
Abstract
Background:
Clinical laboratories are under pressure to increase value by improving test utilization. The clinical utility of reverse triiodothyronine (rT3) is controversial. A study was conducted to identify order patterns that might suggest inappropriate utilization of rT3.
Methods:
All orders for thyroid tests placed over a period of one year at a national reference laboratory were reviewed. Order patterns by client (hospital) and by provider were analyzed. A Pareto analysis was conducted to determine the percentage of orders placed as a function of the percentage of providers. A systematic review of the indexed literature and an informal review of the web were conducted to identify indications for rT3 testing.
Results:
There were 402,386 orders for 447,664 thyroid tests, including 91,767 orders for rT3. These orders were placed by 60,733 providers located at 1139 different organizations. Only 20% of providers who ordered thyroid tests placed an order for rT3. Of those who placed an order for rT3, 95% placed two orders or fewer for rT3. One hundred providers (0.1% of the 60,733 providers who placed orders for thyroid tests) accounted for 29.5% of the orders for rT3. Of the 100 providers, 60 with the highest order volumes for rT3 were classified as practitioners of functional medicine. A systematic review of Medline found little evidence to support the high volumes of orders for rT3. A survey of Web sites for functional medicine suggests that rT3 is useful for the diagnosis of rT3 dominance and can be used to direct triiodothyronine replacement therapy.
Conclusions:
There is wide practice variation in rT3 testing. A high proportion of tests are ordered by a relatively small proportion of providers. There is little evidence to support high volumes of rT3 testing placed by some practitioners.
Introduction
M
The measurement of reverse triiodothyronine (rT3) lacks guidelines and is controversial in the conventional medicine community. In general, conventional practitioners believe that rT3 measurements provide little value (2). However, the functional medicine community believes that rT3 measurements are useful as an indicator of thyroid dysfunction and a determinant of therapy. Thus, one might expect to see considerable practice variation with respect to rT3 testing.
Studies on practice variation can provide evidence regarding potential misutilization of laboratory tests. The authors previously reported on the significant variation observed in thyroid testing patterns across the United States. That work described the practice patterns for the most commonly available thyroid-related laboratory tests, as reported from >80 laboratories from >20 different healthcare organizations, and found significant practice variation in thyroid testing. Overall, the ordering pattern for rT3 was rare and notably concentrated, with few providers making up the majority of all rT3 test requests. This study expands upon that report by investigating test order patterns for rT3 received by a national reference laboratory from >1300 sites and 60,000 clinicians who ordered thyroid tests. The available evidence supporting the use of rT3 testing is also surveyed.
Methods
Survey of rT3 use
A query was performed to obtain all orders that included any thyroid test (thyrotropin, free thyroxine, total thyroxine, free triiodothyronine, total triiodothyronine, rT3, triiodothyronine uptake, thyroid binding globulin, thyroglobulin, thyroglobulin antibodies, thyroid peroxidase antibody, thyroid stimulating immunoglobulin, or thyroid stimulating hormone receptor antibody, performed at ARUP laboratories for a one-year period from November 1, 2015, to November 30, 2016). ARUP Laboratories is a reference laboratory that serves a nationwide clientele. The query included the client ID and ordering physician (provider). The number of orders was calculated for rT3 by client and by ordering physician. A client generally corresponds to a hospital or a group of hospitals.
Providers were given a unique identifier based on their name and client ID. Providers were given the name “unknown” if the name was missing. Thus, the orders from unknown providers associated with a particular client were aggregated as a single unknown provider. Unknown providers were excluded from the provider analysis because it was impossible to determine whether the aggregate unknown provider represented one or several providers. Unknown providers were retained in the client-level analysis.
It was hypothesized that providers who ordered large volumes of rT3 might be clustered by client. Hierarchical regression was used to test for an organizational effect controlling for client size (beds) and client type (academic, community).
