
Abstract
Background:
Exclusion of analytical interference is important when there is discrepancy between clinical and laboratory findings. However, interferences on immunoassays are often mistaken as isolated laboratory artefacts. The mechanism of a rare cause of interference in two patients that caused erroneous thyroid function tests, and also affects many other biotin dependent immunoassays, was characterized and reported.
Patient findings:
Patient 1 was a 77-year-old female with worsening fatigue while taking carbimazole over several years. Her thyroid function tests, however, were not suggestive of hypothyroidism. Patient 2 was a 25-year-old female also prescribed carbimazole for apparent primary hyperthyroidism. Despite an elevated free thyroxine, the lowest thyrotropin on record was 0.17 mIU/L. In both cases, thyroid function tests performed by an alternative method were markedly different. Further characterization of both patients' serum demonstrated analytical interference on many immunoassays using the biotin–streptavidin interaction. Sandwich assays (e.g., thyrotropin, follicle-stimulating hormone, troponin T, beta-human chorionic gonadotropin) were falsely low, while competitive assays (e.g., free thyroxine, free triiodothyronine, TSH binding inhibitory immunoglobulin) were falsely high. Pre-incubation of serum with streptavidin microparticles removed the analytical interference, initially suggesting the cause of interference was biotin. However, neither patient had been taking biotin. Instead, a ∼100 kDa immunoglobulin M (IgM) immunoglobulin with high affinity to streptavidin was isolated from each patient's serum. The findings confirm IgM anti-streptavidin antibodies as the cause of analytical interference.
Summary:
Two patients with apparent hyperthyroidism as a result of analytical interference caused by IgM anti-streptavidin antibodies are described.
Conclusion:
Analytical interference identified on one immunoassay should raise the possibility of other affected results. Characterization of interference may help to identify other potentially affected immunoassays. In the case of anti-streptavidin antibodies, the pattern of interference mimics that due to biotin ingestion. However, the degree of interference varies between individual assays and between patients.
Introduction
A
Two patients are reported with unusual thyroid function tests incongruent to their clinical findings. Neither patient had been taking biotin. However, both demonstrated interference causing falsely high results on competitive assays and falsely low results on sandwich assays. After written consent, a separate collection of serum was obtained from both patients, and an attempt was made to characterize this interference further.
Patients
Patient 1 was a 77-year-old female who presented in 2016 with worsening fatigue on carbimazole 10 mg twice daily for hyperthyroidism. However, clinically, she now reported symptoms of hypothyroidism. She had originally been diagnosed with Graves' hyperthyroidism and coeliac disease in 2009. After initial treatment with carbimazole, she was diagnosed with a relapse in 2012. However, the lowest TSH on record was 0.21 mIU/L (reference interval 0.27–4.2 mIU/L). On examination, there was a small, smooth goiter but no bruit or signs of Graves' ophthalmopathy. Despite symptoms of hypothyroidism, thyroid function tests performed at the time by the Roche Cobas method were: TSH 0.75 mIU/L (0.27–4.2 mIU/L), fT4 12 pmol/L (12–22 pmol/L), and fT3 8.1 pmol/L (3.9–6.8 pmol/L). TBII was detected at low levels of 3.8 IU/L (<1.3 IU/L) using a Roche Cobas assay. Given the unusual presentation, thyroid function tests were repeated on a Siemens Centaur platform, which suggested biochemical hypothyroidism: TSH 37 mIU/L (0.3–4.0 mIU/L), fT4 7 pmol/L (10–20 pmol/L), and fT3 3.0 pmol/L (3.0–6.5 pmol/L), more in keeping with her symptoms and clinical examination.
Patient 2 was a 25-year-old female who was started on 20 mg/day of carbimazole for apparent hyperthyroidism in 2013 and referred for further assessment. By the time of clinic review, she was in the first trimester of pregnancy and as a result had stopped carbimazole of her own volition. Her symptoms, which were compatible with hyperthyroidism, including anxiety, tremor, shortness of breath, and loose bowel motions, had gradually improved since pregnancy. On examination, there were no signs of thyroid eye disease or goiter. However, a fine tremor was noted. Thyroid function tests performed by the Roche Cobas method at the time demonstrated a high fT4 of 31.9 pmol/L (12–22 pmol/L) and fT3 9.4 pmol/L (3.9–6.8 pmol/L), without suppression of TSH, which was 0.33 mIU/L (0.27–4.2 mIU/L). It was also noted that the lowest TSH on record was 0.17 mIU/L (0.27–4.2 mIU/L). Repeating thyroid function tests using an alternative method (Abbott Architect) demonstrated biochemical euthyroidism, and testing of TBII by a radioimmunoassay method (RSR Ltd.), not dependent on biotin–streptavidin interaction, was negative. The overall findings suggested analytical interference and excluded hyperthyroidism as the cause of her symptoms.
