
Abstract
Background:
The outcomes of patients with thyroid cancer proven by histology in patients in whom cytology was Thy 3 (indeterminate; Thy 3 patients in this study) based on the Italian consensus classification compared with those in whom cytology was Thy 4 (suspicious for malignancy) or Thy 5 (indicative for malignancy) (Thy 4–5 patients here) remains unclear.
Objective:
To analyze the outcome of 371 Thy 3 patients versus 269 Thy 4–5 patients homogeneously treated with total thyroidectomy and 131I activity.
Results:
T1 stage was observed in 46.0% of Thy 3 and in 38.8% of Thy 4–5 patients (p = 0.02), N0 in 95.9% of Thy 3 and in 75.5% of Thy 4–5 patients (p < 0.0001). 35/261 (9.6%) Thy 3 and 85/269 (31.5%) Thy 4–5 patients required >30 mCi of 131I (p < 0.0001). 359/371 (96.8%) Thy 3 and 232/269 (86.2%) Thy 4–5 patients were free of disease at the end of follow-up (p < 0.001). The time required to obtain 50% of patients in remission was 2 years in Thy 3 and 4 years in Thy 4–5 patients (p < 0.001). The most common histological type was the follicular variant of papillary thyroid carcinoma (FV-PTC) in Thy 3 patients (239/371, 64.4%) and the classic variant in Thy 4–5 patients (185/269; 68.8%). The FV-PTC had better prognostic features compared with the other PTC variants: T1 stage was observed in 133/277 (48.0%) FV-PTC patients and in 146/363 (40.0%) patients with the other variants (p < 0.001), N0 was present in 265/277 (96.0%) FV-PTC and in 290/363 (79.8%) patients with the other variants (p < 0.001). Overall, 267/277 FV-PTC patients (96.4%) and 324/363 patients (89.0%) with the other variants were free of disease (p < 0.0008) at the end of follow-up, and the time required to obtain 50% of patients in remission was 2 years in FV-PTC and 4.0 years in the other variants (p < 0.001).
Conclusion:
Patients with Thy 3 cytology have better outcomes of thyroid cancer compared with patients with Thy 4 or Thy 5 cytology, and indeterminate cytology is commonly associated with the less aggressive FV-PTC.
Introduction
F
Papillary thyroid carcinoma (PTC) is the most common endocrine cancer (85–90% of all thyroid cancers) and has a rising incidence in the last decades (5 –9). This histological type has several variants, the most common being the classic and the follicular variant of papillary thyroid cancer (CV-PTC and FV-PTC) (10–11). On histology, the classic variant of PTC is characterized by papillary architecture and peculiar nuclear features with nuclear enlargement, crowding, clearing and irregular nuclear borders, resulting in the formation of nuclear grooves and pseudo-inclusions (12 –14). The follicular variant, described initially by Lindsay (15) and later characterized by Chem and Rosai (16), has now been extensively recognized as a variant characterized by nuclear features of classical PTC associated with follicular cell growth patterns. It has been recently reported that the prognosis of PTC correlates with histological type (17 –19), with the tall cell variant having the worst and the follicular variant the best prognosis.
It is well established that some patients with indeterminate cytology will have a thyroid carcinoma on histology. However, the clinical outcome of patients with a final histology of thyroid carcinoma in whom cytology was indeterminate compared with those in whom cytology was suspicious or indicative of carcinoma remains unclear. This information is relevant for establishing an appropriate management strategy.
In this study we observed that patients with a final histological diagnosis of thyroid cancer and an indeterminate cytology have less aggressive tumors and better outcomes compared with patients with cytological findings suspicious or indicative of carcinoma.
Materials and Methods
Patients
In a previous study (5), among 5546 patients with Thy 3 cytology who presented at our institution during the period January 2000 to December 2010, we evaluated 1520 consecutive patients who had a complete workup in our institution including: (a) fine needle aspiration cytology, (b) thyroid surgery, (c) pathological examination, and (d) follow-up. Of these 1520 patients, 371 had a histology of cancer (Thy 3 patients).