The 100 physicians who had the highest order volumes of rT3 were identified, and a Google search was conducted to identify the specialty of each of these physicians.
The adult reference interval (≥18 years) for rT3 at the authors' laboratory is 9–27 ng/dL. The reference interval is independent of sex and age. There is no established reference interval for patients <18 years of age.
Literature and Web survey
A systematic review was conducted of the conventional literature on rT3. PubMed was searched on October 24, 2017, for all articles listed under the Medical Subject Heading (MeSH) term “Triiodothyronine, reverse” (PubChemID: 44123465). The search was restricted to human studies. The number of articles per year was determined. Clinical studies and diagnostic studies were identified, and the findings in these sets of articles were summarized. A search was also conducted of nonconventional literature by searching the Web for articles on rT3 (Google search for “reverse triiodothyronine”). The content of the top 150 pages identified by the Google search were categorized.
Results
rT3 order patterns
There were 402,386 orders for 447,664 thyroid tests (some orders were for more than one test). There were 91,767 orders for rT3. Orders for thyroid tests were placed by 60,733 providers (60,143 known; 590 unknown) from 1139 different clients. Known providers placed 53,657 orders for rT3.
rT3 values ranged from 2.5 to 947 ng/dL (median 15.5 ng/dL; interquartile range 12.4–19.4 ng/dL). rT3 was ordered more frequently for women (74%) than for men. On average, rT3 values were 2.2 ng/dL higher in men than in women (t = 22.4; p < 0.0005), and rT3 values increased 0.02 ng/dL for each year of age (t = 6.8; p < 0.0005). A total of 6.5% of orders were for patients aged <18 years. Abnormal rT3 results were independent of sex (p = 0.66), and although the effect size was small (odds ratio = 1.01), abnormal rT3 results had a statistically significant association with age (p < 0.0005).
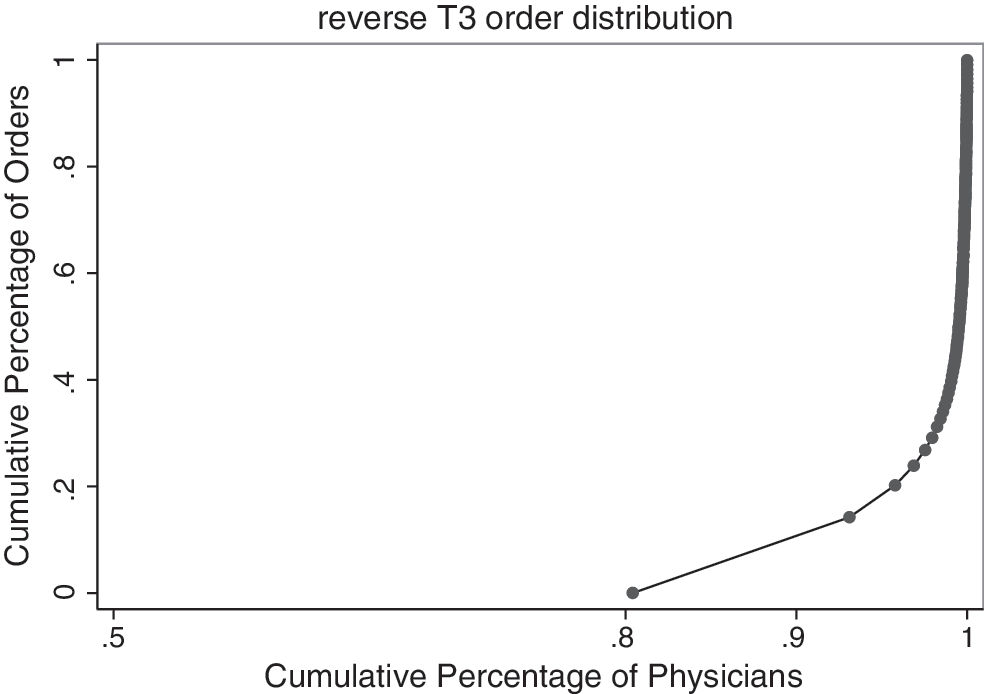
A relatively small proportion of providers accounted for the majority of rT3 orders (Fig. 1). Eighty percent of providers who placed an order for a thyroid-related test never ordered rT3. Of 60,143 providers, 57,606 (95%) ordered at most two rT3 during the year. The 100 providers with the highest rT3 order volume (0.1% of all 60,143 providers, 0.8% of the 11,782 providers who ordered at least one rT3) accounted for 15,823/53,657 (29.5%) of rT3 orders.
