
Abstract
Objective:
This study investigated the association between hypothyroidism and mortality in both treated and untreated hypothyroid patients, and the consequences of over- and under-treatment with respect to mortality.
Patients and Methods:
This was a register-based cohort study of 235,168 individuals who had at least one serum thyrotropin (TSH) during 1995–2011 (median follow-up 7.2 years). Hypothyroidism was defined as at least two measurements of TSH >4.0 mIU/L within a half year spaced by at least 14 days, or one measurement of TSH >4.0 mIU/L and two filled prescriptions of levothyroxine the following year. All-cause mortality rates were calculated using multivariable Cox regression analysis adjusted for age, sex, and comorbidities using the Charlson Comorbidity Index.
Results:
Mortality was increased in untreated hypothyroid individuals (n = 673; hazard ratio [HR] = 1.46 [confidence interval (CI) 1.26–1.69]; p < 0.001) compared to euthyroid controls. Results remained significant even when subdividing according to mild (TSH >4.0 mIU/L and ≤10 mIU/L; p < 0.001) and marked hypothyroidism (TSH >10 mIU/L; p = 0.002). Mortality was increased in both treated and untreated hypothyroid individuals for each six months a patient had increased TSH (HR = 1.05 [CI 1.02–1.07], p < 0.0001, and HR = 1.05 [CI 1.02–1.07], p = 0.0009, respectively). In patients who received levothyroxine, the HR for mortality increased by a factor 1.18 ([CI 1.15–1.21]; p < 0.0001) for each six months a patient exhibited decreased TSH. This finding was essentially unchanged after stratification by disease severity (mild or marked hypothyroidism) and age (older and younger than 65 years).
Conclusions:
Mortality was increased in untreated but not in treated hypothyroid individuals, independently of age and severity of hypothyroidism. Duration of decreased TSH in treated individuals had a greater impact on mortality than did duration of elevated TSH. These results stress the need for close monitoring of treatment in individuals receiving thyroid hormone replacement therapy.
Introduction
H
This study aimed to investigate all-cause mortality in treated as well as untreated biochemically documented hypothyroid individuals. Furthermore, it investigated the consequence of over- and under-treatment of hypothyroidism by analyzing the relationship between duration of decreased and elevated TSH, respectively, and mortality in hypothyroid individuals receiving treatment.
Materials and Methods
Study design and population
In order to determine the association between treated and untreated hypothyroidism and mortality, a register-based cohort study was conducted. The cohort was established through the Odense Patient data Explorative Network (OPEN). OPEN contains the results of all blood samples collected from hospitals and general practices on the island of Funen between January 1, 1995, and January 1, 2011. Through a unique personal identifier, the data were linked to the Danish National Patient Register (DNPR), which contains diagnoses from hospital admissions based on the International Classification of Diseases (ICD)-8 and ICD-10 since January 1, 1977, and outpatient visits since January 1, 1995 (20), the Danish National Prescription Registry (DNPrR), which contains data on all prescriptions filled since 1995 (21), and the Danish Register of Causes of Death, which contains data on mortality and causes of death (22). As described in Figure 1, 275,467 individuals—who in the period January 1, 1995, to January 1, 2011, had at least one thyroid function test performed—were initially identified. To investigate incident cases, patients who had a thyroid function test before 1996 were excluded (n = 5644). Furthermore, individuals known to use thyroid medication, including thyroid hormone, or who had undergone thyroid surgery or radioactive iodine treatment prior to the first TSH determination were excluded (n = 8819). Persons younger than 18 years of age (n = 20,260), with previous pituitary disease (n = 753), and those who emigrated or were lost to follow-up (n = 223) were excluded, as were hyperthyroid patients (n = 2793). Thyroid function was defined based on the initial TSH determinations. Hence, hypothyroidism was defined by at least two measurements of elevated TSH within a period of six months, at least 14 days apart. In order to include patients in whom intervention was started without repeating TSH measurements, individuals with an increased initial TSH level and subsequently at least two filled prescriptions of thyroid hormone within the following year were also considered to be hypothyroid. Because of the minimum two weeks between TSH measurements, follow-up started 14 days after the initial TSH determination for identical allocation of risk time. Accordingly, as discussed below, individuals who died during this period of time were excluded due to negative time (n = 1807). This left 2908 hypothyroid cases, and 232,260 euthyroid controls qualified for analysis. Participants were followed until death or end of study (November 30, 2012). Since blood measurements were repeated, controls could become hypo- and/or hyperthyroid during follow-up. If so, they were censored at the time of development of thyroid dysfunction, as they would no longer contribute unexposed risk time. As the databases are event based and capture contacts to general practices and hospitals, as well as filled prescriptions, there were no identifiably missing data.