Among the entire group of 2098 patients with Thy 4 or Thy 5 cytology and cancer on histology, observed during the same period and meeting the identical inclusion criteria, we randomly selected 269 patients matched for sex, age, and length of follow-up (Thy 4–5 patients). All patients gave their informed consent to participate to the study.
Thyroid function tests
Serum thyrotropin (TSH) was measured by a sensitive immunoradiometric assay (Delphia, Pharmacia; reference values 0.4–3.4 μU/mL). Serum thyroglobulin was measured by Immulite 2000 (Diagnostic Products Corp.; functional sensitivity: 0.5 ng/mL) or by Access Immunoassay Systems, 2006 (Beckman Counter, Inc,; functional sensitivity: 0.1 ng/mL). Autoantibodies to thyroglobulin (TgAb) were measured by Immuno Enzymometric assay (AIA-Pack TgAb, Tosoh; positive values >30 IU/mL). Serum free thyroxine (FT4) was measured by RIA (FT4 Liso-Phase, reference values 7–17 pg/mL, Technogenetics, s.r.l.).
Thyroid ultrasound
Conventional ultrasound (US) was performed using a real-time instrument (Esaote SPA, My Lab 70 machine with 8–13 MHz linear transducer). During the follow-up, remnants or recurrent disease in the thyroid bed and suspicious lymph nodes in neck stations were evaluated by thyroid US.
Fine needle aspiration cytology and histology
FNA was performed under US guidance using a 23-gauge needle attached to a 10 mL syringe. The material was air dried, stained with Papanicolaou and Giemsa, and interpreted by two experienced cytopathologists (R.R., G.S.). The adequacy of aspirates was defined according to the guidelines of the Papanicolaou Society (20). Results of cytology were classified according to the Italian Consensus classification (1), in which the Thy 3 category, subdivided into two subclasses (Thy 3A and Thy 3B), roughly corresponds to the Thy III and Thy IV classes of the Bethesda classification system (3). The histological diagnosis was made by two expert pathologists (F.B., A.P.) according to the 2004 World Health Organization guidelines (21).
Treatment and follow-up
Out of the 371 Thy 3 patients, 303 underwent total thyroidectomy at the first operation, while 68 patients with a single nodule underwent lobectomy and then a completion thyroidectomy after the diagnosis of thyroid cancer on histology. All 269 Thy 4–5 patients were treated with total thyroidectomy at the first operation and subsequent 131I remnant ablation.
Patients were evaluated at 3, 6, and 12 months after surgery, and every 12 months thereafter. The follow-up was 1–12 years (mean ± SD 3.1 ± 1.2 years). At each evaluation, serum Tg, TgAb, TSH, and FT4 were measured. Neck US was performed to assess the presence of remnant/relapse and/or lymph node metastases. In patients with suspicious lymph nodes or recurrence in the thyroid bed, FNA with measurement of Tg in the washout liquid from the needle was performed. When necessary, the workup included radioiodine scanning after stimulation with recombinant TSH, computed tomography scan, magnetic resonance imaging, or 2-deoxy-2-fluorine-18-fluoro-D-glucose positron emission tomography/computed tomography.
Statistical analysis
Proportions and frequencies calculated in different groups of patients were compared using chi-squared test and Fisher's exact test as appropriate. The Kolmogorov-Smirnov test was employed to test the normality of data distribution of continuous variables. Student's t-test and Mann–Whitney U test were used to detect differences between groups for normal and skewed variables, respectively. Disease-free probability was calculated by the Kaplan–Meier analysis using the Aalen-Johansen method of cumulative remission rate in patients, and differences between groups of patients were tested by the log-rank test (23). Statistical analyses were performed using SPSS (SPSS Inc.).