Distribution of reverse triiodothyronine (rT3) orders by providers. Eighty percent of providers who ordered thyroid-related tests did not order rT3.
Provider order volume was clustered within clients (χ2 1 = 146; p < 0.001) Bed size and facility type (academic, community) were not associated with provider order volume (p = 0.42 and 0.28 for bed size and facility type, respectively). Of 80 known providers who ordered >100 rT3 tests per year, 16 were associated with one client.
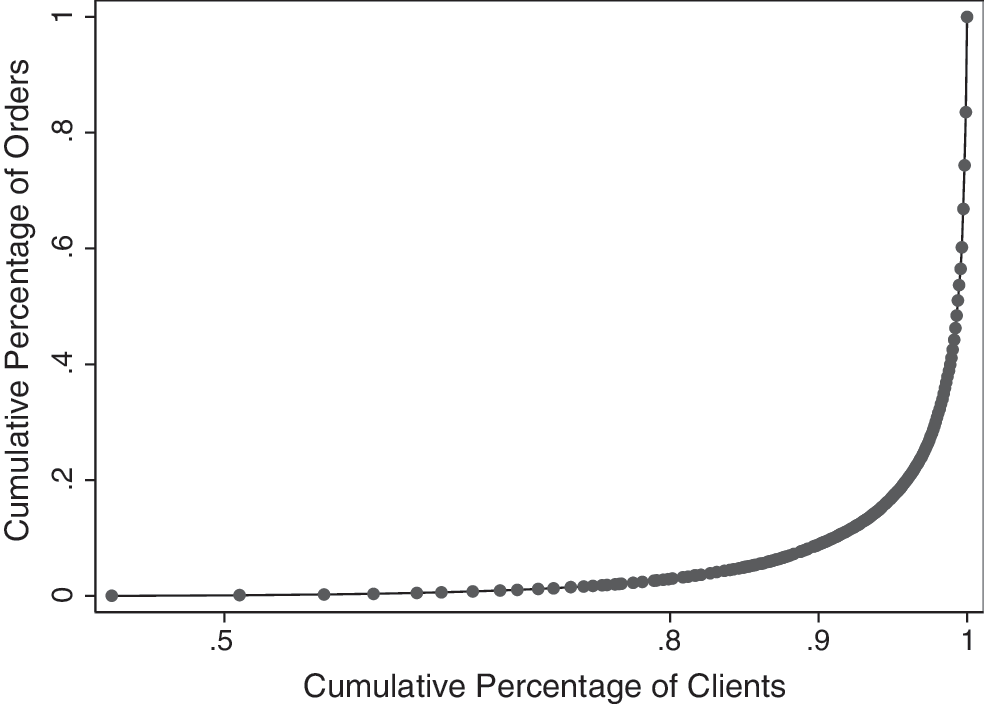
The pattern of client orders showed a similar pattern (Fig. 2). Forty-two percent of clients who placed an order for a thyroid-related test did not order a rT3 over the course of the year. Of 1139 clients 646 (57%) ordered two or fewer T3. The 10/1139 (0.9%) clients with the largest order volume accounted for 51,173/91,767 (56%) rT3 orders.
Distribution of rT3 orders by clients. Forty-two percent of clients who ordered thyroid-related tests did not order rT3.
