
Abstract
Introduction:
Risk-stratified treatment strategies have become a focus in the treatment of differentiated thyroid cancer (DTC). In the 2015 American Thyroid Association treatment guidelines, adjuvant treatment with radioactive iodine (RAI) is considered in the presence of minimal extrathyroidal extension (mETE). This study aimed to investigate the prognostic significance of mETE and tumor size in patients with DTC.
Methods:
A retrospective review was undertaken of 2323 consecutive patients treated surgically for T1–T3 (defined per seventh edition of the American Joint Committee on Cancer staging criteria) and M0 DTC from 2000 to 2015 at The University of Texas MD Anderson Cancer Center. Patients were divided into four groups according to the size of the tumor (≤4 cm vs. >4 cm) and the presence of mETE. Predictors of disease-free survival (DFS), disease-specific survival, locoregional failure (LRF), and distant metastatic failure (DMF) were compared using the log-rank test and Cox's proportional hazards models.
Results:
There were only seven DTC-related deaths, limiting the clinical significance of the analysis, especially of overall and disease-specific survival. Following multivariate analysis, patients with tumors >4 cm did worse than patients with tumors ≤4 cm with respect to DFS (group 3 [>4 cm without mETE] adjusted hazard ratio (HRadj) = 2.1 [confidence interval (CI) 1.1–3.8]; group 4 [>4 cm with mETE] HRadj = 2.9 [CI 1.6–5.1]). However, patients did not differ according to DFS, regardless of the presence of mETE within each size category (group 2 [≤4 cm with mETE] vs. group 1 [≤4 cm without mETE] HRadj = 1.3 [CI 0.9–1.8]; group 4 [>4 cm without mETE] vs. group 3 [>4 cm with mETE] HRadj = 1.0 [CI 0.5–2.3]). For LRF and DMF, size but not mETE was also an independent risk factor.
Conclusion:
Tumor size, but not the presence of mETE, was an independent predictor of DFS, LRF, and DMF in DTC.
Introduction
R
Pathologic diagnosis of mETE is challenging, resulting in inconsistencies reporting its presence (4,5). Though poor disease outcome has been demonstrated in patients with gross extrathyroidal extension (extensive visceral or soft tissue extension) (6), the prognostic importance of mETE remains controversial (7 –12). This study aims to elucidate the prognostic significance of the presence of mETE and its interaction with size in patients with DTC.
Methods
After obtaining Institutional Review Board approval, a retrospective review of the institutional tumor registry was conducted for patients surgically treated for DTC at the University of Texas MD Anderson Cancer Center (MDACC) from 2000 to 2015. Patients aged ≥18 years undergoing definitive primary surgery at MDACC and pathologically diagnosed with a T1–T3 tumor according to the seventh edition of the AJCC Cancer Staging Manual (3) were included in the study. Patients with distant metastatic disease at initial assessment or follow-up of <6 months were excluded.
Baseline demographic data (age, sex, and race/ethnicity) and pathologic data (histology, tumor size, margin status, lymphovascular invasion, perineural invasion, capsular invasion, pathological N classification, and presence of extrathyroidal extension) were collected. mETE was defined as tumor extension to the perithyroidal soft tissue or strap muscles, according to the seventh edition of AJCC Cancer Staging Manual (3). Extent of surgical treatment along with adjuvant treatment with RAI and external beam radiation were recorded.
Patients were divided into groups based on two criteria for pathologic T3 classification: (i) size and (ii) presence of mETE. Thus, four study groups were identified: group 1 (≤4 cm/–ETE): size ≤4 cm without the presence of mETE; group 2 (≤4 cm/+ETE): size ≤4 cm with the presence of mETE; group 3 (>4 cm/–ETE): size >4 cm without the presence of mETE; and group 4 (>4 cm/+ETE): size >4 cm with the presence of mETE.
The primary outcome measure was disease-free survival (DFS). This was defined as time from initial surgery for thyroid cancer to time of recurrence or death from any cause. Overall survival (OS), time from initial surgery to death from any cause, and disease-specific survival (DSS), time from initial surgery to death from thyroid cancer, were also calculated. The recurrence rate was determined using locoregional failure (LRF), defined as the time from initial surgery to locoregional recurrence, and distant metastatic failure (DMF), defined as the time from initial surgery to distant metastatic disease detection. Locoregional recurrence was defined as recurrent structural disease with biopsy confirmation, although in a few cases with convincing radiographic findings, locoregional failure was not confirmed pathologically.