Results
Histology
Among the 371 Thy 3 patients, 308 had papillary thyroid carcinomas, 55 follicular carcinomas (49 minimally invasive), and 8 poorly differentiated thyroid carcinomas. Out of the 308 papillary thyroid carcinomas, 47 were classic variant, 239 follicular variant, 6 oxyphilic variant, 10 tall cell variant, and 6 solid variant with trabecular aspects (Fig. 1). All the 269 Thy 4–5 patients had papillary thyroid carcinomas: 185 were classic variant, 38 follicular variant, 1 oxyphilic variant, 42 tall cell variant, and 3 solid variant with trabecular aspects. Therefore, the great majority (239/371; 64.4%) of Thy 3 patients had the follicular variant while 185/269 (68.8%) of Thy 4–5 patients had the classic variant (Fig. 1). Two hundred and twenty five out of 277 follicular variant specimens were available for revision. Out of these, 105 were encapsulated and among them 17 were reclassified as noninvasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP) (15 in Thy 3 and 2 in Thy 4–5).
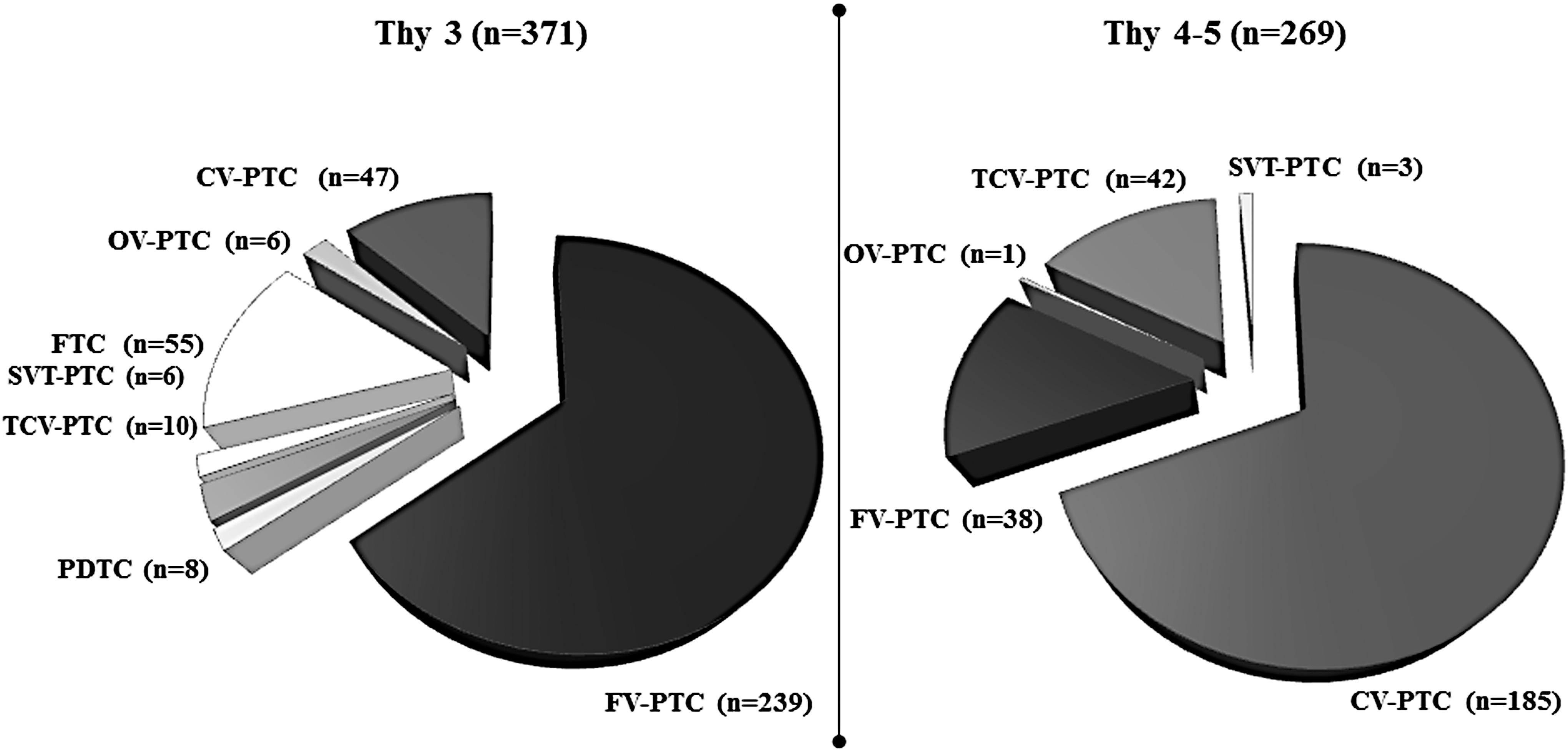
Distribution of histotype and variants of thyroid carcinoma in 371 Thy 3 and 269 Thy 4–5 patients. CV-PTC, classic variant papillary thyroid carcinoma; FC, follicular carcinoma; FV-PTC, follicular variant PTC; OV-PTC, oxyphylic variant PTC; PDC, poorly differentiated carcinoma; SVT-PTC, solid variant with trabecular PTC; TCV-PTC, tall cell variant PTC.
Tumor characteristics in Thy 3 and Thy 4–5 patients
The tumor stage was T1 in 171/371 (46.0%) Thy 3 and in 102/269 (37.8%) Thy 4–5 patients (p = 0.02). 