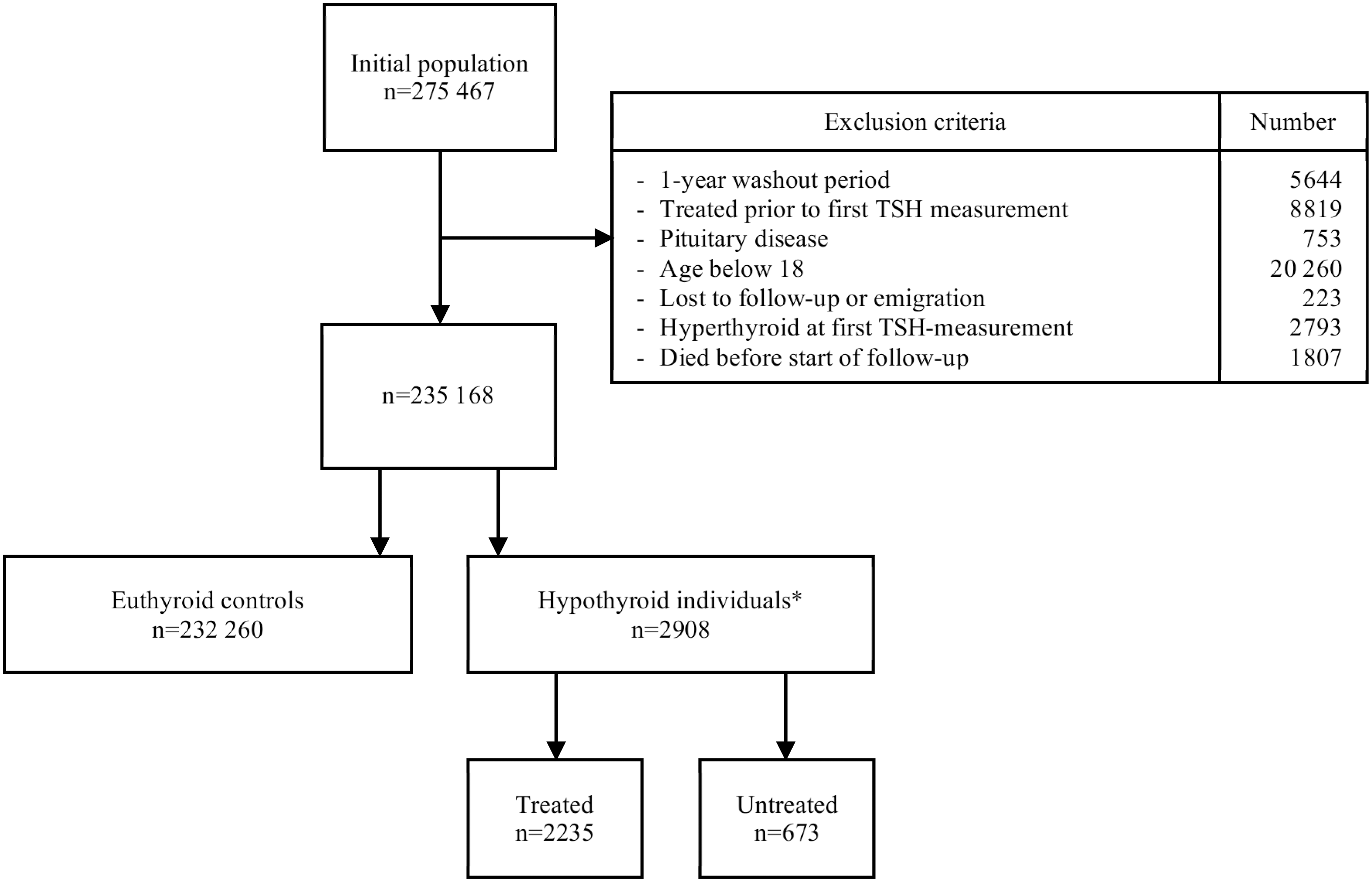
Flow of individuals in the study with at least one serum thyrotropin (TSH) measurement. *Two measurements of decreased TSH: n = 2414; one measurement of decreased TSH, two subsequent prescriptions of LT4: n = 494.
Patient involvement
There was no patient involvement in the design or analysis of this study. All findings are disseminated through patient organizations (The Danish Thyroid Patient Society, Denmark).