Statistical analysis
Descriptive statistics, including mean, median, standard deviation, and range, were obtained for all baseline characteristics. Continuous variables were compared using one-way analysis of variance and categorical variables with the chi-square test or Fisher's exact test, as appropriate. The Kaplan–Meier method was employed for all survival analyses and compared with the log-rank test. Cox's proportional hazards model was used for univariate and multivariate analysis to investigate predictors of survival. Candidate disease covariates for inclusion in the final model were study group, age at diagnosis, sex, race/ethnicity, tumor morphology, pathologic N classification, presence of extranodal extension, and presence of lymphovascular invasion.
All variables with a p-value of <0.05 in the univariate analysis were included in the multivariate model. To investigate the possibility that other tumor size cutoffs might be better predictors of survival, multivariate models were created using new study groups defined with 2 and 3 cm tumor size cutoffs. The Akaike information criterion (AIC) was used to compare between models, and the model demonstrating best goodness of fit was used as the final model (13). All tests were two-tailed, and alpha was set to 0.05 for significance. All statistical analyses were completed using SAS JMP Pro v12.1.0 (SAS Institute, Cary, NC).
Results
Baseline group characteristics
A total of 2323 patients met the inclusion criteria (Fig. 1). Of these patients, 978 (42%) patients had pathological T3 tumors, and 1345 (58%) had pathological T1–T2 tumors. Baseline characteristics for all patients and by study group are delineated in detail in Table 1. The median follow-up for all patients was 57 months (range = 6–192 months) and statistically significantly longer for patients in group 1 (≤4 cm/–ETE; p < 0.001) compared to those in group 2 (≤4 cm/+ETE; median = 63 months; range = 6–192 months), but all other between-group comparisons did not demonstrate a statistically significant difference.
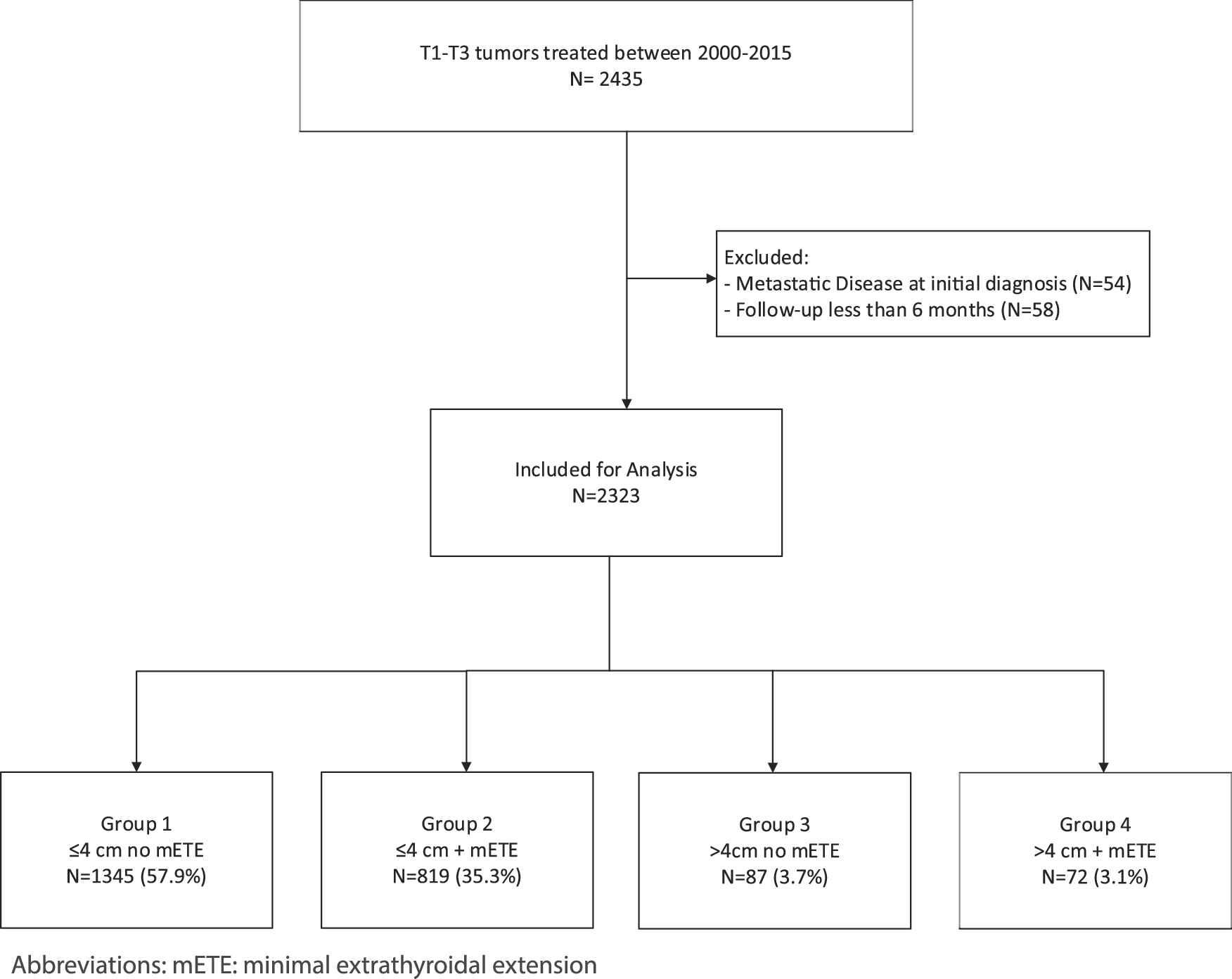
Patient flow chart of patients included in the study.
Group 1: size ≤4 cm without the presence of mETE; group 2: size ≤4 cm with the presence of mETE; group 3: size >4 cm without the presence of mETE; and group 4: size >4 cm with the presence of mETE.