356/371 (95.9%) Thy 3 and 203/269 (75.5%) Thy 4–5 patients had no evidence of lymph node metastasis (N0) (p < 0.0001). A few patients had distant metastases: 3/371 (0.8%) Thy 3 and 5/269 (1.9%) Thy 4–5 patients (p = 0.2). Extrathyroidal extension was found in 32/355 (9.0%) Thy 3 and 95/235 (40.0%) Thy 4–5 patients (p < 0.0001); lymphovascular invasion was found in 24/355 (6.7%) Thy 3 and 10/235 (7.5%) Thy 4–5 patients (p = 0.2) (Table 1). In all patients, tumors were completely resected and surgical resection margins were negative.
Tumor characteristics in follicular variant vs other variants of papillary thyroid carcinomas
The clinical features of the 277 patients with FV-PTC were compared with those of the 363 patients with the other variants of PTC. The tumor stage was T1 in 133/277 (48.0%) patients with FV-PTC and in 146/363 (40.0%) with the other variants (p < 0.001). 265/277 (96.0%) patients with FV-PTC and 290/363 (79.8%) with other variants had no evidence of lymph node metastasis (N0) (p < 0.001). A few patients had distant metastases in both groups: 5/277 (1.8%) of those with the FV-PTC and 8/363 (2.2%) of those with the other variants of PTC (p = 0.7).
A noncapsulated tumor was found in 43/264 (16.2%) FV-PTC and in 287/326 (88.0%) of the other variants (p < 0.0001). Extrathyroidal extension was found in 22/264 (8.3%) FV-PTC and in 104/326 (21.9%) of the other variants (p < 0.0001); lymphovascular invasion was found in 7/264 (2.7%) FV-PTC and in 27/326 (8.2%) of the other variants (p < 0.003) (Table 2).
Clinical outcomes according to cytology in Thy 3 versus Thy 4–5 patients
A lower number of Thy 3 patients (35/261; 9.6%) required a 131I activity >30 mCi, as compared with Thy 4–5 patients (85/269; 31.5%) (p < 0.001). The cumulative activity of 131I was 51 ± 119 (mean ± SD) mCi in Thy 3 patients and 104 ± 53 (m ± SD) mCi in Thy 4–5 patients (p < 0.001) (data not shown). Ten Thy 3 patients did not require 131I remnant ablation or therapy because of their favorable TNM score.
