
Abstract
Background:
Recurrent laryngeal nerve (RLN) palsy remains a major source of morbidity after thyroid surgeries. Intraoperative neural monitoring (IONM) has gained increasing acceptance as an adjunct to standard practice of visual RLN identification. Endotracheal tube (ETT) surface recording electrodes systems are now widely used for IONM; however, a malpositioned ETT can cause false IONM results and requires time-consuming intraoperative verification of the ETT position and readjustment by the anesthesiologist. The aim of this experimental study was to evaluate the feasibility of the transcutaneous approach for recording evoked laryngeal electromyography (EMG) signals during IONM.
Methods:
A porcine model with well-established applicability in IONM research was used. Twelve piglets (24 nerve sides) were enrolled. Electrically evoked EMGs were recorded from surface electrodes on the ETT and from the adhesive pre-gelled surface electrodes on the anterior neck skin. The evoked EMG waveforms were measured and analyzed. The real-time signal stability of the electrodes during tracheal displacement and their accuracy in reflecting adverse EMG changes during RLN stress were evaluated during continuous IONM performed with automatic periodic vagus nerve (VN) stimulation.
Results:
In all nerves, both the ETT and neck adhesive skin electrodes successfully recorded typical evoked laryngeal EMG waveforms from the RLNs and VNs under stimulation with 1 mA. The transcutaneous electrodes recorded mean EMG amplitudes of 264 μV (±79) under RLN stimulation and 202 μV (±55) under VN stimulation. The electrodes recorded mean EMG latencies of 2.98 ms (±0.20) under RLN stimulation, 4.51 ms (±0.50) under right VN stimulation, and 8.13 ms (±0.94) under left VN stimulation, respectively. When tracheal displacement was experimentally induced, the EMG signals obtained by ETT electrodes varied significantly, but those obtained by transcutaneous electrodes did not. When RLN traction stress was experimentally induced, both ETT and transcutaneous electrodes recorded the same pattern of progressively degrading EMG amplitude with gradual recovery after release of traction.
Conclusions:
This study confirms the feasibility of transcutaneous recording of evoked laryngeal EMG during IONM. Although this study confirms the stability and accuracy of the transcutaneous approach, it also revealed the need for new electrode designs to improve EMG amplitudes before practical clinical application of this approach.
Introduction
R
Currently, IONM during thyroid surgery is almost always performed with a commercially available endotracheal tube (ETT)–based surface recording electrode system, a so-called EMG tube, to record the laryngeal electromyography (EMG) response (3). However, a limitation of the clinical use of EMG tubes is the need to maintain constant contact between the electrodes and vocal cords during surgery to obtain a high-quality recording (3,8 –12). An EMG tube that is malpositioned during intubation (e.g., due to rotation, incorrect insertion depth, or incorrect tube size) or displaced during neck extension or surgical manipulation (e.g., due to rotation or upward/downward displacement) can cause false IONM results (9 –11,13 –16), resulting in the need for intraoperative verification or readjustment of the EMG tube position which is troublesome and time consuming.
During IONM, an EMG tube is used to detect the electrophysiologic activity of the thyroarytenoid muscles, which originate from the inner surface of the thyroid cartilage. We therefore hypothesized that needle or surface recording electrodes on thyroid cartilage or overlying neck skin should function like the EMG tube electrodes and enable access to the electrophysiologic response of the thyroarytenoid muscle and RLN. Theoretically, recording electrodes on the thyroid cartilage or neck skin should also be more stable than those on an EMG tube because the anatomic relationship is unaffected by surgical manipulation. We recently reported the feasibility and stability of needle electrodes used to record EMG on thyroid cartilage (17). However, this recording method has two limitations. First, this recording method requires exposure of the thyroid cartilage, which limits its use in procedures performed without a neck incision or only a small neck skin incision and also limits its use in endoscopic or robotic thyroidectomy. Second, the procedure is not entirely noninvasive, and inserting the needle electrodes may be difficult in elderly patients with calcified thyroid cartilage.
To overcome the limitations of EMG tubes and needle thyroid cartilage recording electrodes, we designed a novel transcutaneous approach in which surface skin electrodes are used for IONM recording. Experiments were performed to evaluate the feasibility, stability, and accuracy of the proposed approach.
Materials and Methods
Animal model and anesthesia
The porcine model used for the experiments in this study is well established in IONM research (18 –21). Male piglets (age, 3–4 months; weight, 20–30 kg) were obtained from the Laboratory Animal Center of Kaohsiung Medical University. The study protocol was approved by the Institutional Animal Care and Use Committee of Kaohsiung Medical University. All experiments were performed in piglets according to institutional guidelines that comply with national and international regulations for animal experiments.