The rate of positive findings (i.e., rT3 outside the reference interval) was inversely related to the order volume (Fig. 3). Providers who ordered high volumes of rT3 (>10/year) had lower rates (<0.1) of positive findings (χ2 1 = 754; p < 0.0005).
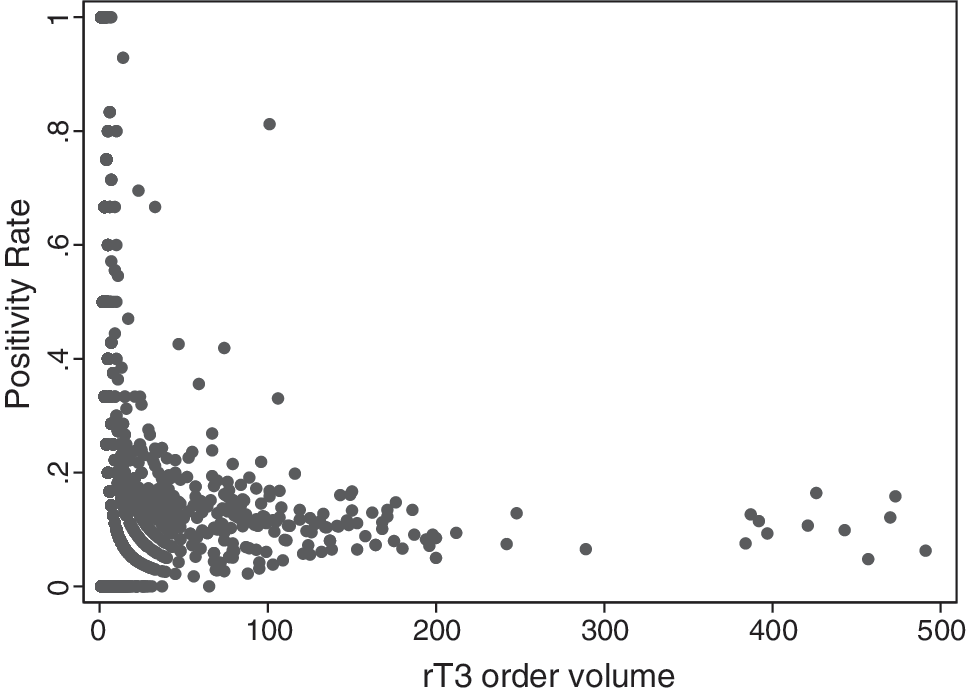
Rate of positive findings by order rate. The graph shows the positive finding rate as a function of the rT3 order rate. Each dot represents a provider.
Of the 100 providers with the highest order volume for rT3, 60 (60%) were classified as practitioners of functional medicine (Table 1). The 40 remaining providers were distributed across multiple specialties. Thirty-four of the high-volume providers were MDs, 16 were doctors of osteopathy, and 19 were naturopaths.
The table contains the specialties of the providers with the 100 highest order volumes (range 186–491 rT3 per year).
rT3, reverse triiodothyronine; MD, allopathic doctor of medicine; DC, doctor of chiropractic medicine; DO, doctor of osteopathy; NMD, doctor of naturopathic medicine; ML, midlevel provider.
Survey of evidence on rT3
The PubMed search identified 1387 articles on rT3. Of these, 895 were conducted in humans. Ninety percent of the 895 articles were published before the year 2000. An average of 5.6 articles per year have been published on rT3 since the year 2000 (Fig. 4). Seventy-two percent (648/895) of the articles were published between 1978 and 1989. The set of articles included 51 clinical trials and 60 articles on diagnosis of disease in humans.
