
Abstract
Background:
The number of patients who need thyroid surgery has increased worldwide in recent decades. Patients with thyroid disease experience globus pharyngeus as a result of direct compression and edema of the surrounding organs. Thyroid surgery is needed to improve these symptoms or as treatment for thyroid cancer. After thyroid surgery, globus symptoms may become worse and may affect the daily life of the patient for a long time. Psychogenic problems have also been thought to cause the globus sensation. A prospective analysis of globus symptoms and psychogenic factors following thyroidectomy was performed.
Material and Methods:
Patients scheduled to undergo thyroid surgery between February and September 2016 completed the foreign-body sensation in the throat score (FBST; range 0–8.2) and the self-rating depression scale (SDS; range 0–100) preoperatively and three days, one month, three months, six months, and 12 months postoperatively.
Results:
Long-term follow-up was completed in 616 patients (491 females). A total of 365 patients had thyroid cancer, 169 had benign tumors, and 82 had diffuse goiters with Graves' disease. The percentage of patients who complained about neck discomfort (FBST >2) was 29.4% before surgery. A preoperative high FBST showed a significant direct correlation with a high SDS, but thyroid volume did not. A postoperative high FBST was seen in 75.3% of patients at two days and 78.9% at one month after surgery, and it then gradually decreased to 49.3% at 12 months after surgery. At three days after the operation, the median FBST was significantly higher in patients who had total thyroidectomy with lateral neck dissection or total thyroidectomy only compared to those who had lobectomy only (p < 0.05). These differences were still present 12 months after surgery. A higher preoperative SDS score was also identified as an independent predictor for a high FBST at 12 months after surgery, but not at one or three months postoperatively, on multivariate analyses.
Conclusion:
Preoperative globus symptoms appear directly related to psychological factors. The area of the surgical procedure and preoperative psychological factors were related to persistent neck discomfort.
Introduction
I
Globus is a persistent non-painful sensation of a lump or foreign body in the throat. Lee et al. reported that approximately 7–10% of people >50 years old have globus symptoms, and 45.6% of the general population had experienced a globus sensation at some time (2). The etiology of globus pharyngeus is still unknown. No consensus has been reached regarding how best to diagnose and manage globus pharyngeus. Detectable thyroid abnormalities are significantly more common in patients with globus pharyngeus than in controls (3 –8). Most patients with thyroid nodules experience globus pharyngeus as a result of direct compression and edema of surrounding organs by an enlarged thyroid gland. Thyroidectomy may be effective in relieving compressive symptoms, but some patients report nonspecific swallowing changes, discomfort, and dysphagia, even long after the surgical procedure (9 –12).
The number of patients who need thyroid operations for thyroid cancer has also increased worldwide because the incidence of thyroid microcarcinomas is on the rise (13).
All previous studies concerning globus symptoms have been small-scale studies, with short follow-up after the operation and no evaluation of the effects of the surgical procedure and psychological factors. Psychogenic problems have often been thought to cause the globus sensation. Up to 96% of patients with globus report symptom exacerbation during periods of high emotional intensity (14). Additional studies that include data gathered from longer follow-up periods are necessary to determine the exact prevalence and clinical impact of globus symptoms. This study investigated the frequency and severity of globus pharyngeus and their relationship with psychological factors after surgery.
Methods and Patients
After Institutional Review Board approval of the study protocol, patients at Ito Hospital who were scheduled to undergo thyroid surgery between February and September 2016 were recruited for this study. Patients with preoperative vocal cord palsy, those <15 years of age, and those with tracheostomies were excluded. Data were prospectively collected on patient demographic and clinicopathologic variables, including age, sex, surgical procedure, final histopathological diagnosis, and perioperative complications. Postoperative hypoparathyroidism was defined as intact parathyroid hormone <15 pg/mL on postoperative day 1. Recurrent laryngeal nerve paralysis was routinely diagnosed by laryngoscopic examination before and two or three days after surgery. Postoperative nausea was defined as symptomatic vomiting requiring anti-emetic pharmacotherapy. Neck stretching exercise was performed for all patients, except those who had laryngeal nerve anastomosis, at least three times a day beginning the morning following surgery. Patients performed the exercise slowly by themselves during their hospitalization and also after discharge.
Two questionnaire surveys were administered: the foreign-body sensation in the throat score (FBST), an evaluation score for patients complaining of globus pharyngeus symptoms (range 0–8.2) (15); and the self-rating depression scale (SDS) (16) to determine the extent of psychological distress. Responses were obtained from all patients preoperatively and three days, one month, three months, six months, and 12 months postoperatively. Patients with missing data were excluded from this study.