At 8 hours after fasting and 30 minutes before the experiment, each piglet was premedicated with intramuscular azaperone (4 mg/kg). General anesthesia was induced by inhalation of 2–4% sevoflurane via a hollow plastic bottle in prone position. A bolus of propofol 1 mg/kg was administered intravenously with a 24-gauge peripheral intravenous catheter placed on the ear. Each piglet was then intubated with a No. 6 EMG ETT (NIM Standard EMG Tube, Medtronic, Jacksonville, FL) (Fig. 1A). The EMG tube position was confirmed by the anesthesiologist. After fixation of the tube, the piglet was placed in the supine position with the neck extended. Anesthesia was induced with sevoflurane 1–3% in oxygen. The lungs were ventilated in volume-control mode at a tidal volume of 8–12 mL/kg, and the respiratory rate was set to 12–14 breaths/min. Body temperature was maintained with a circulating water mattress maintained at 40°C.
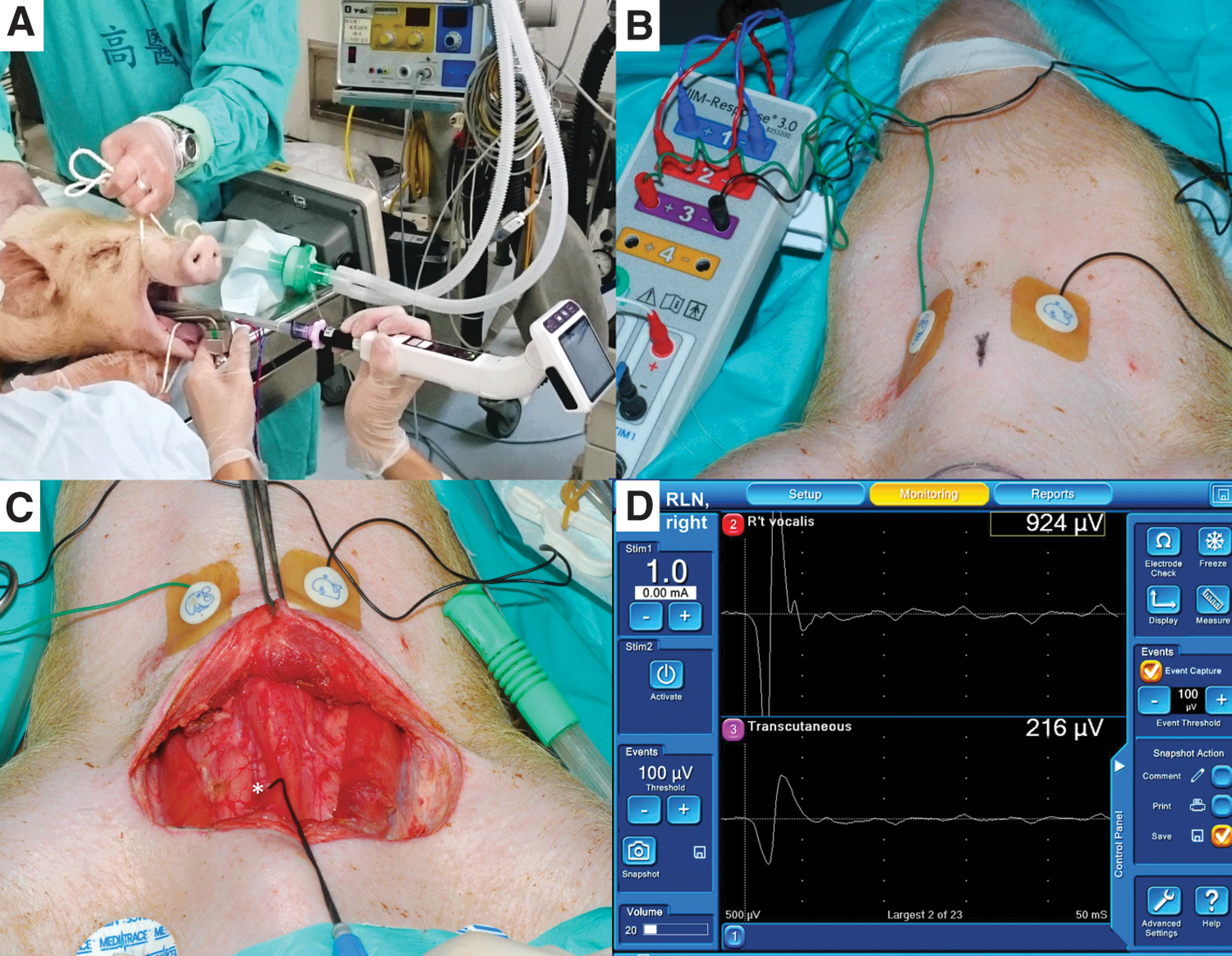
Setup of the endotracheal tube and the transcutaneous surface recording electrodes for intraoperative neuromonitoring in a porcine model. (
Equipment setup, operation, and experimental design
In addition to the EMG tube electrodes (Fig. 1A), another pair of adhesive pre-gelled electrodes (Neotrode II®, ConMed Corporation, Utica, NY) were attached to the neck skin at the upper borders of the left and right lamina of the thyroid cartilage. The channel leads from the EMG tube and neck skin transcutaneous electrodes were connected to the monitoring system (NIM-Response 3.0, Medtronic) (Fig. 1B).
