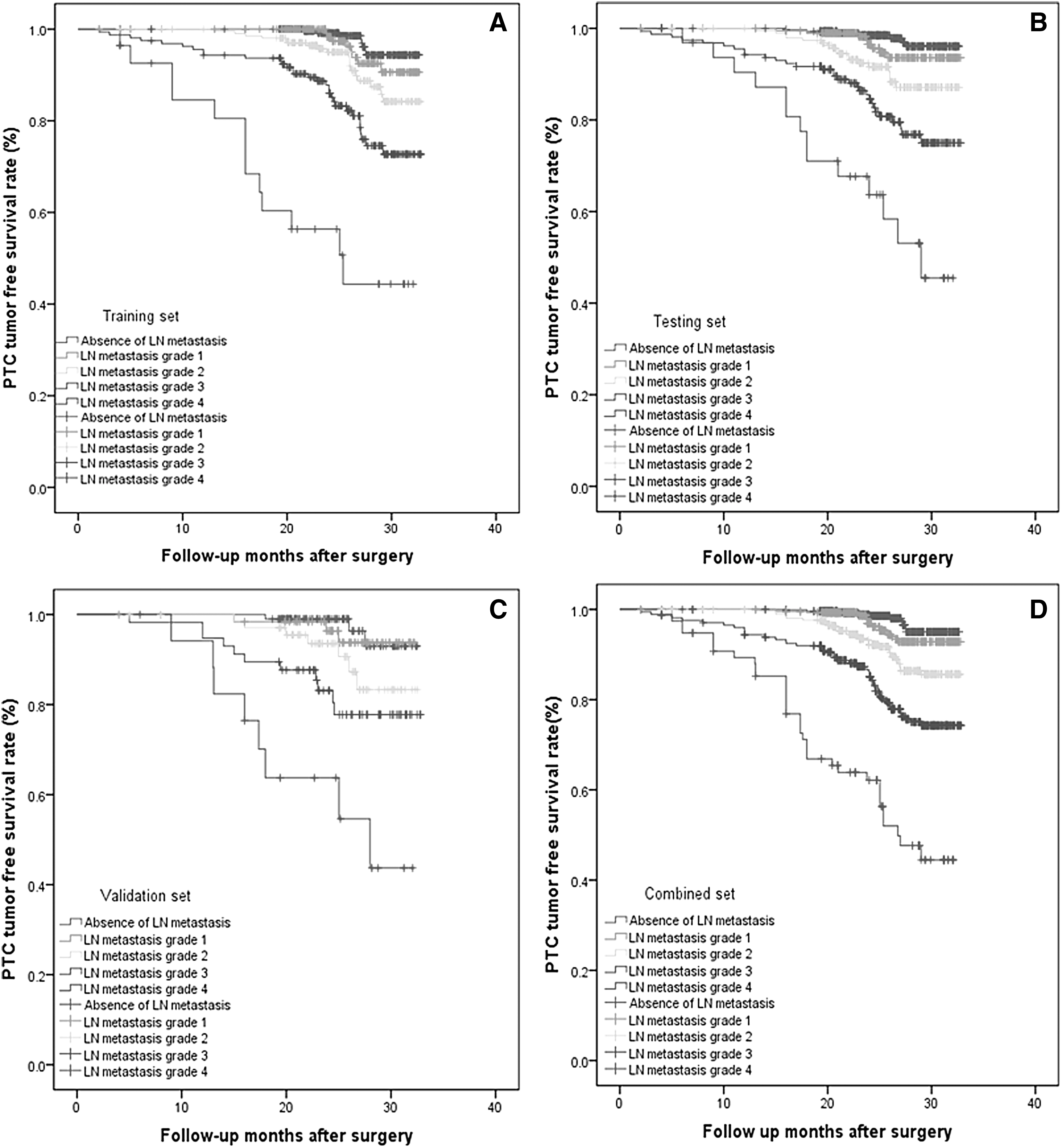
Comparison of tumor-free survival among PTC patients with different grades of metastatic LN invasion. A correlation with more advanced extranodal extension and lower PTC-free survival were observed in the training (
Nomogram for predicting PTC recurrence
All risk factors that showed statistical significance were included in the nomogram. The pN classification, LN capsular invasion, and LN organ invasion were combined into one factor (the LN invasion grade). Thus, five factors were ultimately used to build the nomogram in the training set. As shown in Figure 4, the ability to predict a recurrence was stronger based on the analysis of metastatic LN characteristics compared to the characteristics of the thyroidal PTC lesion(s). For individual PTC patients, the risk of early recurrence was calculated using the data for these five risk factors. A line can be drawn upward for each risk factor (lines 2–6) to acquire point values (line 1). Then, the sum of all five points can be plotted on the total point axis (line 7), and a line can be drawn downward to the risk axis (line 8). Then, the risk of recurrence can be calculated for an individual patient. In the internal (testing set) and external validation cohorts (validation set), the C-indexes of the PTC recurrence nomogram were 0.81 [confidence interval (CI) 0.71–0.89] and 0.78 [CI 0.72–0.85], respectively. Therefore, the proposed nomogram performed well in all PTC cases.
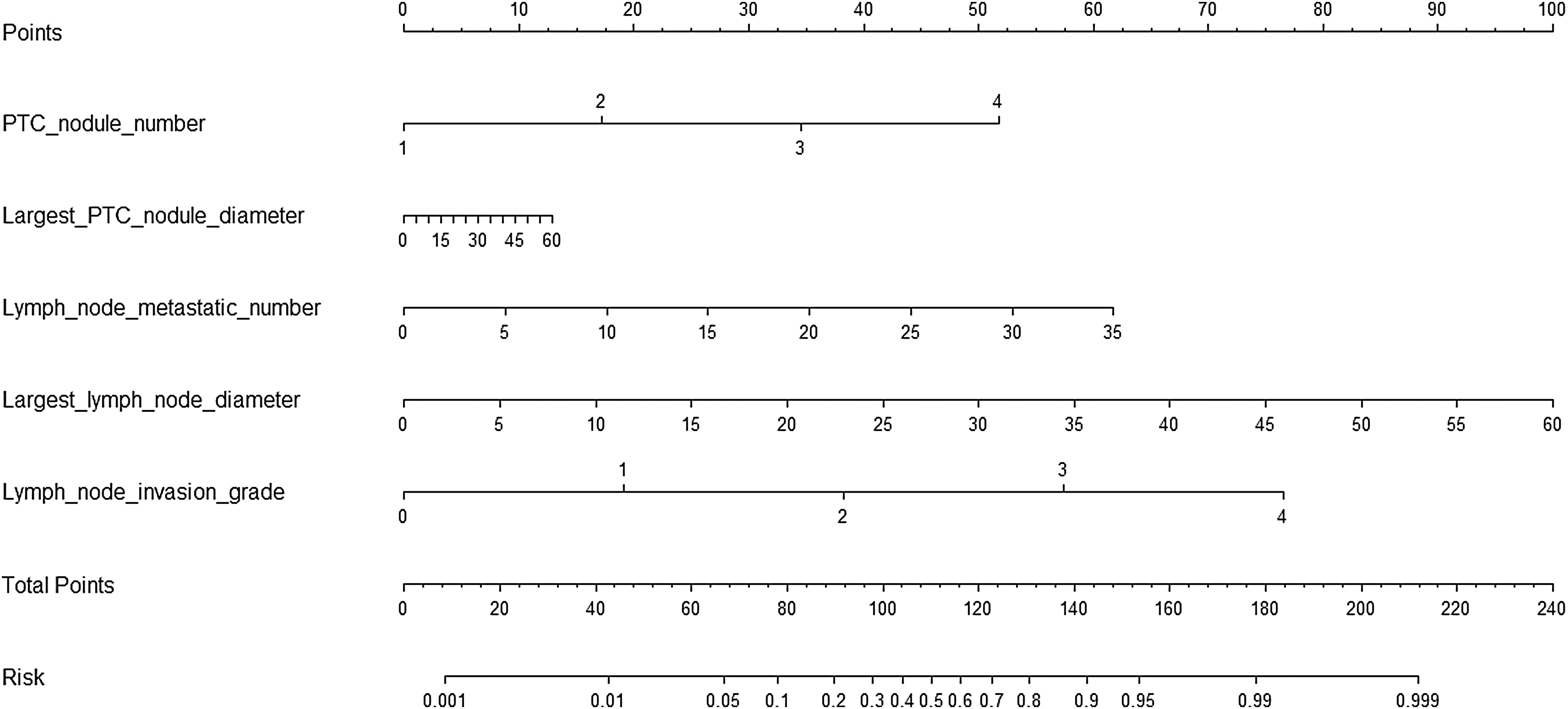