p-Value for one-way analysis of variance or chi-square test, as appropriate.
Median (range).
mETE, minimal extrathyroidal extension.
Patients with tumors having mETE (group 2 [≤4 cm/+ETE] and group 4 [>4 cm/+ETE]) were more likely to have nodal disease (p < 0.001); large tumors with mETE (group 4 [>4 cm/+ETE]) were more likely to demonstrate lymphovascular invasion (p < 0.001). Large tumors without mETE (group 3 [>4 cm/–ETE]) were more likely to be follicular carcinomas compared to other groups (p < 0.001).
Extent of treatment
The extent of surgical and adjuvant treatment is summarized in Table 2. Patients with the presence of mETE (group 2 [≤4 cm/+ETE] and group 4 [>4 cm/+ETE]) were statistically more likely than those without mETE (group 1 [≤4 cm/–ETE] and group 3 [>4 cm/–ETE]) to undergo total thyroidectomy or completion thyroidectomy (97% vs. 87%; p < 0.001), and central (84% vs. 39%; p < 0.001) or lateral neck dissection (38% vs. 12%; p < 0.001). In patients with small tumors without mETE (group 1 [≤4 cm/–ETE]), adjuvant RAI was less likely to be delivered compared to patients with small tumors with mETE (group 2 [≤4 cm/+ETE]; 42% vs. 72%; p < 0.001). Patients in the remaining groups (groups 2–4) had no statistically significant difference in rate of RAI treatment (72% vs. 72% vs. 82%; p = 0.432).
Group 1: size ≤4 cm without the presence of mETE; group 2: size ≤4 cm with the presence of mETE; group 3: size >4 cm without the presence of mETE; and group 4: size >4 cm with the presence of mETE.
p-Value for chi-square test.
Includes patients undergoing total thyroidectomy or lobectomy with completion thyroidectomy.
RAI, radioactive iodine; EBRT, external beam radiotherapy.
Survival by study group
Five-year DFS by study group was 94% in group 1 (≤4 cm/–ETE), 91% in group 2 (≤4 cm/+ETE), 83% in group 3 (>4 cm/–ETE), and 71% in group 4 (>4 cm/+ETE; p < 0.001; Fig. 2A). Five-year OS was 96% for group 1 (≤4 cm/–ETE), 97% for group 2 (≤4 cm/+ETE), 91% for group 3 (>4 cm/–ETE), and 98% for group 4 (>4 cm/+ETE; p = 0.667). Five-year DSS was 100% for group 1 (≤4 cm/–ETE), 100% for group 2 (≤4 cm/+ETE), 97% for group 3 (>4 cm/–ETE), and 98% for group 4 (>4 cm/+ETE; p < 0.001; Fig. 2B).