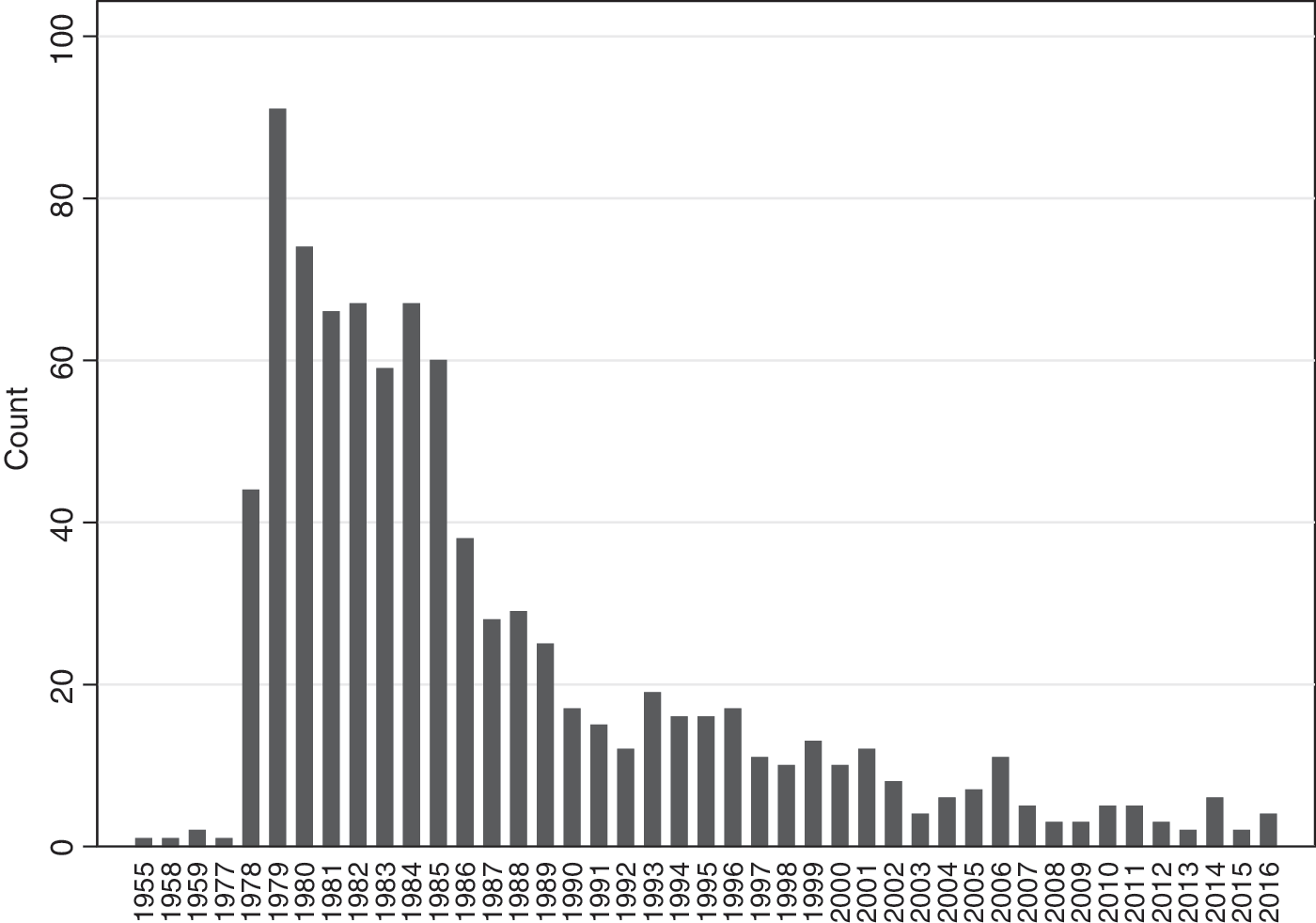
Publication count of articles on rT3 by year. Search limited to articles on humans.