Evaluation score for patients complaining of globus pharyngeus symptoms
The FBST is an 11-item, condition-specific instrument (Table 1) (15). Each response was scored according to the magnitude of the FBST value. Each patient was asked to select one or two sentences that indicated the description most similar to his or her FBST from the list, and the average of the values attached to the selected sentences was regarded as the FBST value for the patient. The total score ranges from 0 (no problem perceived) to 8.2 (maximum perceived disability due to neck discomfort). FBST scores were divided into three groups: scores of <2 were categorized as asymptomatic; scores between 2.1 and 5 were categorized as mildly symptomatic; and scores >5.1 were considered severely symptomatic.
Patients choose one or two scores. When patients chose two responses, the score was calculated as the average of the scores for the two responses.
SDS
The SDS is a well-established tool for screening the severity of adult depression (16). The total score (range 20–80) is obtained by summing the scores for all of the individual items. Symptoms “over the past several days” are rated on a four-point (range 1–4) ordinal scale. Half of the items are worded positively, and half are worded negatively.
Statistical analysis
Statistical analysis was performed using JMP v12.0 software (SAS Institute, Cary, NC). The clinical data are presented as means ± standard deviation (SD), medians, or percentages. For the comparisons of pre- and postoperative data, Dennett's multiple comparison test was used. Fisher's exact analysis was used for univariate analysis. The Tukey–Kramer multiple comparison test was used to compare values at the same time between groups. p-Values of <0.05 were considered significant.
Results
Long-term evaluation was completed in 616 patients (491 females). The mean age was 49.6 years for males and 50.2 years for women. Demographic-, disease-, and treatment-related variables for this study cohort are summarized in Table 2. In terms of surgical history, 587 patients underwent primary surgery (no prior thyroid surgery), and 29 patients underwent a secondary intervention (one or more thyroid operations prior to this intervention). Perioperative hypoparathyroidism requiring calcium supplementation occurred in 152 (24.8%) patients. Eight (1.2%) patients showed recurrent laryngeal nerve palsy after surgery. Two of these patients had extrathyroidal invasion to the recurrent laryngeal nerve. All patients achieved recovery of vocal cord function within three months. Postoperative nausea occurred in 200 (32.6%) patients. One patient developed chyle leakage, and two patients developed neck hematomas; all three patients required re-operation.
Preoperative state
The median preoperative FBST was 1.35 (range 0–6.95). The percentage of patients who complained of neck discomfort (FBST >2) was 29.3% before surgery. Neck discomfort was related to Graves' disease but not thyroid cancer. A second surgery was associated with a slightly higher FBST (median 1.41, range 0–6.95), but it was not significantly different compared to primary surgery (median 1.33, range 0–5.85). The median FBST of patients with benign tumors with a thyroid volume >150 g and <150 g was 1.2 and 1.1, respectively. Thyroid volume in patients with benign thyroid tumors showed no significant correlation with throat discomfort.
The median SDS values of patients with Graves' disease, adenomatous goiter, and thyroid cancer were 39.4, 33.7, and 34.0, respectively; 54.9% of patients with Graves' disease, 24.3% of those with adenomatous goiter, and 29.8% of those with thyroid cancer had SDS >40. The SDS was higher in Graves' disease than in other diseases. Among patients with Graves' disease, thyroid volume was not related to a high SDS (p = 0.6548).
Table 3 shows the results of multivariate logistic analysis for factors predicting a severe foreign body sensation in the throat. Higher psychological factors (SDS >40) and female sex showed significant direct correlations with an increased foreign body sensation in the throat, but thyroid volume, older age, and thyroid disease did not.
SDS, self-rating depression scale.
Postoperative state
At three days postoperatively, 283 (45.9%) patients developed new compressive symptoms. The median FBST values at three days, one month, three months, six months, and 12 months postoperatively were 3.0 (range 0–7.65), 3.45 (range 0–8.2), 2.54 (range 0–8.2), 2.21 (range 0–7.1), and 1.99 (range 0–7.1), respectively. Postoperative deterioration of swallowing (FBST >2) was seen in 75.2% at three days and 78.8% at one month after surgery, and it then gradually decreased to 55.8% at three months and 49.3% at 12 months after surgery (Fig. 1).