Nomogram for the prediction of PTC recurrence. To use this nomogram in individual patients, the information for five (axes 2–6) risk factors should be visualized as a point on the first axis. Then, the sum of these five points out of the total number of points should be plotted on axis 7. Then, a line is drawn downward toward the risk axis (axis 8) to determine the likelihood of recurrence for an individual patient.
Discussion
The present study found that metastatic LN characteristics are independent of the thyroidal PTC lesion and could be used to predict the risk of PTC recurrence. Moreover, the ability to predict a recurrence was stronger based on the analysis of metastatic LN characteristics compared to the characteristics of the thyroidal PTC lesion. Based on these risk factors, a recurrence nomogram was developed to predict the risk of recurrence for individual patients. More attention should be paid to metastatic LN characteristics, such as the number of metastatic LNs involved and the largest diameter of the metastatic LNs, as detailed in the 2015 ATA risk stratification system. Additionally, the extent of invasion of metastatic LNs may contribute to the risk for PTC recurrences.
This study may be considered in the context of several reports on the risk stratification of LN metastasis (4,10,11). However, some potentially important improvements were made in this study. First, this is one of the largest cohort analyses on this topic. Second, all of the results were tested in an internal cohort of patients and validated in an external cohort of patients. Third, a characteristic relationship was not detected between the original PTC lesion and metastatic LNs. LN subgroups were generated based on five grades according to the extent of invasion, and significant differences were found in PTC recurrence. Fourth, the numbers and the largest diameter of the thyroidal PTC lesion(s) and metastatic LN(s) could be used to predict the risk for recurrence. It was discovered that the metastatic LN numbers and largest diameters are better predictors for recurrence than the thyroidal PTC lesion(s). Finally, a nomogram was developed based on the risk factors that could be used to calculate individual patients' recurrence risks.
Postoperative staging is very important in the assessment of the recurrence risk and in decision making regarding follow-up protocols and adjuvant therapies, such as thyrotropin suppressive therapy and 131I radiotherapy. The AJCC/UICC TNM classification system is generally applied for PTC staging, but the TNM classification system only distinguishes N1a (central LN metastases) from N1b (lateral neck metastases) and does not consider the characteristics of metastatic LNs. The MACIS system has the same limitation. Compared to the 2009 ATA guidelines (3), the 2015 ATA guidelines include characteristics of LN metastasis, such as the largest size and the number of metastatic LNs, but not extent of invasion (2). The present results show that these three risk factors should be included in staging systems to predict recurrence risk accurately.