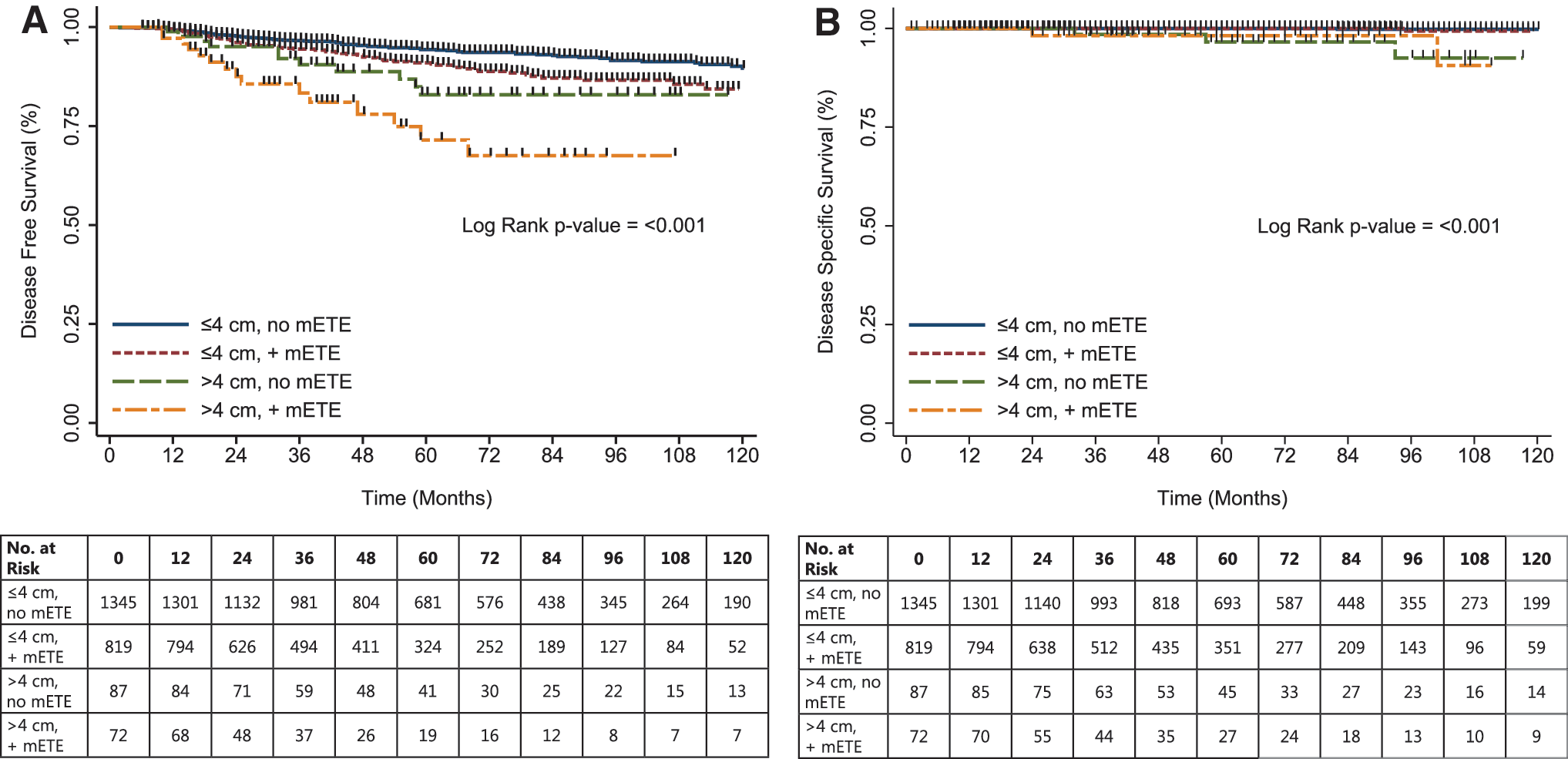
Kaplan–Meier analysis for disease-free survival (
The numbers of patients with locoregional and distant metastases were 20 (1%) and 5 (0.4%) in group 1 (≤4 cm/–ETE), 34 (4%) and 13 (2%) in group 2 (≤4 cm/+ETE), 6 (7%) and 4 (5%) in group 3 (>4 cm/–ETE), and 11 (15%) and 6 (8%) in group 4 (>4 cm/+ETE), respectively. Five-year locoregional and distant metastasis are summarized in Figure 3. Locoregional and distant metastases were more common in patients in group 4 (>4 cm/+ETE) compared to the other groups (p < 0.001 and p < 0.001, respectively).