Characterization and identification of interference
Serum from both patients was tested by immunoassays from Roche Cobas (biotin–streptavidin based method) and Siemens Centaur. Their serum was also pre-incubated with streptavidin microparticles (SM), as previously described (7), or with heterophile blocking tubes (HBT; Scantibodies, Inc.) before retesting by Roche immunoassays. Although differing in magnitude, both patients demonstrated analytical interferences in the same direction on multiple assays, except on the testosterone assay where interference was not detected in patient 2 (Table 1). Pre-incubation of control serum with SM had no effect (Supplementary Table S1; Supplementary Data are available online at
Sera from two patients with streptavidin antibodies were incubated with SM or HBT prior to assay. Interference was considered present if >20% difference was observed. Elecsys® immunoassays relying on the streptavidin–biotin interaction were performed on a Roche Cobas E602. Results were compared to an unaffected method on the Siemens Centaur (Supplementary Table S1). A very high digoxin level was also detected in patient 2, despite not being prescribed this medication. Stated ranges are for post-menopausal patients (patient 1).
Estradiol, LH, and FSH ranges are lower in patient 2, a 25-year-old pre-menopausal patient (follicular ranges): LH 2–8 IU/L; FSH 3–10 IU/L; estradiol 50–850 pmol/L.
SM, streptavidin microparticles; HBT, heterophile blocking reagent; fT4, free thyroxine; fT3, free triiodothyronine; TBII, thyrotropin binding inhibitory immunoglobulin; TSH, thyrotropin; LH, luteinizing hormone; FSH, follicle-stimulating hormone; PTH, parathyroid hormone; NA, testing on alternative platform not performed; ↓, falsely low; ↑, falsely high; —, no interference detected.
Pooled residual sera containing high concentrations of HT Troponin T, NT-pro-BNP, beta-HCG, and progesterone were mixed with patients' sera containing anti-streptavidin antibodies. Immunoassay results were obtained before (neat) and after pre-incubation with streptavidin microparticles (SM). Results for each analyte were low or undetectable prior to mixing studies. The final mixture did not contain more than 20% (v/v) residual pooled sera. Reference intervals for the Roche platform for post-menopausal females are provided.
Although pre-incubation with SM detected interference, neither patient had a history of biotin ingestion. Further, serum biotin was not increased in either patient when tested by an academic research laboratory utilizing tandem-mass spectrometry. An alternative compound with an unusually high affinity to streptavidin was hypothesized as the cause of interference. This interfering compound was eluted from SM by the addition of citric acid (0.1 M). Following sodium dodecyl sulfate polyacrylamide gel, two bands were found (Fig. 1). Peptide sequencing of the heavier band (MW: ∼100 kDa) identified it as the heavy chain of immunoglobulin M (IgM; see Supplemental Data: Peptide Sequencing). No protein band was eluted following pre-incubation of control patient serum. The findings demonstrate the cause of interference as anti-streptavidin antibodies of IgM isotype in both patients.
