
Abstract
Background:
Levothyroxine (LT4) is one of the most prescribed drugs worldwide. Once started, approximately 90% of patients continue treatment long term. However, accumulating evidence suggests that many patients, for whom the indication for its administration is not adequately established and the diagnosis is not well documented, are overusing it. This study aimed to evaluate the necessity for and determine potential prognostic factors of long-term LT4 supplementation.
Methods:
A prospective clinical cohort follow-up study was carried out. In 291 subjects (84% females) aged 48 ± 16 years on LT4 replacement therapy without a solid diagnosis of hypothyroidism being provided, the treatment was paused. At the beginning and after six to eight weeks of treatment discontinuation, thyrotropin (TSH) and free thyroxine levels were assessed, and thyroid ultrasound was performed. A TSH value of ≥4.5 IU/mL was considered as underlying hypothyroidism.
Results:
Among the 291 individuals, 114 became hypothyroid (group A), while 177 subjects remained euthyroid off LT4 (group B; 39.2% vs. 60.8%, p < 0.001). The groups were comparable regarding sex, family history, age, body mass index, duration of treatment, basal TSH and free thyroxine values, thyroid volume, and presence of thyroid autoantibodies. However, diffuse inhomogeneous echogenicity on ultrasound examination was significantly higher (p < 0.001) in group A.
Conclusions:
These findings suggest considerable overuse of thyroxine therapy. The results underline the initial need to establish the diagnosis firmly before treatment initiation and to undertake periodic evaluation of all patients on chronic LT4 treatment as to the necessity for treatment continuation. In all patients on long-term LT4 therapy in whom the diagnosis has not been definitively established, it appears rational to introduce a six- to eight-week period of LT4 replacement therapy discontinuation, preceded and followed by TSH tests, as the first-line approach—a procedure that could be implemented as part of a common strategy among the scientific community to decrease current LT4 overuse.
Introduction
I
LT4 administration has been steadily rising worldwide over the last decade (1). Indeed, the number of LT4 prescriptions increased significantly from 2007 to 2014, making LT4 the most prescribed drug in the United States and the third most prescribed drug in the United Kingdom, although the incidence of overt (0.2–2%) and subclinical hypothyroidism (up to 12%) remained relatively stable in those countries (2,3). Meanwhile, the ongoing variations in recommendations for thyroid TFTs and thyroid nodule management further contribute to clinician uncertainty (4). International guidelines, although inconsistent between different societies, generally indicate LT4 prescription for people with subclinical hypothyroidism who have a thyrotropin (TSH) concentration of ≥10 IU/mL and for those with abnormal TSH concentrations but <10 IU/mL who may complain of hypothyroid-like symptoms or display positive autoantibodies or suffer from dyslipidemia, diabetes mellitus, arterial hypertension, or cardiovascular disease (5,6). However, there is a shift today toward lower TSH values as cutoff points, and in Europe, a TSH value >4.5 IU/mL, particularly in young patients with the abovementioned parameters, usually prompts initiation of therapy (7).
One probable reason for overdiagnosis might be the well known fact that “hypothyroidism symptoms” are not specific but vague, and signs such as dry skin, hair loss, myalgia, fatigue, menstrual irregularities, and weight gain are signs and symptoms of an array of different medical conditions. Furthermore, these same signs could be part of the normal spectrum of findings occurring due to the stress of everyday living, such as nervous tension, fatigue, unhealthy eating behaviors, or loss of sleep (8). In fact, even the 20–25% of people with TSH values within the reference range report one or two of the above symptoms (2,7). Additionally, the nonspecific nature of many signs and symptoms of primary hypothyroidism make it difficult to rely on history and physical examination to determine which individuals would benefit from determining TFTs. There are indeed physicians who treat hypothyroidism based on symptoms alone or who add triiodothyronine for persistent nonspecific symptoms, even though there is no evidence to support this approach. For the above reasons, it is estimated that approximately 25% of the British adult population are required by their attending physicians to have their TFTs determined every year (9).
As mentioned above, in numerous cases, patients have been started on LT4 administration without a solid diagnosis of hypothyroidism. This inappropriate diagnosis can initiate a sequence of therapeutic misadventures. For instance, in a population-based study, it was found that 62% of patients with spontaneously elevated TSH concentrations have normal levels if measurements are repeated, implying that TSH levels could be affected by several factors such as illness, drugs, other environmental factors, or assay interference (10). Consequently, variability in TSH levels might lead to misdiagnosis. Lastly, it should be mentioned that most guidelines and experts recommend that TSH values, age-adjusted for normal reference ranges, need to be confirmed twice as abnormal and that at different ages different cutoff values could be implied before LT4 is initiated (11,12).
Taking these aspects surrounding diagnosis and treatment into account, and considering the recent findings arguing against the treatment of older adults for subclinical hypothyroidism (13), this study addressed the question of whether LT4 treatment is necessary in all patients treated, including young and older individuals, hypothesizing that numerous individuals on LT4 replacement therapy may no longer require it. Therefore, the study evaluated whether patients on LT4 replacement therapy maintain normal TFTs after therapy discontinuation lasting at least six to eight weeks. In addition, the study sought to determine the potential prognostic factors necessary to discriminate which patients would most benefit from this approach.