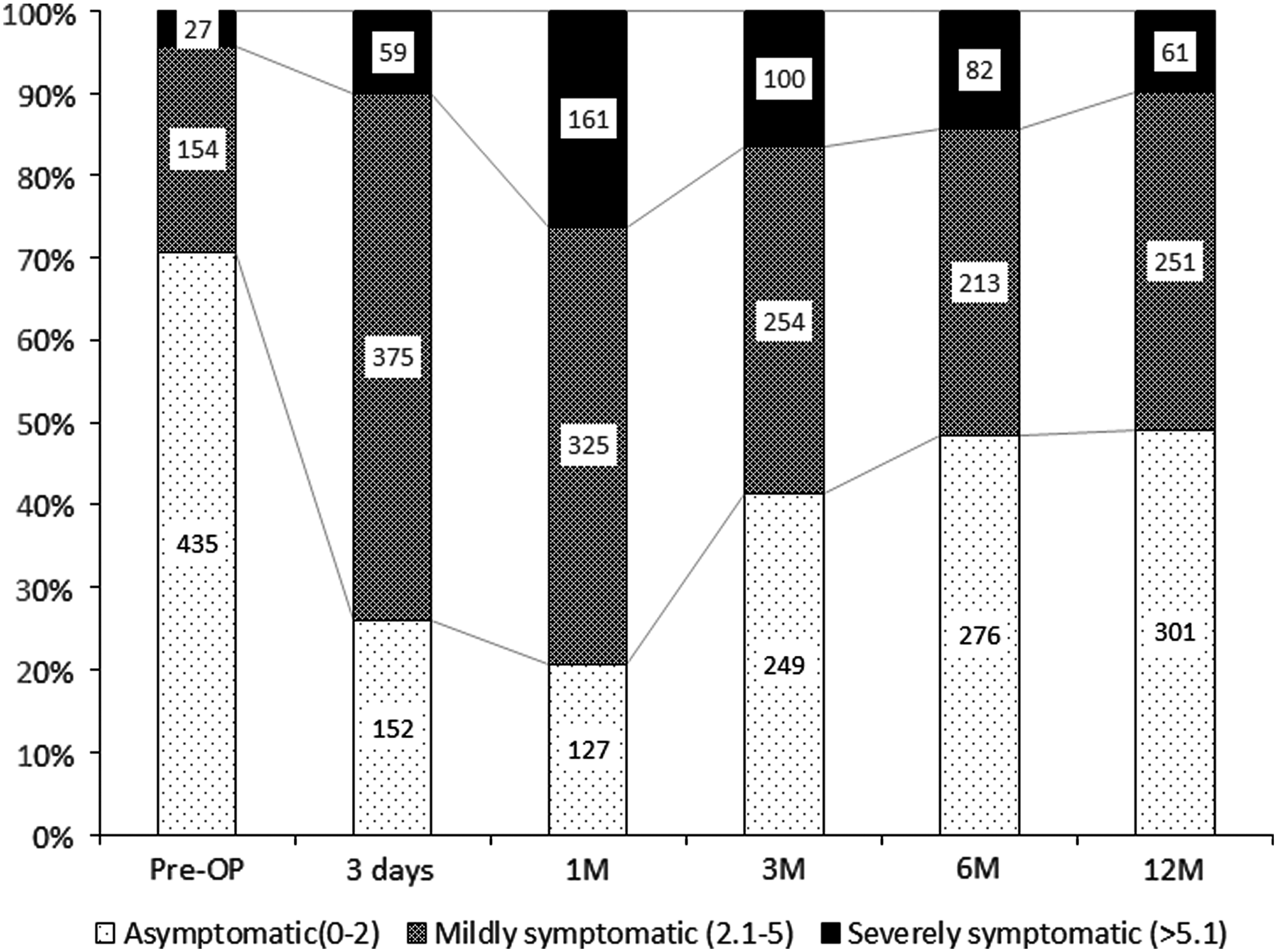
Distribution of patients in three classes of foreign-body sensation of the throat score (FBST) pre- and postoperatively.
Figure 2 shows the FBST at 12 months after surgery according to the level of the preoperative FBST; 59% of patients had globus symptoms equivalent to the preoperative period. Forty-seven (7.6%) patients had an improved throat sensation, and 32.8% had worsened globus symptoms.