The cumulative remission rate was higher in Thy 3 patients (median 2.0 years; mean + SD: 3.0 + 2.2 yr) versus Thy 4–5 patients (median 4.0 years; mean + SD: 5.2 + 3.1 yr) (p < 0.001) (Fig. 2). At the end of follow-up 359/371 (96.8%) Thy 3 patients and 232/269 (86.2%) Thy 4–5 patients were in remission (p < 0.001) (Fig. 2). Out of 12 Thy 3 patients with persistent disease, 7 had biochemical persistence and 5 structural persistent disease (1 lymph node metastasis, 3 distant and lymph node metastasis, 1 local disease). The mean age of Thy 3 patients was 41 ± 13 years in those with biochemical persistent disease, and 54 + 19.0 years in those with structural disease. Out of the 37 Thy 4–5 patients with persistent disease, 4 had biochemical and 33 structural persistent disease (13 local disease, 10 local disease and distant metastasis, 9 distant metastasis, 1 patient died secondary to local disease with infiltration of esophagus and trachea). The mean age of Thy 4–5 patients was 39 ± 14 years in those with biochemical persistent disease and 47 ± 21 years in those with structural persistent disease. Thy 3 versus Thy 4–5 patients showed a lower prevalence of biochemical persistent disease (7/371 vs. 4/269; p < 0.0001), as well as