The surgery began with formation of an apron flap. Subplatysmal flaps were raised. Bilateral RLNs and vagus nerves (VNs) were localized, identified, and carefully exposed using a handheld stimulation probe (Ball-tip 1mm, Medtronic) (Fig. 1C). The monitoring system generated stimuli with a time window set to 50 ms and an amplitude scale set to 0.2 mV/division. The pulsed stimuli were 100 μs in duration and 4 Hz in frequency. The event capture was activated at a threshold of 100 μV.
Feasibility study
In each piglet, the bilateral VNs and RLNs were stimulated with a current of 1 mA, and the electrically evoked EMG waveforms recorded from both the EMG tube and the transcutaneous electrodes were displayed on a monitor (Fig. 1D) and were measured for further analysis. In addition to evaluating the feasibility of transcutaneous recording during intermittent IONM (I-IONM) with a handheld stimulation probe, the feasibility during continuous IONM (C-IONM) was also evaluated by using an automatic periodic stimulating electrode (Medtronic) for continuous VN stimulation (Fig. 2A)
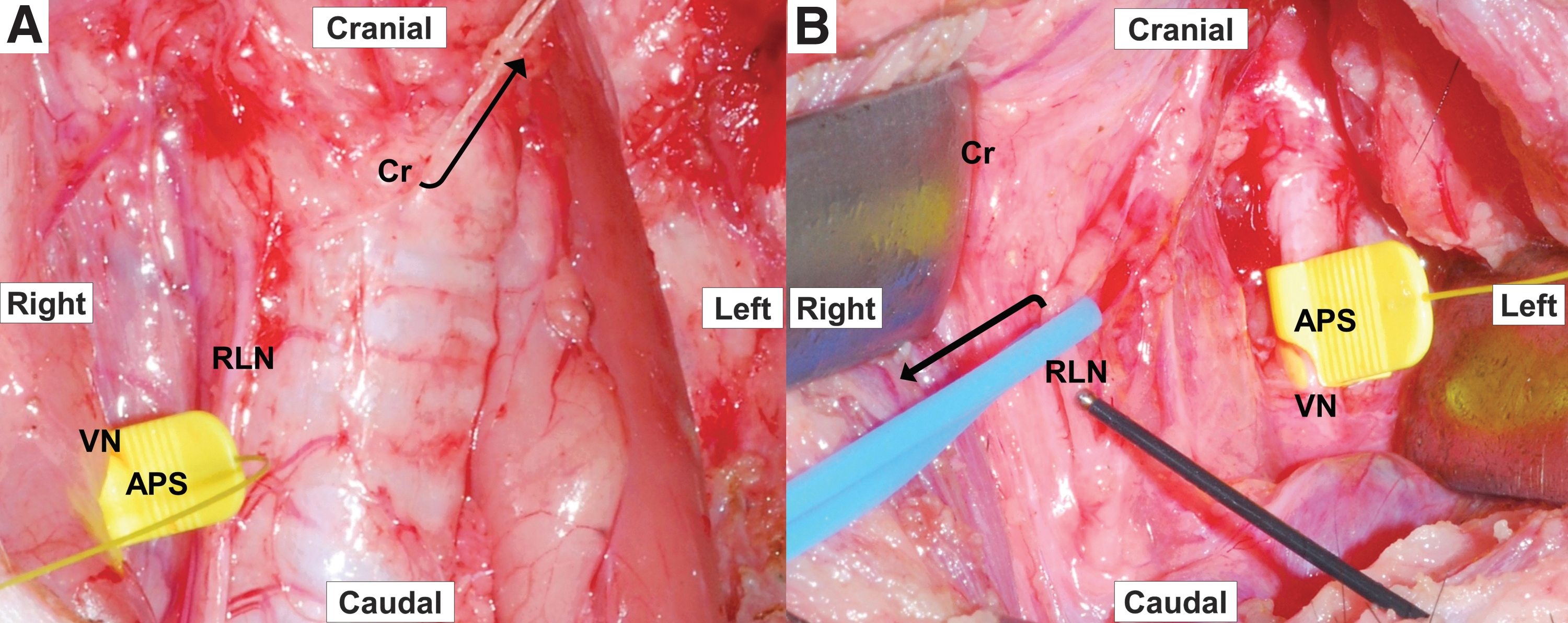
Protocols for feasibility, stability, and accuracy studies. (
Stability study
Baseline electrophysiologic EMG data obtained from both the EMG tube and transcutaneous electrodes were documented. To evaluate and compare the stability of EMG signals during surgical manipulation, upward cricoid displacement was experimentally induced during C-IONM (Fig. 2A) to mimic the effects of thyroid retraction during surgery.