Thyroid function
Hypothyroidism was defined as above, and further arbitrarily subdivided into mild (TSH >4.0 mIU/L and ≤10 mIU/L) and marked hypothyroidism (TSH >10 mIU/L). Euthyroidism was defined as TSH between 0.3 and 4.0 mIU/L, and hyperthyroidism as TSH <0.3 mIU/L. All TSH determinations were performed in the same laboratory. The methods have been described in detail elsewhere (23). Briefly, until 2006, TSH analyses were performed using the AutoDELFIA equipment (Wallac, Turku, Finland). The limit of detection (LOD) was 0.005 mIU/L, while within-run imprecision had a coefficient of variation (CV) of 2.7% at 0.89 mIU/L and 1.3% at 17.6 mIU/L (24). From 2006, TSH was determined with a solid-phase, two-site chemiluminescent immunometric assay using Immulite 2000 equipment (Siemens, Erlangen, Germany). LOD was 0.004 mIU/L, and within-run CV was 5.3% at 0.32 mIU/L and 3.9% at 3.3 mIU/L. Method comparison was performed in 120 patient samples using Spearman's rank-order correlation, showing a regression coefficient of 0.991. An external quality control program secured comparability (Ringversuche, RfB, Bonn, Germany).
Treatment
Treatment was defined as having filled at least one prescription of thyroid hormone during follow-up, or at least two filled prescriptions of thyroid hormone within the first year of an increased initial TSH.
Outcome measures
All-cause mortality as registered in the Danish Register of Causes of Death.
Morbidity
The Charlson Comorbidity Index (CCI) (25) was used to determine comorbidity at initial TSH measurement. Diagnoses prior to the index date were identified from ICD-8 and ICD-10 codes in the DNPR. Thus, the CCI in this study covers the period from January 1, 1977, until the date of the first TSH determination of the participants.
Ethical considerations
The data used in the study were anonymized so that the identity of all patients remained unknown to the investigators, and the project was approved by the Danish Data Protection Agency. OPEN is an approved research institution permitted to access data hosted by Statistics Denmark (Project 704047).
Statistical analysis
Baseline demographics of the study groups were analyzed using parametric and nonparametric statistical methods as applicable. Cox regression was used to calculate hazard ratios (HR) for mortality, with adjustment for age, sex, and comorbidities, all factors that influence mortality. The proportional hazards assumption was assessed by inspection of Schoenfeld residuals versus time. No significant deviations from the proportional hazards assumption were present. Post hoc comparisons of distribution of causes of death between groups were performed using the Kolmogorov–Smirnov test for equality of distributions.
As thyroid status may vary over time, a dynamic model using six-month periods of elevated TSH, as well as decreased TSH in the treated population, was applied in the Cox regression to analyze thyroid status as a dichotomous time-varying covariate. It also allowed the effect of possible over- and under-treatment to be analyzed. Any six-month period in which no TSH measurements had been performed were considered periods of normal TSH.
Sensitivity analyses were performed to control for immortal time bias (26) with regard to treatment. Further analyses were performed in order to adjust for the possible influence of postpartum thyroiditis and pregnancy on TSH levels by excluding patients registered in the DNPR with a contact regarding pregnancy or a diagnosis of postpartum thyroiditis in a nine-month period before or after the initial TSH. Stratification into age groups younger than and older than 65 years was also performed. Analyses of cases defined by 6 or 12 weeks between initial TSH measurements were performed in order to limit risk of overlooking transient hypothyroidism. Finally, comparison of mortality between the treated individuals with regard to case definition was performed.
Significant differences between the study groups were defined by p-values <5% using two-tailed tests.
Statistical analyses were performed in Stata v14.1 (Stata Corp. Inc., College Station, TX) and SAS v9.4 (SAS Institute, Inc., Cary, NC) through virtual private network access to Statistics Denmark.