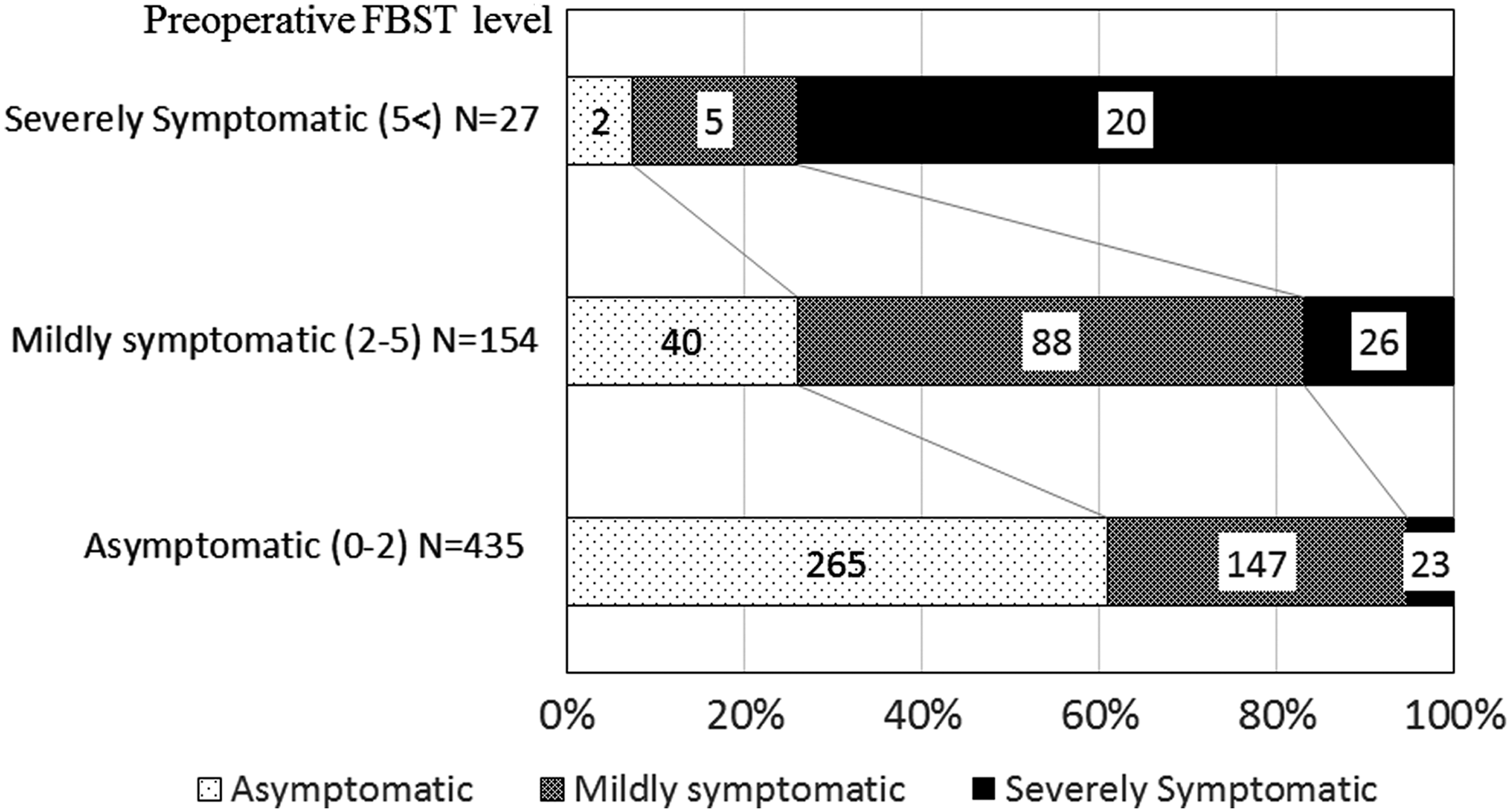
At 12 months after surgery, modification of the level of symptoms according to preoperative FBST.
Among the 27 patients with a preoperative severely symptomatic FBST, 25.9% reported improved symptoms, but others still complained that they were severely symptomatic. Forty percent of asymptomatic patients preoperatively developed mild or severe symptoms postoperatively.
To investigate the impact of surgical procedure on postoperative globus sensation, three groups were compared: total thyroidectomy (TT), lobectomy (LO), or TT with lateral neck dissection (LD). Figure 3 shows the time-dependent changes of FBST of the three groups. At one month after surgery, FBST was significantly higher among patients who had undergone TT with LD (median 4.68) than in patients who had TT only (median 3.74) or LO (median 3.26). The differences were still present at 12 months after surgery, and 60.4% of TT with LD patients had mild or severe symptoms.

Time-dependent change of FBST of the patients with a LO, TT or TT with LD. Significance levels: *p < 0.05. TT, total thyroidectomy; LO, lobectomy; LD, lateral neck dissection; Pre-OP, before surgery; Post 1, three days after operation; Post 2, one month post operation; Post 3, three months post operation; Post 4, six months post operation; Post 5, one year post operation.