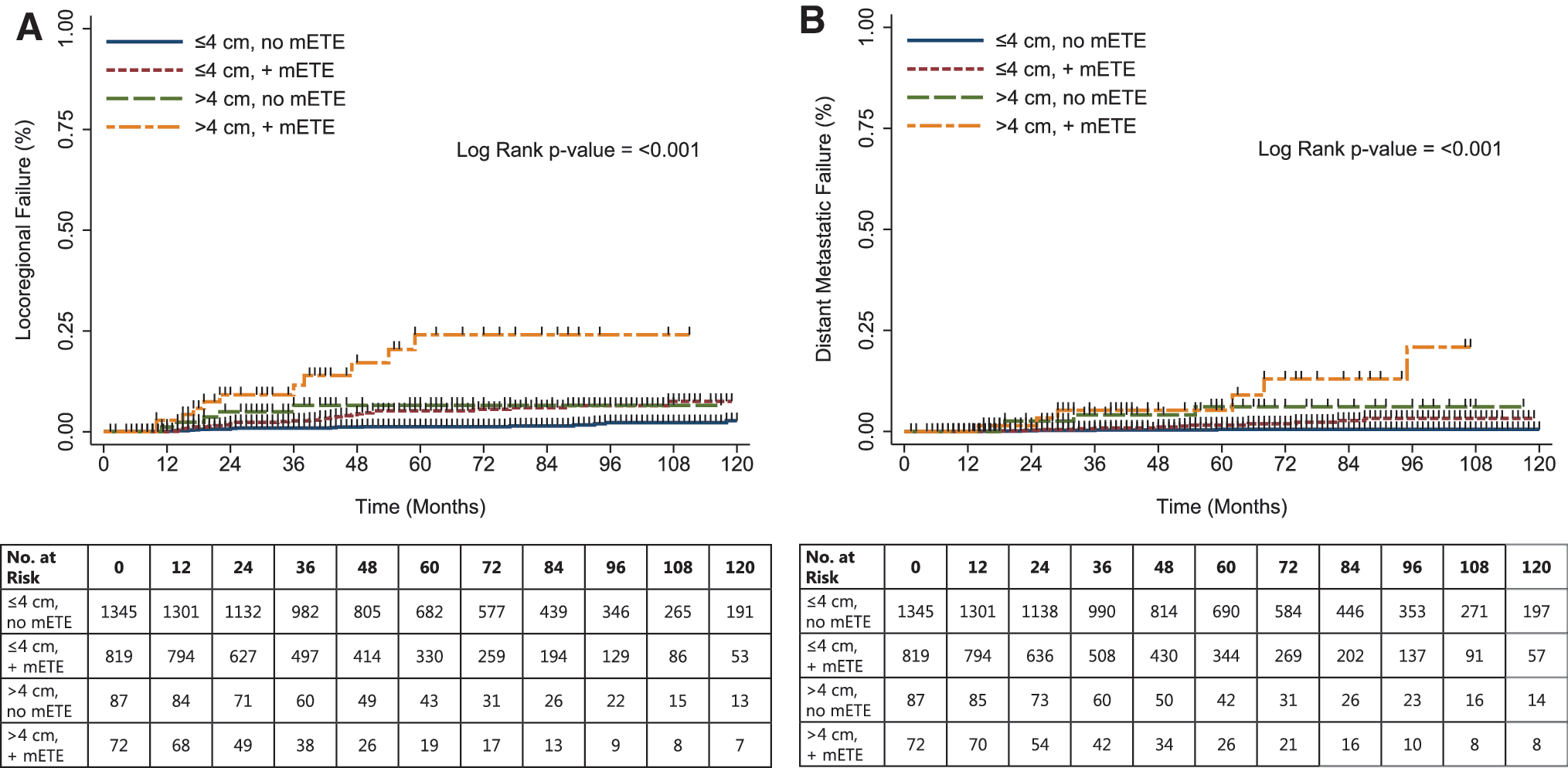
Kaplan–Meier analysis for locoregional (
Factors predicting DFS
On univariate analysis, increasing age (hazard ratio [HR] = 1.0 [confidence interval (CI) 1.0–1.1]), male sex (HR = 2.6 [CI 1.9–3.4]), pathological N classification (N1a: HR = 1.1 [CI 0.8–1.7]; N1b: HR = 2.6 [CI 1.9–3.6]), and the presence of extranodal extension (HR = 2.5 [CI 1.8–3.5]) were significant prognosticators of DFS and were included in the multivariate model. Patients with small tumors and mETE (group 2 [≤4 cm/+ETE], HR = 1.6 [CI 1.2–2.3]) and large tumors without mETE (group 3 [>4 cm/–ETE], HR = 2.3 [CI 1.2–4.2]) had impaired DFS compared to patients with small tumors without mETE (group 1 [≤4 cm/–ETE]). Comparing patients with large tumors and mETE (group 4 [>4 cm/+ETE]), both size and presence of mETE appear to have an additive effect on DFS (HR = 4.7 [CI 2.7–8.2]).
Comparing the multivariate models with 2, 3, and 4 cm tumor cutoffs, the model using the original 4 cm cutoff had the smallest AIC and was therefore used as the final model. In this final model, even with adjustment for age, sex, pathologic N classification, and presence of extranodal extension, the patient study group continued to be a statistically significant predictor of DFS (Table 3). Patients with small tumors did not do significantly worse with the presence of mETE (group 1 [≤4 cm/–ETE] versus group 2 [≤4 cm/+ETE]: adjusted HR [HRadj] = 1.1 [CI 0.8–1.5]). However, those with large tumors fared significantly worse compared to patients with smaller tumors (group 3 [>4 cm/–ETE] HRadj = 2.2 [CI 1.2–4.1]; group 4 [>4 cm/+ETE] HRadj = 2.4 [CI 1.3–4.2]). In those with large tumors, the presence of mETE did not result in a statistically significant difference in DFS (group 4 [>4 cm/+ETE] vs. group 3 [>4 cm/–ETE] HRadj = 1.0 [CI 0.5–2.3]).
Per year increase.