of structural persistent disease (5/371 vs. 33/269; p < 0.001). In addition, Thy 3 patients showed a lower prevalence of lymph node metastases (15/371, 4.0%) compared with Thy 4–5 patients (66/269; 24.5%) (p < 0.0001), while no difference was observed regarding distant metastases (3/371; 0.8% vs. 5/269, 1.9% p = 0.2).
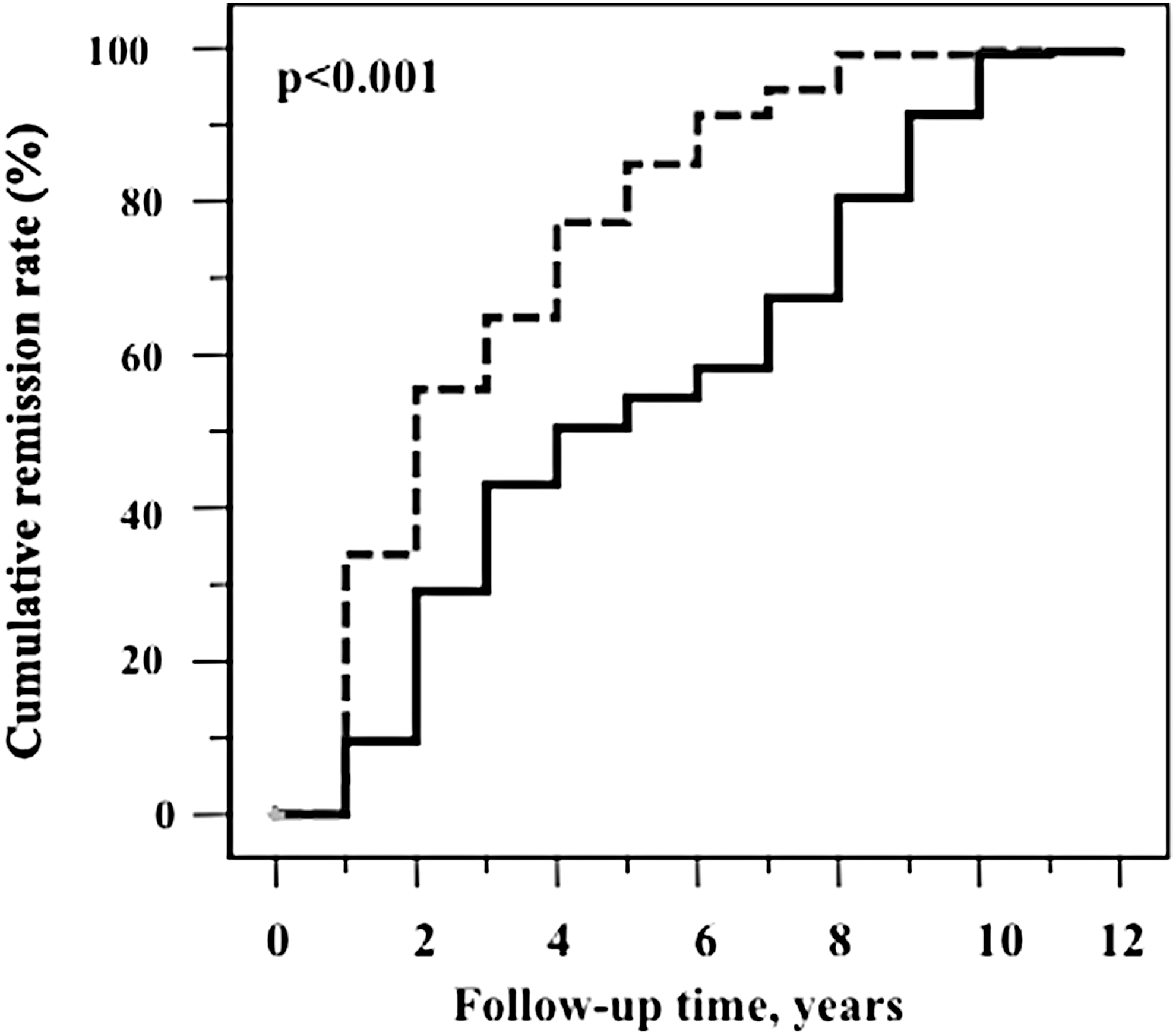
Kaplan–Meier analysis using the Aalen–Johansen method of cumulative remission rate in p Thy 3 patients (n = 371, dashed line) and Thy 4–5 patients (n = 269, solid line). Median: 2 years (Thy 3) vs. 4 years (Thy 4–5); mean ± SD: 3 years ±2.2 (Thy 3) vs. 5.2 ± 3.1 years (Thy 4–5), log-rank test p < 0.001. Patients in remission at the end of follow-up: 359, 96.8% (Thy 3) vs. 232, 86.3% (Thy 4–5).
Clinical outcomes in patients with follicular variant vs other variants of papillary thyroid carcinoma
The cumulative remission rate was higher in FV-PTC (median 2.0 years; mean ± SD: 3.2 ± 2.3 years)s compared with the other variants (median 4.0 years; mean ± SD: 5.2 ± 3.3 years) (p < 0.001). At the end of follow-up, 267/277 (96.4%) patients with the FV-PTC and 324/363 (89.0%) with other variants were in remission (p < 0.001) (Fig. 3). The clinical outcomes of the 55 patients with follicular carcinoma, who were all in the Thy 3 group, was favorable. Indeed, only 1 of them had biochemical persistent disease and 1 structural persistent disease.