According to previous studies, the recurrence risk for pN1 PTC patients can vary from as low as 3–4% in patients with a small number of LN metastases to as high as 32% in patients with a large volume of locoregional LN metastases (4,6). However, the cutoff for LN size varies, with some studies using cutoff values of 0.2 cm (12), 1 cm (13), and 3 cm (5), although most previous studies used 3 cm cutoff values. Ito et al. (14) demonstrated that neck LNs with a large size >3 cm were associated with poorer disease-free survival than PTC patients with small metastatic LNs. In a 10-year follow-up study, Sugitani et al. (15) demonstrated that the risk of recurrence was significantly higher in pN1 PTC patients with largest metastatic LNs >3 cm compared to patients with pN1 LNs <3 cm (27.0% vs. 11.0%). This cutoff value was adopted by the 2015 ATA guidelines (2). Based on univariate and multivariate analyses in the present study, it is concluded that the diameters of metastatic LNs represent one risk factor for PTC recurrence and should be considered in recurrence risk stratification. In the nomogram, the impact of the largest metastatic LN was repeatedly evaluated and might offer a specific risk estimation for individual PTC cases, which is impossible for dichotomous categories (such as ≤0.2 cm, >0.2 cm (12); ≤1 cm, >1 cm (13); or ≤3 cm, >3 cm (5)).
A greater number of LN metastases is also positively associated with a higher risk of recurrence, as reported in previous studies. For instance, Leboulleux et al. reported that the risk of recurrence was 21%, 7%, and 3% in cases with >10, 6–10, and <5 metastatic LNs, respectively. Ito et al. (16) indicated a cutoff value of ≥10 LN metastases for an increased risk of recurrence, and Sugitani et al. (15) and Ito et al. (14) demonstrated that the risk of recurrence in patients with more than five LN metastases was significantly higher than the risk in patients with fewer than five LN metastases; this cutoff value was adopted by the 2015 ATA guidelines. When this study focused on comparing the thyroidal PTC lesions and LN metastases with the largest diameters and intrathyroidal number of foci for the prediction of PTC recurrence, the characteristics of metastatic LNs showed the best predictive value. Therefore, more attention should be paid to metastatic LN characteristics in the postoperative recurrence stratification.
The extranodal extension of cervical LN metastases was also considered in the risk of recurrence analysis (4,6,17). However, to the best of the authors' knowledge, no published study has evaluated subgroups. The thyroidal PTC lesion can be classified into four grades according to the extent of invasion. Therefore, it was hypothesized that metastatic LN invasion can also be divided into four subgroups based on different stages. Minimal invasion was categorized as N1 (capsular invasion) and N2 (minimal extranodal extension). The PTC tumor-free survival comparison in Figure 3 confirmed the hypothesis because different stages of extranodal LN extension showed significantly different PTC recurrence rates, as shown in the nomogram.
This study has several limitations. First, the focus was on the evaluation of PTC recurrences, but overall survival was not evaluated due to the limited follow-up period. Different results could emerge with longer follow-ups, such as the long-term impact of the number of metastatic LNs on overall survival in Surveillance, Epidemiology, and End Results data for differentiated thyroid cancer (18). Further long-term follow-up is thus needed for the PTC patients. Even with the extensive two-center data analysis, larger cohorts and data from multiple centers may be needed to obtain a more objective conclusion. Lastly, the nomogram requires further validation in a large prospective cohort of PTC cases.
In conclusion, this study found that the recurrence-free survival of PTC patients might be significantly affected by the number of metastatic LNs, the largest metastatic LN diameter, and the extent of extranodal invasion. These characteristics were significantly more important than the characteristics of the thyroidal PTC lesion. The nomogram objectively and accurately predicted the risk for PTC recurrence in individual cases.
Footnotes
Acknowledgments
This study was supported by grants from National Key R&D Program of China (2017YFC0907504), National Natural Science Foundation (81702646), Sichuan Province Science and Technology Project of China (No. 2017SZ0139), Sichuan University for youth fund (2017SCU11016), Health and Family Planning Commission of Sichuan Province (17PJ398), and Postdoctoral Sustentation Fund of Sichuan University (2017SCU12035).
Author Disclosure Statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.