The systematic review of the conventional literature found limited evidence to support the clinical use of rT3 and, when present, only for very narrow indications. Fifty-one clinical studies were identified, and almost all of the clinical studies monitored the impact of a drug or clinical condition on thyroid hormone concentrations, including rT3. One study suggested that rT3 could be used as a prognostic marker for outcomes in critically ill patients (3). Thirty-four prognostic studies were identified. Many of these studies showed significant associations between rT3 concentrations and prognosis in critically ill patients (3 –17). However, it is not clear how rT3 compares to other prognostic factors or how often rT3 is used for this purpose. No specific uses were found for rT3 among 61 diagnostic studies. One unpublished meeting abstract claimed that elevated rT3 was associated with subclinical hypothyroidism (18).
A Google search for “reverse triiodothyronine” obtained 207,000 results. The top 150 pages that were identified in the search were categorized (Table 2). The majority of Web pages (49%) were links to PubMed articles. Of the pages that focused on medicine (diagnosis, therapy, prognosis), 16 pages (11%) were associated with functional medicine, and two pages (1%) were associated with conventional medicine.
Discussion
It was found that orders for rT3 are concentrated among relatively few providers and clients. Among providers who ordered thyroid-related tests, 0.1% of providers accounted for 29% of rT3 orders. Similarly, approximately 1% of clients accounted for 56% of orders for rT3. Further, it was found that providers who order high volumes of rT3 tend to be clustered within clients. It was found that results from providers who order high volumes of rT3 tend to have a lower clinical yield (i.e., a lower rate of abnormal findings) than orders from providers who placed relatively few orders for rT3. Finally, it was found that specialists in functional medicine are highly represented among the providers who order the highest volumes of rT3.
The highly skewed distribution of rT3 test utilization suggests that there is significant practice variation with respect to rT3 measurements. The wide practice variation suggests misutilization. Given the lack of evidence to support the usefulness of high volumes of rT3 testing, the data suggest that rT3 testing is overutilized by a small proportion of practitioners.
In conventional practice, rT3 is considered an inactive metabolite of the thyroid hormone thyroxine (T4), as opposed to the conversion of T4 into the active T3. The inability of rT3 to exert the same energy and metabolism-related effects as T3 supports its definition as an inactive hormone representative of the catabolic state. It has been proposed that favoring the alternative rT3 metabolic pathway may serve as a mechanism to conserve energy in times of severe illness or starvation (19 –21). Elevated concentrations of rT3 are the norm in nonthyroidal illness (NTI) or sick euthyroid syndrome and “low T3 syndrome” (decreased T3 and elevated rT3 concentrations). Therefore, its measurement is rarely useful in hospitalized patients (22). In most laboratories, rT3 is sent to a referral testing site, and the long turnaround time may further limit its utility, particularly in inpatient settings. The indications for rT3 testing in ambulatory care are very limited. For example, rT3 measurements can be helpful in the diagnosis of thyroid hormone cell membrane transport defects, thyroid hormone metabolism defects, and consumptive hypothyroidism (23 –25).
It has been reported that rT3 concentrations increase with age, proposedly due to diminished renal metabolism and eventual degradation of rT3 in the liver (26,27). This rise in rT3 may, in part, reflect underlying illness or malnutrition in the aging population, similar to that described in hospitalized patients. Elevations in free T4 and rT3 hormone concentrations have been associated with lower physical and mental functionality scores in elderly men (28), but the strong correlation between the T4 and rT3 values is consistent with the notion of concurrent illness, which may explain these lower scores.