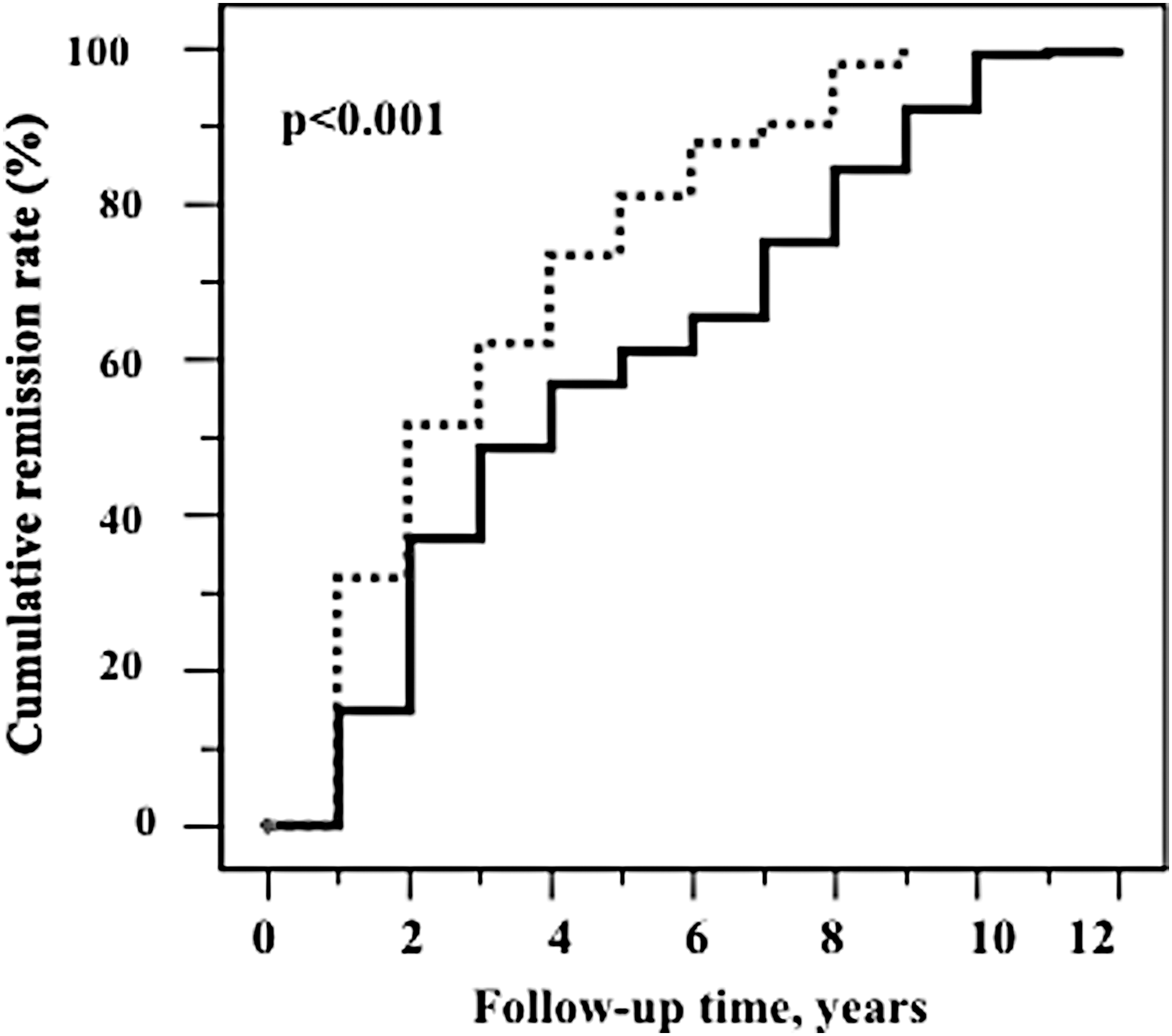
Kaplan–Meier analysis using the Aalen—Johansen method of cumulative remission rate in patients with follicular (n = 277, dashed line) vs. other variants of papillary carcinoma (n = 363, solid line). Median: 2 years (FV-PTC) vs. 4 years (other variants); mean ± SD: 3.2 ± 2.3 years (FV-PTC) vs. 5.2 ± 3.3 years (other variants), log-rank test p < 0.001. Patients in remission at the end of follow-up: 267, 96.4% (FV-PTC) vs. 324, 89.0% (other variants).
Discussion
We had previously reported clinical and histological features of 1520 patients harboring a nodule with Thy 3 cytology, 371 of whom had a histological diagnosis of carcinoma (4). Features associated with malignancy were atypia on cytology, suspicious ultrasound pattern (spot microcalcifications, absent halo sign, hypoechogenicity) and age >40 years. At the end of follow-up, only 12 patients had persistent disease: 5 structural and 7 biochemical. We conclude that patients with Thy 3 cytology, even when carrying a thyroid cancer, have a very favorable prognosis.