Results
A total of 2908 individuals were identified as hypothyroid. Thus, 2414 individuals had two measurements of elevated TSH, while 494 had an initial TSH measurement of elevated TSH and filled at least two prescriptions of thyroid hormone within one year. Of these 2908 hypothyroid individuals, 2235 (76.9%) initiated treatment during follow-up, while 673 (23.1%) remained untreated. Subdividing according to level of TSH, 1852 individuals were identified with mild TSH elevation (TSH >4.0 mIU/L and ≤10 mIU/L; 1224 treated and 628 untreated), and 1056 with marked TSH elevation (TSH >10 mIU/L; 1011 treated and 45 untreated; Table 1). The 235,168 individuals of the study cohort were followed for a total of 1,737,892 years (median follow-up 7.2 years; range 0–16.9 years). In this period, the study participants received a mean of 3.7 measurements of TSH (SD = 4.5), corresponding to a mean of 1.4 measurements of TSH per year of follow-up (SD = 17.3). Treated patients filled a mean of 35.4 prescriptions of LT4 during follow-up (SD = 28.1), corresponding to a mean of 4.3 prescriptions of LT4 per year of follow-up (SD = 2.7).
Significantly different compared to controls.
Significantly different from treated within the same group.
CCI, Charlson Comorbidity Index.
Baseline characteristics of the study population are listed in Table 1. Euthyroid controls were significantly younger than the hypothyroid group, and comprised significantly fewer females. Median follow-up in the control group was significantly shorter than in the treated hypothyroid groups, while it was significantly longer than in the untreated hypothyroid groups. Comorbidity was significantly increased in the untreated individuals in the entire hypothyroid group compared to controls, but not in the treated individuals. This was also the case in the mildly hypothyroid, but not in the markedly hypothyroid group.
Median TSH concentration at first determination was significantly lower in the untreated than in the treated group.
Mortality in the entire hypothyroid group and association with treatment
A total of 386/2235 (17.3%; incidence rate 20.7/1000 person years [confidence interval (CI) 18.8–22.9]) treated patients died during a median 8.6 years (range 0.1–16.9 years) of follow-up. This was significantly fewer than in the untreated group, where 175/673 (26.0%; incidence rate 42.2/1000 person years [CI 36.4–48.9]) died during a median follow-up of 5.5 years (range 0–15.8 years; p < 0.001). The HR for all-cause mortality was 0.97 ([CI 0.88–1.08]; p = 0.61) in the treated versus control subjects, and 1.98 ([CI 1.71–2.30]; p < 0.001) in the untreated versus control subjects. After adjusting for age, sex, and CCI, the HR in the treated individuals versus controls was 0.83 ([CI 0.75–0.92]; p < 0.001), while the HR in the untreated group versus controls was 1.46 ([CI 1.26–1.69]; p < 0.001; Table 2). Stratification into age groups older than and younger than 65 years essentially yielded the same results as the main analysis. In the group ≥65 years of age, the HR was 0.84 ([CI 0.75–0.94; p = 0.002) in the treated individuals versus controls, and 1.42 ([CI 1.20–1.68]; p < 0.001) in the untreated individuals versus controls. In the group <65 years of age, the HR was 0.80 ([CI 0.64–1.00]; p = 0.052) in those treated versus controls, while it was 1.66 ([CI 1.21–2.26]; p = 0.001) in the untreated individuals versus controls.
Data shown are HR with confidence intervals.
Adjusted for age, sex and Charlson Comorbidity Index.
p < 0.001; ** p = 0.002.
HR, hazard ratio.
Testing for equality of distributions, no differences were found in distribution of causes of death between any of the groups. Specific causes of death were investigated in the untreated hypothyroid group, but the small number of deaths in this group by for example cardiovascular disease (n = 28) did not allow for any meaningful statistical evaluation of causes of death.
Mortality in the mildly hypothyroid and association with treatment
Mortality was increased relative to that of controls in untreated mild hypothyroidism (HR = 1.93 [CI 1.65–2.25]; p < 0.001), but not in those who were treated. When controlling for age, sex, and comorbidities, mortality remained significantly increased in the untreated versus controls (HR = 1.41 [CI 1.21–1.65]; p < 0.001], but was significantly reduced in those treated versus controls (HR = 0.76 [CI 0.66–0.88]; p < 0.001).
Mortality in the markedly hypothyroid and association with treatment
The HR for mortality in treated patients versus control subjects was 1.10 ([CI 0.96–1.27]; p = 0.2) compared to 2.78 ([CI 1.68–4.62]; p < 0.001) in those untreated versus controls. In the adjusted analysis, the association between elevated TSH and all-cause mortality remained insignificant in the treated individuals, while mortality in the untreated individuals was greater than in controls (HR = 2.27 [CI 1.37–3.76]; p = 0.002).