Adjusted for age, sex, study group, pN classification, and presence of ECS.
Adjusted for age, sex, study group, presence of ECS, and presence of lymphovascular invasion.
Adjusted for sex, study group, pN classification, presence of ECS, and presence of LVI.
N/A indicates that the variable was not included in the multivariate analysis, as the variable was not found to be a significant predictor of outcome on univariate analysis.
DFS, disease-free survival; DSS, disease-specific survival; LRF, locoregional failure; HRadj, adjusted hazard ratio; CI, confidence interval; ENE, extranodal extension; CI, 95% confidence interval.
Factors predicting DSS
Univariate analysis demonstrated that increasing age (HR = 1.1 [CI 1.0–1.1]), male sex (HR = 1.4 [CI 1.3–35.2]), presence of extranodal extension (HR = 10.3 [CI 2.3–46.0]), and presence of lymphovascular invasion (HR = 13.0 [CI 2.5–67.4]) were significant predictors of DSS. Patients with small tumors fared better than patients with larger tumors (group 3 [>4 cm/–ETE] HR = 46.6 [CI 4.8–447.9] and group 4 [>4 cm/+ETE] HR = 48.2 [CI 4.4–532.0]). However, there was no significant difference in DSS for patients with small tumors, regardless of presence of mETE (group 2 [≤4 cm/+ETE] HR = 2.1 [CI 0.1–34.0]).
Using these significant variables on univariate, multivariate analysis was completed (Table 3). The model using the original 4 cm tumor size cutoff demonstrated the smallest AIC and was therefore used as the final model. Increasing age (HRadj = 1.1 [CI 1.0–1.2]) and presence of extracapsular spread in the lymph nodes (HRadj = 39.6 [CI 4.1–378.4]) continued to be independent predictors of DSS. Following multivariate adjustment, patients with large tumors continued to have worse DSS, with large tumors without mETE having an HRadj = 62.8 [CI 4.2–940.2] and large tumors with mETE having an HRadj = 3.1 [CI 0.2–53.2].