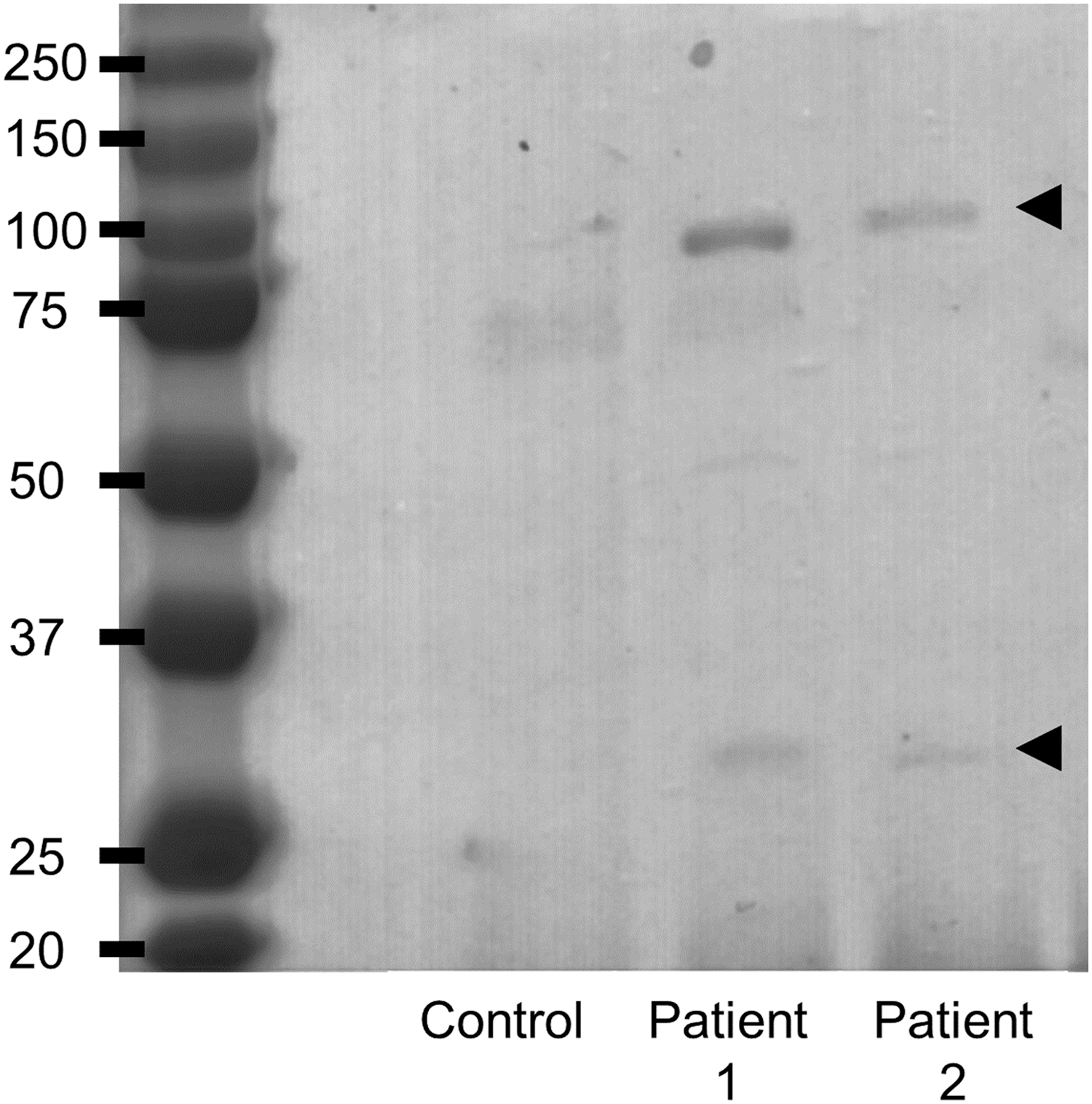
Molecular weight of protein bound to streptavidin microparticles in two patients with anti-streptavidin antibodies. Sodium dodecyl sulfate polyacrylamide gel of protein eluted from streptavidin microparticles identified a heavy (∼100 kDa) and light band (25–37 kDa) corresponding to immunoglobulin M (IgM) heavy chain and light chain (arrow heads). Elution of protein was carried out by incubation of streptavidin microparticles with 0.1 M of citric acid at 56°C for 15 minutes following three washes with phosphate-buffered saline. Protein was visualized by staining the gel with Coomassie blue. IgM heavy chain was confirmed in both patients by proteolytic digestion and peptide sequencing (see Supplemental Data: Peptide Sequencing).
Discussion
Two patients are described with unusual thyroid function tests with persistent analytical interference in specimens collected four and seven years since first presentation. Neither patient had a history of biotin use. However, pre-incubation of each patient's serum with SM removed the interfering compound. In each patient's serum, a ∼100 kDa protein with affinity for streptavidin was isolated. Peptide sequencing of this protein confirmed IgM anti-streptavidin antibodies. Similar to interference from biotin, a large number of assays were affected, with falsely high results on competitive assays (e.g., fT4, fT3, TBII, Digoxin) and falsely low results on sandwich assays (e.g., TSH, follicle-stimulating hormone, troponin T, human chorionic gonadotropin). However, the degree of interference otherwise varied unpredictably between assays and patients.
In both patients, analytical interference led to unnecessary treatment with carbimazole, anxiety for the patients, and significant confusion for clinicians involved. Carbimazole was discontinued in patient 1 with resolution of the fatigue. Both patients were biochemically euthyroid using immunoassays not utilizing the biotin–streptavidin interaction. They and their doctors were advised that future results from immunoassays using biotin–streptavidin interaction should be interpreted with caution and testing by alternative platforms should be sought.