Dose–response analyses
When periods of elevated TSH (a proxy for under-treatment) were employed as a time-dependent variable, an increased mortality was found per every six months of elevated TSH in both treated (HR = 1.05 [CI 1.02–1.07]; p < 0.0001) and untreated hypothyroid individuals (HR = 1.05 [CI 1.02–1.08]; p = 0.0009). In the group with an initially mild increase in TSH, HR for mortality per six months of elevated TSH was 1.07 ([CI 1.04–1.10]; p < 0.0001) in the treated and 1.06 ([CI 1.03–1.10]; p = 0.0001) in the untreated individuals. In the group with an initially marked increase of TSH, HR for mortality per six months of elevated TSH was significantly increased in those treated (HR = 1.05 [CI 1.02–1.08]; p = 0.0005), as well as in the untreated individuals (HR = 1.07 [CI 1.03–1.10]; p < 0.0001).
Analyzing periods of decreased TSH (TSH <0.3 mIU/L), as a measure of over-treatment, it was found that mortality was significantly increased per six months of decreased TSH in the treated groups, irrespective of severity: HR = 1.18 ([CI 1.15–1.21]; p < 0.0001) in the entire hypothyroid group. The HR was 1.19 ([CI 1.16–1.22]; p < 0.0001) in the group with initially mildly elevated TSH, and 1.18 ([CI 1.15–1.21]; p < 0.0001) in the group with initially markedly elevated TSH (Table 3).
Data shown are HR with confidence intervals, adjusted for age, sex, and CCI.
p < 0.0001.
Stratifying by age, mortality per six months of decreased TSH was higher in those <65 years of age than in the group >65 years of age compared to controls: HR = 1.26 ([CI 1.19–1.34]; p < 0.0001) and HR = 1.16 ([CI 1.13–1.19]; p < 0.0001), respectively.
Sensitivity analyses
In order to evaluate the validity of the definition of hypothyroidism, the survival analyses were performed with cases defined with the two initial TSH measurements six weeks apart, and also 12 weeks apart, starting follow-up 6 and 12 weeks after the initial TSH, respectively. This did not influence the overall results (data not shown).
Excluding patients with pregnancy or postpartum thyroiditis did not change the results of the analyses (data not shown).
When allocation to a specific case group is determined by an event that occurs during follow-up, in this case treatment, individuals are essentially immortal from start of follow-up until initiation of treatment, thus causing an immortal time bias. A total of 412 hypothyroid individuals (14.2%) started treatment a year or more after the start of follow-up, which may have caused an overestimation of survival in the treated group. In order to control for this bias, sensitivity analyses were performed starting follow-up after one, two, and three years, excluding patients who died before these landmarks and anyone who started treatment afterwards. When compared to the original analysis (as shown in Table 2), the HR for all-cause mortality essentially remained the same in the untreated hypothyroid group, while the survival in the treated group was now the same as in the controls (Table 4). There was no difference in mortality between the treated hypothyroid individuals defined by two measurements of decreased TSH and the treated hypothyroid individuals defined by one measurement of low TSH and two filled prescriptions.
Adjusted for age, sex, and CCI.
p < 0.001; ** p = 0.02.
Discussion
Principal findings
In this long-term follow-up study of a cohort of biochemically documented treated and untreated hypothyroid individuals, the effect of treatment with thyroid hormone was evaluated. The study emphasizes the effect of duration of under- and over-treatment on all-cause mortality. To the authors' knowledge, this is the first study to do so. Strong evidence is provided for excess mortality in hypothyroid patients who do not receive treatment, while treated hypothyroid patients have mortality similar to that of the background population. When taking into account periods of decreased TSH as well as periods of elevated TSH in treated hypothyroid individuals, the risk of mortality is highest per six months of decreased TSH, irrespective of age and disease severity, graded by the magnitude of TSH elevation. While not directly implying causality, this suggests that the duration of over-treatment of hypothyroidism may have a greater impact on mortality than the duration of under-treatment of hypothyroidism.
Comparison with previous studies
Numerous studies and meta-analyses have investigated the relationship between hypothyroidism and mortality (3,8,10 –13,27 –37), but disagreement persists. A potentially important reason for this poor reproducibility is the considerable heterogeneity between the studies with regard to case definition, study design, follow-up length, and treatment. For example, some studies rely on only one TSH measurement for case definition (8,11,12,28 –30,32,33,35,37). This carries a risk of phenotype misclassification, since spontaneous normalization of an initially elevated TSH may occur in >50% of individuals given a repeat measurement (38). The risk of misclassification is minimized by the present approach of using two TSH determinations separated in time. Many studies are hampered by inadequate control for comorbidities (10,11,27,33). However, it is well accepted that the burden of comorbidity influences mortality (13) and should therefore be taken into consideration. This study used the CCI to control for this effect, thereby allowing the investigation of a more direct association between hypothyroidism per se and mortality. In addition, most earlier studies have not differentiated between treated and untreated individuals. Also, when investigating treated individuals, these studies disagree on whether mortality is increased (10,27 –29,35) and suffer from the limitations highlighted previously.