Accuracy study
After the stability study of electrophysiolic EMG data, the accuracy of the electrodes in reflecting adverse changes in EMG signals under RLN stress were further evaluated and compared under experimentally induced RLN traction during C-IONM (Fig. 2B). The RLN traction was experimentally induced to mimic the case of an RLN trapped at the ligament of Berry and the case of an RLN adhered to the goiter capsule and stretched forward during medial traction.
Results
The feasibility analysis included left and right VNs and RLNs in twelve piglets (24 VNs and 24 RLNs). In all animals, both the EMG tube electrodes and the neck adhesive pre-gelled skin electrodes successfully recorded typical evoked laryngeal EMG waveforms during I-IONM and C-IONM (Figs. 1D and 3A–B).
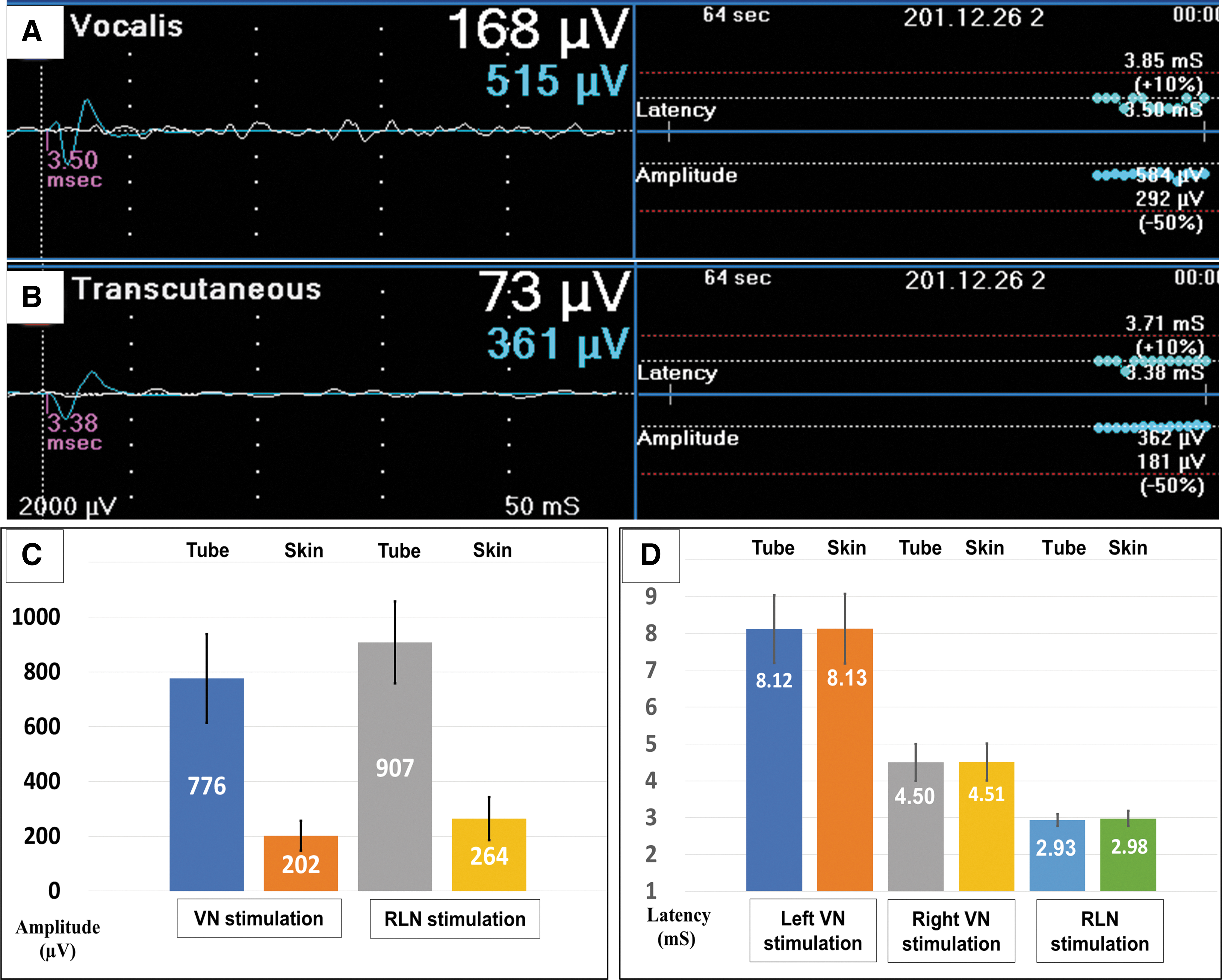
Comparisons of evoked laryngeal EMG responses from the EMG tube electrodes and neck skin electrodes (feasibility study). (
Mean EMG amplitudes recorded under VN stimulation were 776 μV (±161) for EMG tube electrodes and 202 μV (±55) for neck adhesive skin electrodes; mean recorded EMG amplitudes recorded under RLN stimulation were 907 μV (±149) for EMG tube electrodes and 264 μV (±79) for neck skin electrodes. The neck adhesive skin electrodes recorded relatively lower EMG amplitudes compared to EMG tube electrodes (Fig. 3C).
Mean EMG latencies recorded under RLN stimulation were 2.93 ms (±0.16) for EMG tube electrodes and 2.98 ms (±0.20) for neck skin electrodes. Mean EMG latencies recorded under right VN stimulation were 4.50 ms (±0.50) for EMG tube electrodes and 4.51 ms (±0.50) for neck skin electrodes. Mean EMG latencies recorded under left VN stimulation were 8.12 ms (±0.92) for EMG tube electrodes and 8.13 ms (±0.94) for neck skin electrodes. There is no significant difference between the mean EMG latencies in both recording electrodes (Fig. 3D).