One situation where rT3 testing may be helpful is to distinguish central hypothyroidism from NTI in hospitalized patients. While other thyroid tests, such as TSH and free T4, may be similarly low in these two conditions, rT3 is usually also low in central hypothyroidism and high in patients with NTI. Even here, however, a good clinical evaluation by an experienced clinician will usually provide the accurate diagnosis in the absence of a rT3 measurement. The distinction between primary hypothyroidism and NTI is much more straightforward, since the serum TSH is elevated in primary hypothyroidism and usually low in NTI until the recovery phase when it is transiently mildly elevated. A seasoned clinician and even less experienced providers usually have no problem making this distinction without the added expense of a rT3 measurement. There are also some rare conditions such as consumptive hypothyroidism, MCT8 mutations, and SBP2 mutations where rT3 measurements can be helpful in characterizing the phenotype and the underlying mechanism of disease (23,29,30). Therefore, for the conventional medical community, the clinical indications for use of rT3 testing are very limited, and it remains an unusual request. Its use is not referred to or supported in routine clinical practice guidelines related to thyroid disease testing or management (31). This is presumably due to minimal evidence of rT3 utility found in the primary literature.
The functional medicine community believes that tissue concentrations of T3 are the key determinant of thyroid function and that serum concentrations of T3 are sometimes a poor indicator of thyroid hormone concentrations at the tissue level (32,33). Functional medicine hypothesizes that rT3 competes with T3 at binding sites so that elevated rT3 can cause hypothyroid symptoms when T3 concentrations are normal (34,35). This is known as rT3 dominance. It is proposed that a number of conditions such as liver disease, kidney disease, stress, chronic alcohol abuse or other drug abuse, and simple aging can lead to increases in rT3, which in turn leads to rT3 dominance. These practitioners recommend the use of the rT3/T3 ratio to diagnose rT3 dominance. When the rT3/T3 ratio is elevated in the setting of hypothyroid symptoms and normal TSH, T3, and free T4, these practitioners suggest therapy with thyroid hormone supplementation (34). However, the affinity of T3 for the T3 receptor is 100-fold higher than the affinity of rT3. Therefore, the notion that rT3 can compete with T3 for occupancy of the T3 receptor is not consistent with current scientific data (36). Moreover, no studies were found in the conventional literature that recommend interventions based on rT3 concentrations.
Functional medicine practitioners treat patients with a rT3 dominance profile (hypothyroid symptoms, elevated rT3 and normal T4) with hormone supplementation (liothyronine or desiccated thyroid hormone preparations). Functional medicine practitioners sometimes prescribe cofactors for enzymes involved in thyroid metabolism or nutrients that are considered important for thyroid health such as selenium, zinc, iron, iodide, and vitamins C, D, and E. These nutrients are thought to enhance the conversion of T4 to T3 rather than rT3 and provide an alternative to T3 supplementation (37). However, according to conventional medicine, the only known intervention that increases T4 to rT3 conversion is the administration of glucocorticoids (38). There is little or no published evidence to support the rT3 dominance hypothesis or the interventions based on the theory.
Is the rT3 dominance hypothesis plausible? There is evidence that many diseases and medications lead to changes in thyroid hormone concentrations (39,40). It is theoretically possible that rT3 might compete for T3 receptors. However, the evidence suggests that this is not the case. One study from almost 30 years ago suggested that rT3 had an had an affinity for placental nuclear binding sites that was 40 times greater than thyroxine and 63 times greater than triiodothyronine (41). Another study suggested that rT3 represses thyroid-regulated genes in mice (42). However, in contrast, another study showed that the relative affinity of rT3 to T3 for solubilized nuclear T3 receptors was 0.01 (36). In addition, T3 is present in much higher concentrations than rT3. The reference range for the T3/rT3 ratio is 4.2–11.0 (43). The T3/rT3 ratio remains >1.0, even in illness (3). Because of the transient function of the placenta and its unique deiodinase profile, it is certainly questionable whether T3 receptor binding in this tissue is representative of the rest of the body's tissues. In contrast, studies of T3 receptors in the human liver and kidney have demonstrated that the affinity of T3 for the T3 receptor is 100-fold higher than that for rT3 (34). This certainly casts doubt on the ability of rT3 to compete with T3 for receptor occupancy and therefore of the validity of the concept of rT3 dominance.