Strengths and limitations
A strength of this study is the fact that participants were diagnosed and treated in a real-world clinical setting, suggesting robustness of the results and that they may be applicable to other populations. Unique to the current study is the assessment of the association between duration of decreased TSH and elevated TSH (reflecting over- and under-treatment, respectively) and mortality in hypothyroid individuals who receive thyroid hormone replacement therapy. In light of recent studies showing a high prevalence of over-treatment in patients receiving thyroid hormone replacement therapy, this may constitute the most important message of this study (16,17). Thus, thyrotoxicosis caused by excess treatment with thyroid hormones accounted for approximately half of both prevalence and incidence measures of decreased TSH in a cohort of community-residing older individuals (17). In support, Somwaru et al. found that 41% of patients >65 years of age and receiving thyroid hormone had decreased TSH (16). Combined, these data provide strong arguments for more meticulous monitoring of thyroid hormone therapy in hypothyroid patients. Indeed, considering that recent studies showed no effect of treatment of mild hypothyroidism on quality of life (15) or cardiac morbidity (35), and may suggest a prolonged life-span in the elderly with elevated TSH (12,31), the decision to initiate treatment in hypothyroid individuals is not straightforward. In other words, it is paramount that hypo- and hyperthyroidism is avoided through proper dosage of medication and titration according to TSH measurements.
The current study does have limitations. Data on smoking and alcohol consumption—two factors that influence both thyroid disease and mortality (39,40)—were not available. However, adjusting for chronic pulmonary disease, cancer, and liver disease using the CCI partly alleviates this limitation. Any 6-month period with no TSH measurement was classified as a period of euthyroidism. This operational definition implies that a study participant may have had periods of unmonitored thyroid dysfunction that were considered euthyroid time intervals in the analyses. However, if of any influence, it would lead to an underestimation of the effect of thyroid disease and over-treatment, rather than inflation of the risk estimates.
It is important to emphasize that the control population is not a random population sample, and thus does not necessarily represent a healthy background population with respect to mortality. The initial TSH determination likely was performed due to suspicion of thyroid disease or in relation to a general test. Even so, it is surprising that mortality should be lower in patients with hypothyroidism who receive replacement therapy than in those who are not hypothyroid at all. Information on the reasons for initiating or withholding treatment is lacking, and the possibility cannot be dismissed that the better survival in the treated group is due to more medical attention than the untreated group. Moreover, the finding of lower mortality in treated hypothyroidism than in spontaneously euthyroid individuals was not robust to changes in the starting time of the Cox regression, as shown in Table 4, suggesting that the criterion used to classify patients as having initiated treatment is responsible for a large proportion of the observed difference. However, as the treated hypothyroid individuals have more severe hypothyroidism than those untreated, as evident from the baseline TSH measurements, the lack of excess mortality in the treated individuals is consistent with a benefit from treatment, even in patients with mild TSH elevation, but not to a survival that exceeds that of euthyroid subjects.
Due to lack of power, mortality was not investigated in patients on LT4-liothyronine combination therapy separately. The literature gives us no reason to believe that the consequences of decreased TSH with regard to mortality depend on whether it is caused by monotherapy with LT4 or the combination of LT4 and liothyronine. Long-term data regarding comorbidities and mortality in individuals receiving combination therapy are unavailable. In view of the growing patient demand (41) and the fact that many such patients are over-treated, this supports the unambiguous relevance of the data and reinforces the need for further study.
Conclusion
In conclusion, mortality was increased in untreated but not in treated hypothyroid individuals, independently of age and severity of hypothyroidism. The duration of decreased TSH in treated hypothyroid individuals had a greater impact on mortality than did duration of elevated TSH, stressing the need for close monitoring of treatment in individuals receiving thyroid hormone replacement therapy.
Footnotes
Acknowledgments
Dr. Mads Nybo, Department of Clinical Biochemistry, Odense University Hospital, is acknowledged for his role in the initial data collection. This article was presented orally in part at the annual meeting of the European Thyroid Association in Belgrade, Serbia, September 9–12, 2017.
Author Disclosure Statement
All authors have completed the ICMJE uniform disclosure form at