This stability study evaluated the real-time stability of the signal obtained during tracheal displacement under C-IONM in four animals. All real-time EMG tracings showed that the experimentally induced upward displacement of the cricoid caused significant variations in the EMG signals obtained by the ETT electrodes (Fig. 4A). However, the displacement did not significantly affect the EMG signals obtained by the transcutaneous electrodes (Fig. 4B).
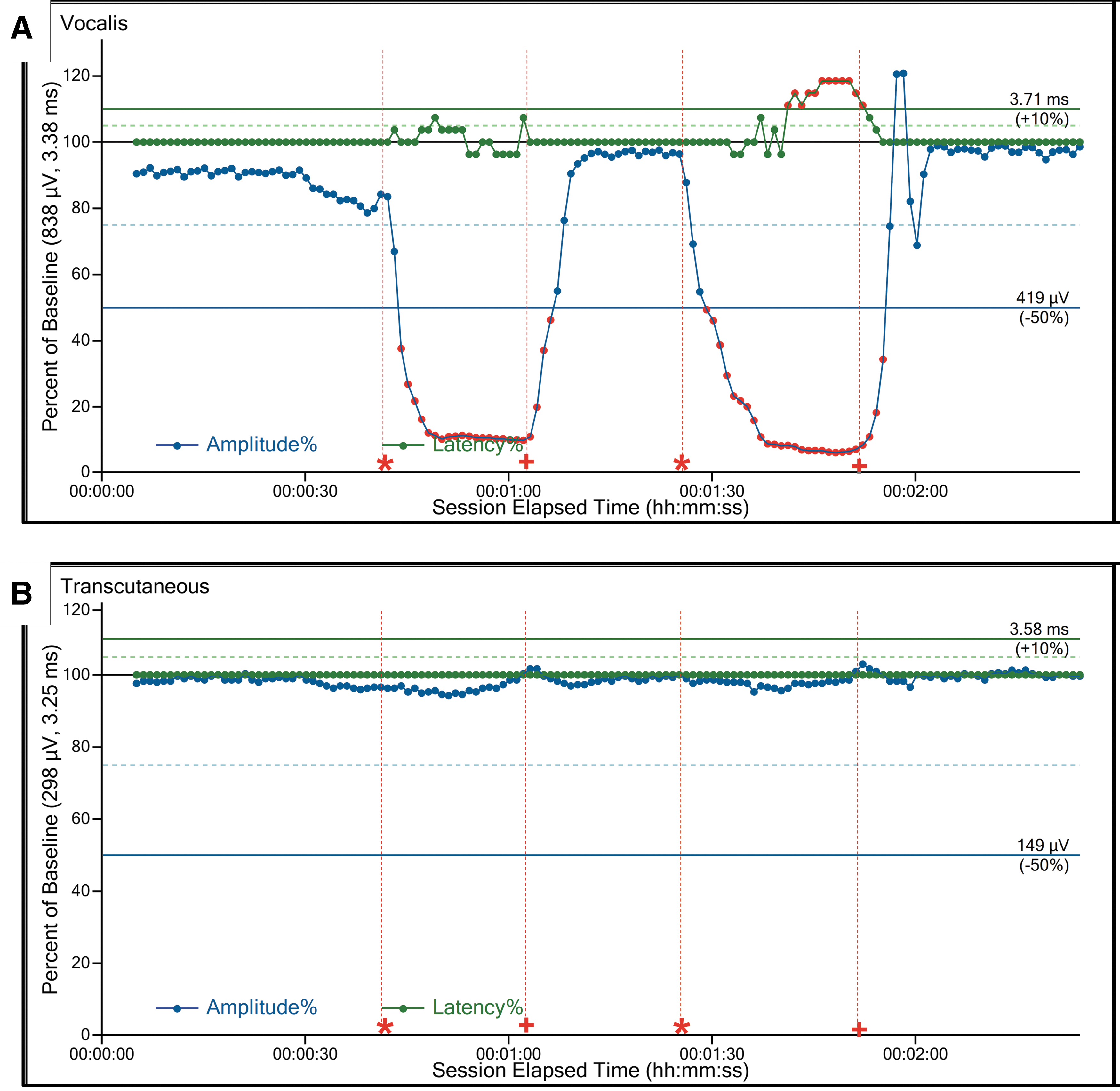
Comparison of real-time changes in electromyography (EMG) signals detected by EMG tube electrodes on the vocalis muscle and by transcutaneous electrodes on the neck skin when tracheal displacement was experimentally induced (Stability study). (
The accuracy study investigated whether real-time signals obtained under C-IONM accurately reflect the EMG signal degradation caused by RLN stress. Real-time EMG tracings obtained under RLN traction stress induced in all four experimental animals showed that both ETT and transcutaneous electrodes recorded the same pattern of progressively degrading EMG amplitude with gradual recovery after termination of traction (Fig. 5A and B).
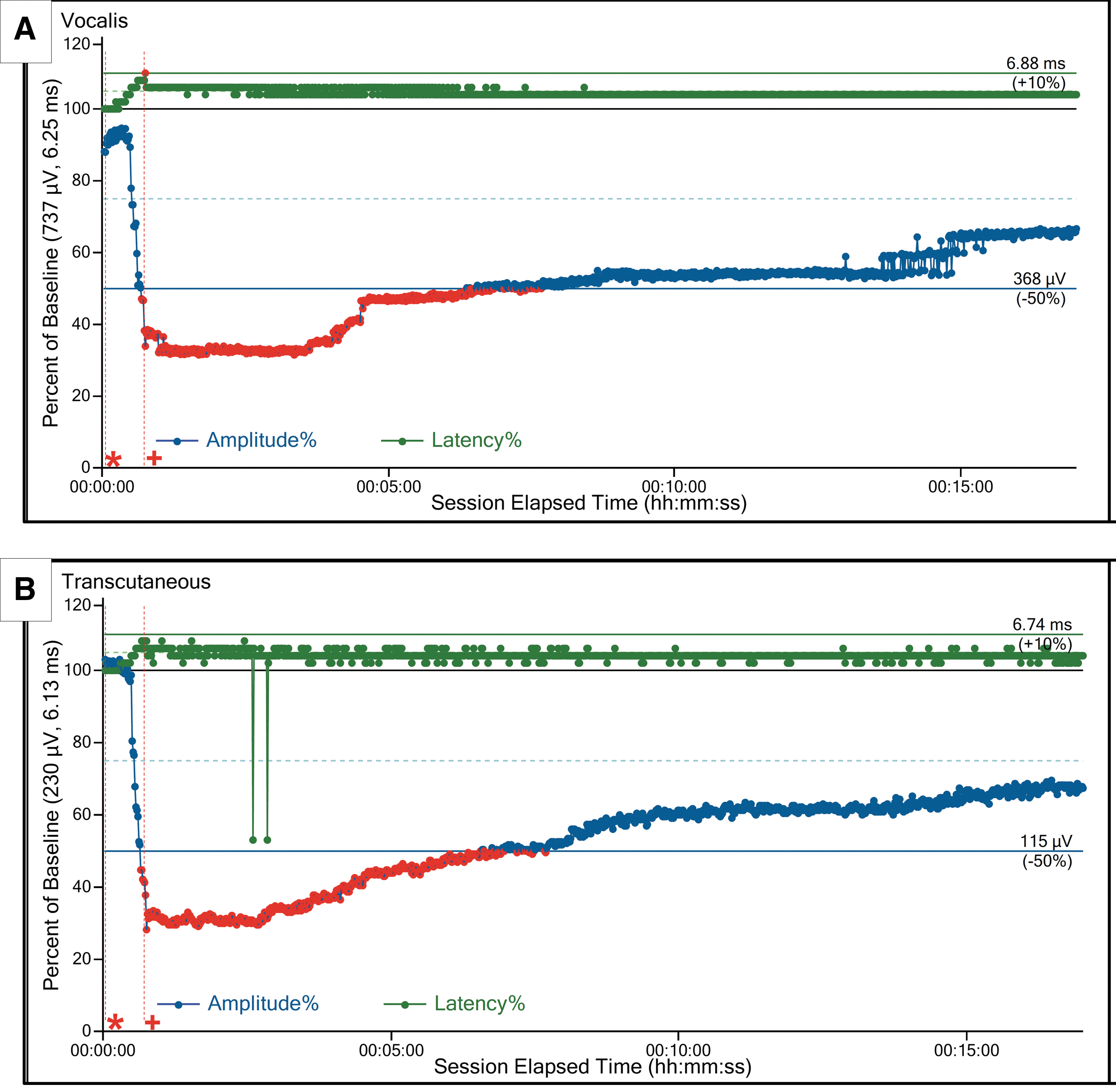
Comparison of real-time changes in electromyography (EMG) signals detected by EMG tube electrodes on the vocalis muscle and by transcutaneous electrodes on the neck skin when recurent laryngeal nerve traction stress was experimentally induced (Accuracy study). The (
Discussion