Factors predicting LRF and DMF
For LRF, male sex (HR = 2.5 [CI 1.6–4.0]), pathologic N classification (N1a: HR = 3.2 [CI 1.6–6.4]; N1b: HR = 7.3 [CI 4.0–13.0]), presence of extracapsular spread in the lymph nodes (HR = 4.4 [CI 2.7–7.2]), and presence of lymphovascular invasion (HR = 3.1 [CI 1.9–5.1]) were significant on univariate analysis and included in the multivariate model (Table 3). On univariate analysis, patients in all study groups had a statistically significant higher rate of LRF compared to patients with small tumors without the presence of mETE (group 2 [≤4 cm/+ETE] HR = 3.4 [CI 2.0–6.0]; group 3 [>4 cm/–ETE] HR = 4.7 [CI 1.9–11.8]; group 4 [>4 cm/+ETE] HR = 14.3 [CI 6.8–30.1]). Multivariate models were compared according to tumor size cutoff, and the model using the original 4 cm cutoff had the smallest AIC and was accepted as the final model. Independent predictors of LRF identified were male sex (HRadj = 1.7 [CI 1.0–2.8]) and pathologic N classification (N1a: HRadj = 2.7 [CI 1.3–5.6]; N1b: HRadj = 3.8 [CI 1.9–8.1]). In patients with small tumors, the presence of mETE was not a predictor of LRF following adjustment, regardless of the presence of mETE (group 2 [≤4 cm/+ETE] HRadj = 1.8 [CI 0.9–3.3]). However, patients with large tumors experienced more events than those with small tumors (group 3 [>4 cm/–ETE] HRadj = 4.2 [CI 1.6–10.9]; group 4 [>4 cm/+ETE] HR = 4.6 [CI 1.9–10.8]). When considering only those with large tumors, no significant difference in LRF according to mETE was demonstrated following multivariate adjustment (group 4 [>4 cm/+ETE] vs. group 3 [>4 cm/–ETE] HR = 1.1 [CI 0.4–3.1]).
Findings from the univariate analysis for DMF are summarized in Supplementary Table S1 (Supplementary Data are available online at
Discussion
This study demonstrates that outcomes in T1–T3 DTC vary according to the presence of mETE and size. Univariate analysis demonstrates that both size and the presence of mETE have an additive effect on DFS. On multivariate analysis, age, sex, pathologic N classification, and the presence of extranodal extension were found to be independent predictors of DFS. After controlling for these disease covariates, size of tumor continued to be an independent predictor of DFS, but there was no difference within size groups regardless of the presence of mETE. Other recurrence-related outcomes measures, LRF and DMF, demonstrated similar findings on multivariate analysis, emphasizing the importance of size rather than mETE in determining risk for recurrent disease.
Conclusions regarding the effect of tumor size and presence of mETE on DSS were challenging due to the small number of events. Due to the generally excellent survival prognosis of patients with T1–T3 DTC, only seven patients experienced DTC-specific mortality, with one event in both group 1 (≤4 cm/–ETE) and group 2 (≤4 cm/+ETE), three events in group 3 (>4 cm/–ETE), and two events in group 4 (>4 cm/+ETE). Therefore, the precision of hazard ratio estimates is low, as demonstrated by wide confidence intervals. Though findings were statistically significantly different between groups, they represent differences of one or two DTC-specific deaths, which is not clinically significant. Longer-term follow-up or larger samples of patients with tumors >4 cm may clarify the relationship between tumor size, mETE, and DSS in future studies.