Much of the evidence from the functional medicine practitioners appears to be based on anecdotal evidence that patients with symptoms and laboratory values consistent with rT3 dominance experience symptom relief with T3 therapy. From the perspective of conventional medicine, such evidence is suggestive, but could also be explained by a placebo effect. Also, some of the effect of T3 supplementation might be explained by the fact that supra-physiologic doses of T3 can work as a mood enhancer in depressed patients (44). The symptoms of hypothyroidism (fatigue, trouble thinking, and weight gain) are very nonspecific and are frequently experienced by healthy people. rT3 concentrations are also elevated in chronic illness/malnutrition. The T4/rT3 ratio generally remains constant, and glucocorticoids are the only factors know to alter this ratio (38). Thus, nutritional interventions are unlikely to be effective. Overall, it appears that there is no published evidence to support the rT3 dominance theory. However, it is important to bear in mind that “absence of evidence is not evidence of absence” (45).
What types of studies are needed to determine whether measurement of rT3 has clinical utility? Functional medicine believes that patients with an rT3 dominance profile (hypothyroid symptoms, elevated rT3, and normal T4) can be treated with thyroid hormone supplementation. However, to the authors' knowledge, this hypothesis has never been tested in a clinical trial. Therefore, a double-blinded randomized trial with patients fitting the rT3 dominance profile (arm 1) and patients with normal rT3 profile (arm 2) and treatment with placebo or T3 supplementation could verify the claims that patients with an rT3 dominance profile benefit from T3 supplementation. Similarly, double-blinded placebo-controlled randomized trials to determine whether nutritional interventions provide symptomatic relief for patients with an rT3 dominance profile might be illuminating. Studies on competitive binding of rT3 and T3 could rule out the rT3 dominance theory if rT3 did not interfere with T3 binding. Results showing that rT3 competes with T3 would be consistent with the rT3 dominance theory but would not be conclusive. Experimental studies showing that exogenous rT3 has an impact on basal temperature and other physiological parameters mediated by T3 would also support the rT3 dominance theory. However, it has been shown that administration of rT3 does not change serum TSH concentrations (46). If rT3 were active, it would be expected to alter TSH concentrations. These studies would be relatively inexpensive and could provide data to guide the use of rT3 testing.
This study found that the authors' laboratory received approximately 91,000 orders for rT3 in one year. On a national basis, it is suspected that the order volume for rT3 is at least one million. Each rT3 test costs about $20 (average list price of commercial laboratories; range $7.00–46.25). It is unclear whether these orders provide value. If rT3 measurement provides no value, there could be an opportunity for significant savings at sites with high order rates for rT3. Given the current emphasis on laboratory utilization, it seems that studies on the utility of rT3 are warranted and would most likely be cost-effective. Since the evidence suggests no utility for rT3, the burden of proof is on the functional medicine community to design scientific studies that support its clinical utility.
This study has several limitations. Practice variation suggests misutilization but is not conclusive. The study only identified order patterns but did not determine the reason why individual orders were placed. A survey or interviews of users might identify the reasons for test orders and identify hypotheses that could be tested. rT3 is generally performed by reference laboratories, but routine thyroid tests are performed at most hospitals. Thus, the estimate of the percentage of physicians who order rT3 is likely to be high because most thyroid testing would be performed locally. The review of the conventional literature was systematic. However, the review of the web literature was informal. Finally, the study found a lack of evidence to support rT3 testing. However, a lack of evidence does not prove a lack of effect. Additional studies are needed to determine the clinical utility of rT3.
In summary, this study shows significant practice variation in rT3 testing. A high proportion of tests are ordered by a relatively small proportion of providers, and much of the use of rT3 testing appears to be driven by functional medicine. At present, there is little evidence to support the high volume of rT3 testing requested by this community.
Footnotes
Author Disclosure Statement
Drs. Schmidt and Straseski are medical directors at ARUP Laboratories, which performs rT3 testing. ARUP Laboratories is a nonprofit organization that is wholly owned by the University of Utah.