In this study, a porcine model with well-established applicability in IONM research (18 –21) was used to evaluate the feasibility, stability, and accuracy of a transcutaneous approach to recording evoked laryngeal EMG during IONM (Figs. 1 and 2). The experiments confirmed that the transcutaneous approach is feasible for recording typical evoked laryngeal EMG responses under stimulation of the VN or RLN (Fig. 3). The experiments also showed that the transcutaneous approach is stable during tracheal displacement (Fig. 4B) and accurately depicts RLN stress (Fig. 5B). Although the transcutaneous electrodes used in this study recorded relatively lower EMG amplitudes compared to conventional EMG tube electrodes, the experiments showed that this novel approach has potential applications in future designs of recording electrodes for use during IONM.
RLN injury remains a major cause of morbidity after thyroid surgery and is a leading cause of medicolegal litigation (22). One major change in thyroid surgery in the past decade is the widespread use of IONM to identify the RLN adjunct to the standard practice of visual identification. Organizational support for IONM is gradually increasing (2 –7). In recent years, the use of EMG tubes in IONM has rapidly increased due their low invasiveness and wide commercial availability (3). For accurate monitoring, the EMG tube used for recording during IONM must be the appropriate size and must be correctly aligned (10,12). However, determining the proper EMG tube size for each patient can be difficult, and there is no commercial available small size EMG tube for pediatric patients. The current guideline is to use the largest possible EMG tube to optimize electrode contact with the vocal cords. However, a large tube