The SDS of patients with Graves' disease decreased from 39.4 preoperatively to 33.1 at one month postoperatively, but that of patients with adenomatous goiter or thyroid cancer was stable. The percentage of Graves' disease patients with high SDS (>40) was 54.9% preoperatively, 37.8% at one month, and 34.1% at 12 months after surgery. The percentage of adenomatous goiter and thyroid cancer patients with high SDS (>40) at 12 months after surgery was 21.7% and 29.3%, respectively, and there was no change compared to the preoperative status.
Higher psychological factors (SDS >40) and surgical area (TT with LD) showed significant direct correlations with an increased foreign body sensation in the throat, but age and disease did not (Table 4).
TT, total thyroidectomy; LD, lateral neck dissection.
Discussion
Consortie et al. reported that the severity of globus symptoms was significantly decreased after thyroidectomy, mainly due to the improvement in strongly symptomatic patients (9). On the other hand, 20% of preoperatively asymptomatic patients developed symptoms, and 80% of mildly symptomatic patients remained symptomatic at three months after surgery. In the present study, 26% of preoperatively strongly symptomatic patients had improved globus symptoms, and 39% of preoperatively asymptomatic patients developed symptoms at 12 months after surgery. Among the 27 patients who were severely symptomatic before surgery, seven patients improved. Six (85.7%) of them had low preoperative SDS scores and benign disease. Though these numbers are very small, a low preoperative SDS might be a good indicator of globus symptom improvement.
The causes of patients' globus symptoms with thyroid disease differed in each perioperative period. In the preoperative state, the majority of patients presenting with aerodigestive compression or tumor volume complained of globus sensation. In the present study, no relationship between thyroid volume and globus symptoms was seen. Preoperative globus symptoms were associated with psychological factors. Comparing patients with Graves' disease and multinodular goiter at the same thyroid volume, patients with Graves' disease had a higher incidence of compressive symptoms. In the present study, the high rate of discomfort in patients with Graves' disease was related to high levels of emotional problems, regardless of thyroid volume.
Post-thyroidectomy patients complain of globus symptoms, although these symptoms frequently settle over time. Burns et al. examined a series of 200 patients who underwent thyroidectomy and found 58 (29%) patients with preoperative globus symptoms, which decreased to 12 (6%) by three to six months postoperatively (6). In the present study, these symptoms worsened around one month after surgery. Some of these symptoms resolved by three or six months later, but they remained in approximately 47.8% of patients at six months postoperatively. This strongly supports the possibility that functional problems were related to the healing process. Neck discomfort was due to inflammation and edema after surgery in the early period and laryngotracheal regional scar with fixation at one to three months after surgery. The surgical area in patients who had undergone TT or TT with LD was obviously wider than that in patients who had undergone LO. Patients who had undergone TT or TT with LD had more globus symptoms than those who had undergone LO, and this difference remained at 12 months after surgery.
Moreover, the patients presenting with globus symptoms had significantly higher levels of psychological distress than asymptomatic patients. Preoperatively, most patients had a mild emotional problem, such as anxiety about the operation, general anesthesia, and the stay in hospital. After surgery, some of these stressors vanished, but neck discomfort or pain appeared. The SDS was stable in patients with adenomatous goiter and thyroid cancer. However, the SDS of patients with Graves' disease decreased after surgery. This may be due to the thyroid function being normal and stable.
How to reduce and manage patients' globus symptoms is an important issue.
Scar tissue formation results in laryngotracheal fixation with impairment of vertical movement. The laryngotracheal fixation seems more evident with strap muscle division. The strap muscles are retracted routinely without sectioning them for benign tumors. However, in cancer cases, it is sometimes difficult to preserve the strap muscles if the cancer invades the surrounding tissue.
Stretching exercises may reduce neck discomfort (13). Wound healing and postoperative hemorrhage were no different between the no-stretching group and the stretching group. It is recommended that all patients begin similar exercises from the morning following surgery.
Patients also suffer mental anguish. Some patients with thyroid cancer have globus symptoms before surgery. After surgery, many patients worry about the possibility of a recurrence. Patients are concerned that globus symptoms may be a sign of recurrence, despite a lack of objective findings. For these reasons, it is important to inform patients about the risks of persistent globus symptoms after surgery.
Conclusion
Regardless of the cause, post-thyroidectomy globus symptoms are frequent, and some are persistent. It is important to know their frequency in order to inform patients and raise awareness.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare in relation to this manuscript.