It is well established that about 25% of patients with Thy 3 cytology will have a thyroid carcinoma on histology. However, the clinical outcome of thyroid carcinoma in patients in whom the cytology was Thy 3 compared with those in whom the cytology was Thy 45 remains unclear. This information is relevant for the subsequent treatment strategy. We then decided to compare tumor stage, histology and clinical outcomes of the 371 patients with Thy 3 cytology with that of 269 patients with Thy 4–5 cytology and a confirmed histology of thyroid carcinoma. Patients were recruited in the same time period and matched for sex, age, and length of follow-up. The two cohorts were homogeneous regarding treatment. In particular all patients underwent total thyroidectomy and (with a few exceptions) 131I ablation.
Compared with Thy 4–5 patients, Thy 3 patients had smaller tumors and fewer lymph node metastases. Very few patients of both groups had distant metastases, thus a statistical analysis of this feature could not be performed reliably. Liu et al. and VanderLaan et al. reported a higher prevalence of lymph node metastases in patients with malignant cytology compared with nodules with cytologies in the AUS (atypia of undetermined significance/follicular lesion of undetermined significance cytology), follicular neoplasm or suspicious for malignancy groups (24,25). The clinical outcome was more favorable in Thy 3 compared with Thy 4–5 patients, structural and biochemical persistence of disease being less common in the former group at the end of the follow-up. In addition, the time required to obtain 50% of patients in remission was shorter in the Thy 3 group and required a lower cumulative activity of 131I. These same features, analyzed according to histology subtype, were more favorable in patients with the FV-PTC compared with patients with the classic and other variants. The clinical aspects of PTC and its variants have been recently reassessed. Taking into account extrathyroidal invasion, lymph node metastases and tumor stage, Shi et al. (17) confirmed the previously reported higher aggressiveness of the tall cell variant and underlined that the follicular variant has a much better prognosis compared with the classic variant. The overall mortality of patients with FV-PTC was only 0.6%. (17) A biological explanation for the less aggressive behavior of the follicular vs the classic variant of PTC derives from the results obtained by The Cancer Genome Atlas (TCGA) network (26). Indeed, RAS mutated tumors, which histologically correspond to the follicular variant, have a higher differentiation score compared with BRAF mutated tumors, which comprise the classic and other histological subtypes. The finding that the transcriptome of FV-PTC was indistinguishable from that of follicular adenomas provides a molecular explanation for the indolent behavior of these tumors (27). Patients with encapsulated FV-PTC rarely show recurrent disease (17), particularly those who have at a careful histological exam demonstrating absent capsular invasion—these cases are now classified as NIFTP (28 –30).
In our series of patients with confirmed carcinomas, the distribution of the histological type was remarkably different in patients with Thy 3 or Thy 4–5 cytologies. 64.4% of Thy 3 patients had FV-PTC, while 68.8% of Thy 4–5 patients had classic variant PTC. A higher prevalence of FV-PTC compared with CV-PTC in nodules that were diagnosed as follicular neoplasm or AUS at FNA was already reported by Liu et al. and VanderLaan et al. (24,25). In both series, the prevalence of CV-PTC was higher compared with the FV-PTC in the malignant category on cytology, while the distribution was similar in the suspicious for malignancy category compared with the follicular /AUS category.
Furthermore, out of 277 FV-PTC, 225 were available for revision. Out of these, 110 were encapsulated FV-PTC and among them 17 were reclassified as NIFTP (15 in Thy 3 and 2 in Thy 4–5).
Of note, patients included in the present study were treated with thyroidectomy and 131I during the period 2000–2010. According to the latest American Thyroid Association guidelines (10,11) many patients would have required a less aggressive treatment. However, we believe that our approach strengthens our study. Indeed, by aiming at total thyroid ablation, we were able to detect differences in the outcomes of the variants of papillary thyroid carcinoma that probably would not be so clear with a less aggressive treatment.
These results give strong support to recommend less aggressive treatment (i.e., lobectomy or clinical observation vs. total thyroidectomy) in patients with an indeterminate nodule on cytology.
Footnotes
Author Disclosure Statement
No competing financial interests exist.