also increases the risk of intubation problems and vocal cord trauma (3). Another problem is that EMG tube movement and changes in the contact with vocal cords often occur during neck extension and surgical manipulation (10). This problem likely explains why studies of EMG tube-based IONM systems often report a high negative predictive value of 92–100% but a low and highly variable positive predictive value of 10–90% (23).
Our experience in this study shows that, in contrast with the troublesome and time-consuming procedures required to adjust EMG tube electrodes and verify their proper position, the setup procedure for transcutaneous electrodes can be performed quickly and easily. The setup time was less than 1 minute in all experiments, and the correct electrode locations could be confirmed by direct visualization at all times (Fig. 1). Compared to EMG tube electrodes and intramuscular or intracartilage needle electrodes, transcutaneous adhesive electrodes are less invasive and do not leave mucosa trauma or needle tracts in the skin, cartilage, or muscles. Transcutaneous electrodes are also easier to use because they do not require adjustment of the EMG tube by the anesthesiologist. In cases of unmonitored thyroidectomy with intraoperative RLN difficult identification or uncertainly anatomic variations, surgeons can easily set-up the transcutaneous IONM intraoperatively. Finally, transcutaneous electrodes seem to be more cost effective. For example, an NIM EMG tube and a paired needle electrode can be purchased locally (i.e., in Taiwan) for the equivalent of 700 USD and 300 USD, respectively, whereas a pair of adhesive pre-gelled electrodes can be purchased for the equivalent of only 5 USD.