Analytical interferences on immunoassays can be broadly categorized as interferences that alter the measurable concentration of the analyte (e.g., effect of thyroxine-binding globulin on total T4 or macroprolactin on prolactin assays) or interferences that alter antibody binding or the assay reaction (8). The causes of this latter category include heterophile antibodies, human anti-animal antibodies, paraproteins, biotin, or endogenous antibodies that target reagents (e.g., anti-ruthenium antibodies). In these cases, altered antibody binding may result in analytical interferences on multiple immunoassays. When these interferences are suspected, a range of laboratory procedures can be used to detect analytical interference in immunoassays. In addition to what has been described in this report, serial dilution, the presence of rheumatoid factor, polyethylene glycol precipitation, and pre-adsorption with protein A/G may be helpful in selected cases (8). However, no single procedure is sufficiently sensitive and robust to detect all causes of analytical interference. The laboratory findings of unexplained apparent high serum estradiol or drugs such as digoxin (Table 1), which had not been prescribed to the patient, may be helpful as a rapid screening test to detect analytical interferences caused by biotin or anti-streptavidin antibodies.
Recently, multiple laboratories, including the authors' (7), have described the use of SM in the detection of analytical interference caused by biotin ingestion (9,10). As demonstrated in this case report, treatment with SM is also effective at detecting interference caused by anti-streptavidin antibodies. The presence of anti-streptavidin antibodies competes with biotinylated reagents used in immunoassays. As the binding of biotinylated reagents to streptavidin is required to retain signal generating antibody complexes, the presence of anti-streptavidin antibodies leads to a reduction in signal observed in immunoassays in a similar manner to ingested biotin (Fig. 2). As the signal intensity is directly proportional to the concentration in sandwich assays, a reduction in signal caused by biotin or anti-streptavidin antibodies translates to artificially low sandwich immunoassay results. In contrast, signal intensity is inversely proportional to concentration on competitive assays, resulting in artificially increased results.
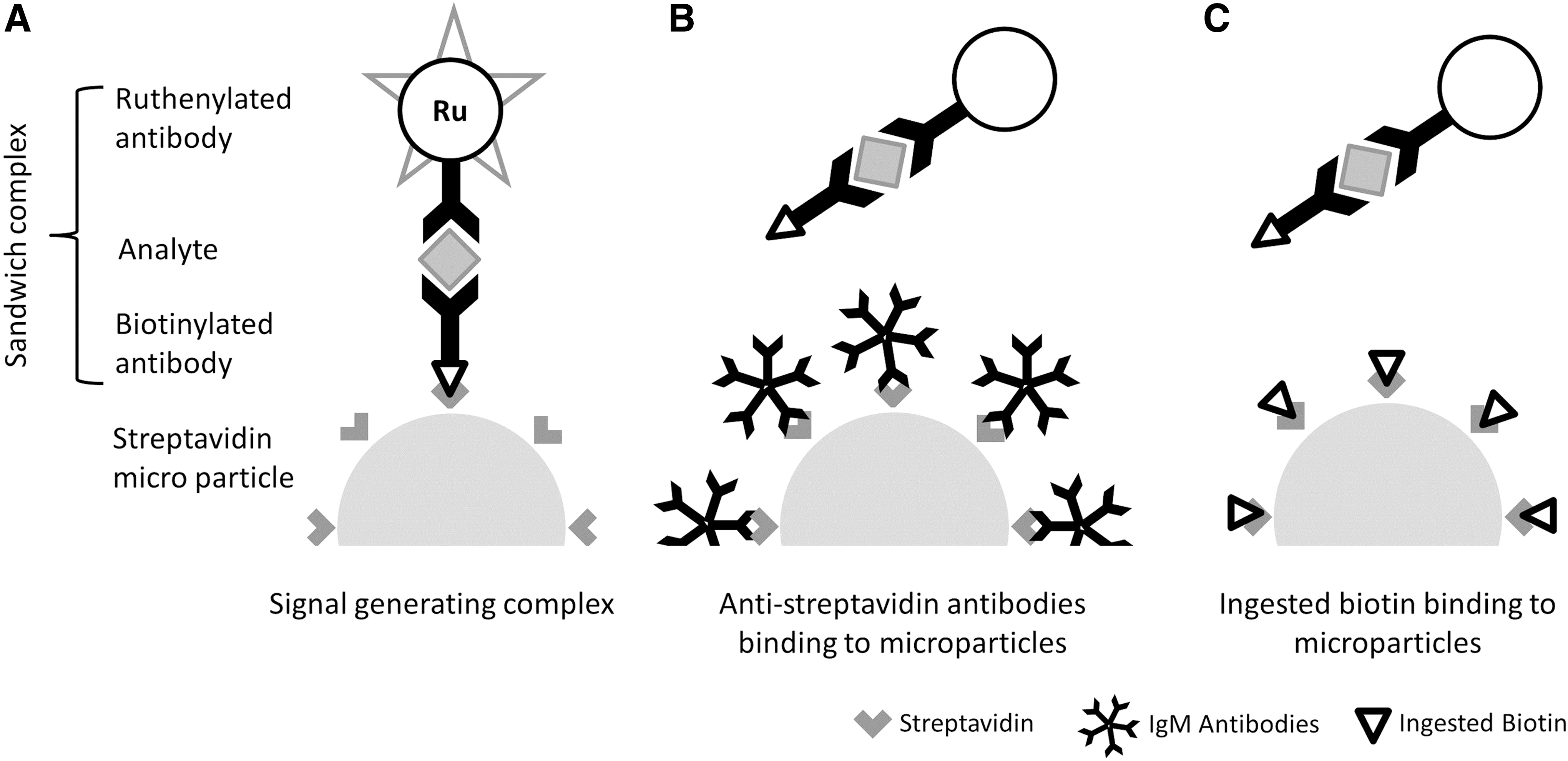
Mechanism of interference caused by anti-streptavidin antibodies and biotin on sandwich assays. Signal can only be generated when biotinylated reagents bind to streptavidin microparticles on Roche Cobas electrochemiluminescence immunoassays (