The role of ETE in DTC has been investigated previously. Comparisons between gross and minimal ETE have been reported, showing worse OS, DSS, and DFS in tumors demonstrating gross ETE (7,10,11,14 –16). The prognostic significance of mETE, however, is more controversial (7 –11,17). Moon et al. (18) demonstrated no significantly increased risk of recurrence in patients with small conventional PTC. Shin et al. (19) similarly found no significant difference in recurrence-free survival in patients with mETE. On the other hand, Yin et al. completed a meta-analysis demonstrating that mETE confers a higher probability of recurrence (9). However, patient populations in the studies were heterogeneous, and size was unable to be taken into consideration within this meta-analysis. The relationship between size and presence of mETE was explored by Kramer et al. (20), who demonstrated that tumor size was an independent predictor of DFS in patients with mETE. Chereau et al. (21) found that patients with papillary thyroid microcarcinomas <10 mm with mETE had better DFS compared to larger tumors with mETE. Santos et al. explored variability in patients with pathological T3 classified tumors. Though mETE and size were both predictors of treatment response, no comparison was made for disease outcome (22). The current study suggests that mETE does not alter disease outcome when adjusted for tumor size. The questionable prognostic importance of mETE is reflected in the changes to the T3 classification definition in the eighth edition the AJCC staging system. In this new edition, the threshold for upstaging patients to T3 classification or older patients to stage III disease is gross extrathyroidal extension involving the strap muscles (but not solely the perithyroidal soft tissues), which is supported by the findings in this current study (23). Further investigation of the effect of size on the new definition of mETE is needed.
Pathologic diagnosis of mETE can be difficult. Mete et al. (4) describe the thyroid's lack of a true capsule and presence of adipose within the gland as examples of reasons why diagnosis of mETE can be variable. Even in a high-volume thyroid center, the diagnosis of mETE has poor inter-rater reliability between dedicated head and neck pathologists (5). In this current cohort, 36% of tumors were upstaged based on the presence of mETE. However, the current 2015 ATA guidelines consider the presence of mETE, regardless of the size of the tumor, to be a determining factor of intermediate risk disease (1).
The 2015 ATA guidelines emphasize the importance of risk stratification in determining the extent of adjuvant therapy (1). Currently, the role of RAI in intermediate-risk thyroid cancer continues to be controversial. The purpose of RAI treatment in intermediate-risk DTC is primarily to decrease the risk of recurrent disease. Ruel et al. (24) utilized the National Cancer Database to investigate intermediate-risk papillary thyroid cancer in 21,870 patients, of whom 71% received adjuvant RAI. Due to limitations with the database, OS was used as the primary outcome measure, which was statistically better (p = 0.001) with delivery of RAI. However, the presence of mETE was not specifically investigated. Chow et al. (25) described a cohort of 352 patients with evidence of mETE and found differences in local control with addition of RAI treatment, but this was based on univariate analysis only. On the other hand, overall disease recurrence was not found to be different in patients receiving RAI with mETE in a systematic review by Lamartina et al. (26). The current study found that tumor size may be a more important consideration than presence of mETE in disease recurrence, which may account for the variability in the findings of previous studies. Additionally, mETE was not a significant predictor of DFS, LRS, or DMF on multivariate analysis, suggesting the need to investigate the role of RAI further in patients with mETE regardless of size. As suggested by the 2015 ATA guidelines, de-escalation of adjuvant treatment according to tumor size rather than the presence of mETE may be warranted and requires further exploration (1).
This study is limited by its retrospective nature. Treatments were chosen based on practitioner assessment of a variety of disease factors that may not be adequately captured by the analysis, though many of these factors have been controlled using multivariate analysis. Therefore, though this analysis brings important questions about treatment to the forefront, treatment recommendations cannot be made based on these data alone. Moreover, presence of mETE was considered a binary variable, and extent of mETE was not considered, which may be an important differentiator for prognosis in these patients.
To the authors' knowledge, this is the largest single-institution study of the effect of mETE and size on DTC outcomes. Previously published studies using national databases have investigated the prognostic importance of the presence of mETE but did not specifically consider size. A previous study investigating the effect of size in patients with mETE discussed short-term treatment response but lacked longer-term disease outcomes, as reported in this current study (22). Despite the aforementioned limitations, this study raises important doubt as to whether patients should undergo differing adjuvant treatment based on the presence or absence of mETE alone. Future studies investigating the efficacy of RAI in this subgroup would be helpful in determining its use in T1–T3 DTC.
Conclusions
When adjusted for other covariates, tumor size continued to be an independent predictor for tumor recurrence, while mETE had no significant effect for a given tumor size.
Footnotes
Author Disclosure Statement
No competing financial interests exist.