This in vivo porcine study has several limitations. First, this study used an animal model with a moderate sample size. Although this model has proven useful and effective for evaluating electrophysiologic correlates of EMG during IONM in previous studies (18 –20) and also showed good reproducibility between animals and all RLN or VN sides in the current study, further studies in human subjects are needed. Second, the adhesive pre-gelled surface electrodes may be dislodged during surgical manipulations such as retraction of the skin or application of traction on the thyroid, and they may not be useful in procedures that require a large incision or involve a large tumor size. To avoid displacement, the electrode must be positioned in the more cranial position (i.e., at the upper borders of the thyroid cartilage used in the experiments in this study; Fig. 1B–C) and must be securely affixed to the skin surface (i.e., by covering the electrode with a transparent membrane such as Tegaderm or OPSITE film). Additionally, excessive skin flap dissection or retraction must be avoided during surgery. The effectiveness of this strategy needs further evaluation in animal and clinical studies.
Third, the EMG amplitudes recorded with neck skin electrodes was much lower than that recorded with EMG tube electrodes (Fig. 3C). Although this study confirms the accuracy of transcutaneous electrodes for detecting neurophysiologic events, their relatively low mean amplitude may still preclude early detection of RLN traction stress, which is essential for preventing injury during IONM. Therefore, different electrode materials and different transduction mechanisms of electrodes need further study to improve the EMG amplitudes obtained in clinical practice.
Notably, the amplitude results can be substantially improved by using electrodes that are designed to be affixed to the thyroid cartilage with a pin or needle (17). However, using such an electrode increases the invasiveness of the procedure. Another possibility is using an “electronic skin” (e-skin) to improve the amplitude results. For example, in the e-skin developed by Kim et al., various serpentine sensors are embedded in a highly stretchable net sandwiched between two protective layers of equal thickness (24). The resulting device has a compact size and can be attached to the skin like a bandage to acquire physiological information without bulky electrodes (24). The device can be used without adhesives, gels, or even wires and has strong potential as a future direction of EMG recording during IONM. However, using an electrode with an e-skin design in IONM could be more expensive than using a conventional EMG tube electrode. Since this technologically advanced design is expensive and complex and is not yet commercially available, the e-skin design was not tested in the current study. Therefore, a remaining challenge in the practical application of transcutaneous IONM is development of transcutaneous surface electrodes that provide a desirable combination of high sensitivity, noninvasiveness, and cost effectiveness.
Various remote access techniques proposed for use in endoscopic and robotic thyroidectomy in the past two decades have demonstrated superior cosmetic outcomes compared to open surgery (25 –28). In a review of studies of endoscopic and robotic thyroidectomy, Dionigi et al. (29) found that IONM was used in only 5% (9 of 160 studies). Possible explanations for the low use of IONM in both endoscopic and robotic thyroidectomy include technological limitations and interference with endoscope monitoring devices (29). Recently, Zhang et al. (30) reported the feasibility and advantages of using percutaneous probe stimulation for IONM during endoscopic thyroidectomy performed with a narrow operating space. Now that our current study has confirmed the feasibility of transcutaneous recording during IONM, our future studies will further investigate the feasibility of a totally transcutaneous approach to stimulation and recording in IONM. A transcutaneous approach would be highly applicable when IONM is used in endoscopic or robotic thyroidectomy or in procedures performed with a small incision or without an incision (e.g., ultrasound-guided laser or radiofrequency ablation).
In conclusion, this study demonstrates the feasibility of a transcutaneous approach to recording evoked laryngeal EMG during IONM. Although the stability and accuracy of the transcutaneous approach were also confirmed, further research is needed to increase the EMG amplitude before practical clinical application of the approach.
Footnotes
Acknowledgments
This paper received the third place award for Best Oral Presentation at the Third World Congress on Thyroid Cancer, July 27–30, 2017, in Boston. The authors gratefully acknowledge the technical assistance provided by Hui-Chun Chen (clinical nurse specialist, Department of Nursing, Kaohsiung Medical University Hospita [KMUH], Kaohsiung Medical University [KMU]), Hsiu-Ya Chen (nurse anesthetist, Department of Anesthesiology, KMUH, KMU). This study was supported by grants from the Kaohsiung Medical University (KMU-TP105E23; KMUH106-6R49) and the Ministry of Science and Technology, Taiwan (MOST 105-2314-B-037-010, 106-2314-B-037-042-MY2).
Author Disclosure Statement
The authors have no conflict of interests to declare.