While a history of biotin ingestion or supplement use may identify the cause of interference, this information is often absent or unreliable. Unfortunately, most laboratories do not have the ability to measure serum biotin directly. In these instances, interference caused by biotin could be differentiated from anti-streptavidin antibodies by the significant fluctuations between consecutive laboratory results. This is due to the dissipating interfering effects of biotin within several hours of ingestion with the complete normalization of thyroid hormones and TSH results within 48 hours (7,11). Alternatively, the combination of heterophile blocking reagents, protein A/G, or polyethylene glycol methods was successful in detecting the interfering effects of anti-streptavidin antibodies in five of six patients (Supplementary Table S2), including the two patients from this report.
Multiple immunoassay interference leading to apparent biochemical hyperthyroidism has been described in all previous case reports of analytical interference suspected to be caused by anti-streptavidin antibodies (Supplementary Table S2). While the antigenic source of these antibodies at this stage has not been determined, this interference is likely significantly under-recognized. As demonstrated in a recent study, using a semi-automated research assay that detects IgG anti-streptavidin antibodies, 0.6% of specimens tested for anti-cyclic citrullinated peptide have been identified to be falsely reported as positive (12). It should be noted while the prevalence of anti-streptavidin antibodies has been established for the IgG isotype, to the authors' knowledge this is the first report of IgM as the isotype of anti-streptavidin antibodies. Protein A/G methods used to detect interference from endogenous antibodies have weak or no affinity toward human IgM and so may not identify such antibodies (13).
The biotin–streptavidin interaction is widely used in clinical immunoassays due to its specificity, flexibility, and high affinity. Analytical interference caused by biotin is increasingly recognized to affect major platforms, including analyzers from Beckman Coulter, Immunodiagnostic Systems, Vitros, Siemens, as well as Roche (see Piketty et al. (5) for analyzer and assay specific details). Similar to biotin ingestion, interference caused by anti-streptavidin antibodies can affect immunoassays on other platforms (14). This report demonstrates anti-streptavidin antibodies can mimic interference caused by biotin. This differential diagnosis should be included when interference from biotin is considered, especially if the patient denies taking biotin. In these cases, clinical correlation and collaboration with the laboratory are critical in the interpretation of results.
Footnotes
Acknowledgments
We would like to acknowledge Mr. Eric Thorstensen, Liggins Institute, Faculty of Medical and Health Sciences, University of Auckland, for his help with the measurement of serum biotin.
One of the two patients described in this report has been previously presented in an abstract for the 19th European Congress of Endocrinology 2017. A repeat collection of blood was performed for the further characterization of this interference.
Author Disclosure Statement
No conflicts of interests.