Methods
Study design and participants
This was a prospective clinical study including 291 individuals (84% females) aged 48 ± 16 years under LT4 supplementation therapy for at least one year. The cohort consisted of Caucasian patients of Greek origin who consecutively visited the Endocrine Outpatient Clinic of the Metropolitan Hospital, Athens, Greece, between January 2015 and December 2016. All records are based on the International Classification of Diseases (ICD-10) code. Only patients with normal TSH levels (0.4–4.5 IU/mL) and normal free thyroxine (fT4) levels (0.58–1.60 ng/dL), according to the institutional reference ranges, were evaluated with the aim of including only those individuals who attained biochemical euthyroidism. As a result, patients who had suppressed TSH levels, because of either a nodule suppression therapy or overuse at baseline, were excluded from the study. Additionally, patients with goiter, with a history of total or partial thyroidectomy, and on thyroid-altering medication (e.g., lithium, corticosteroids), and women wishing to conceive or who had given birth in the previous year were excluded. The diagnosis of hypothyroidism was considered as solidly established when the patient provided at least two laboratory tests with elevated TSH values within a three- to six-month interval. All individuals included in the study were receiving a sufficient dose for their body weight (0.92 ± 0.42 μg/kg/day) (14).
Treatment was discontinued in all patients meeting the above criteria, and serum TSH and fT4 concentrations were measured before and following six to eight weeks of treatment discontinuation. Body mass index (BMI), family history of thyroid diseases, years of supplementation therapy, and LT4 dose (μg/kg/day) were assessed. The study also tested for thyroid autoantibodies and determined thyroid volume and the echogenicity of thyroid parenchyma by ultrasound (US).
Patients were assigned to the following subcategories: (i) presence of thyroid nodules but not on suppression therapy (n = 96; S1); (ii) unknown reason for LT4 supplementation, including cases where the treatment was started in the past and there was no evidence of past thyroid dysfunction provided (n = 78; S2); (iii) therapy initiated post pregnancy and practically no reassessment of the need having been provided (n = 15; S3); and (iv) Hashimoto's or hypothyroidism-like or related symptoms (n = 102; S4). LT4 replacement therapy was discontinued for six to eight weeks in all patients, this amount of time constituting a safe period for elimination of circulating LT4 levels and for assessment of thyroid function, given that T4 formulations have a half-life of seven days. Thyroid function was evaluated with serum TSH and fT4 measurements before and after the discontinuation. A thyroid US was also performed on all subjects. Finally, the participants were alerted to potential symptoms of hypothyroidism. Monitoring and follow-up was continued in all subjects after the appropriate intervals. Euthyroidism with LT4 supplementation or after the pause was defined as a TSH level between 0.4 and 4.5 IU/mL. A TSH value of ≥4.5 IU/mL and/or fT4 below normal values after treatment discontinuation was considered as underlying hypothyroidism, and thyroxine supplementation was reinstituted in those individuals. It should be noted that Greece is considered an iodine-sufficient country (15).
Anthropometric evaluation
All individuals underwent standard anthropometric evaluation, including height and weight. Body height was measured to the nearest 0.1 cm using a portable stadiometer (Soehnle Personenmessgerät; Soehnle Industrial Solutions, Backnang, Germany), and weight was measured to the nearest 0.1 kg with electronic scales (Soehnle S20; Soehnle Industrial Solutions). BMI was calculated by taking the ratio of weight (in kilograms) to height (in meters) squared.
Assays
Serum TSH (Dimension Vista; Siemens Healthcare Diagnostics, Eschborn, Germany) and fT4 (Abbott, Architect i2000; Abbott Laboratories Diagnostics Division, Chicago, IL) levels were determined through immunochemiluminescent procedures. The analytical sensitivity of the TSH assay was 0.005 IU/mL, and the TSH working range was 0.005–100 IU/mL. The interassay coefficients of variations (CV) were 2.04% (low) or 2.20% (high) for TSH. Chemiluminescent competitive immunoassays (Advia Centaur XP; Siemens, Tarrytown, NY) were used to measure antithyroglobulin antibodies (anti-TgAb) and antithyroperoxidase antibodies (anti-TPOAb). The lower and upper limits were: fT4, 0.58–1.60 ng/dL; anti-TgAb, 0–60 IU/mL, and anti-TPOAb, 0–57 IU/mL.
Thyroid US
Thyroid US was performed with a high-resolution US machine (EUB 7000; Hitachi, Tokyo, Japan) equipped with a 6–14 MHz linear transducer. Only one operator performed all the measurements. The craniocaudal, transverse, and anterior–posterior dimensions of each lobe were measured. By multiplying these values by each other and then by 0.52, the volume of each thyroidal lobe was obtained. The sum of the volumes of the two lobes provided the volume of the entire thyroid gland. The hypoechogenic signal with a non-homogeneous structure was evaluated as US heterogeneity. Goiter was defined as a thyroid volume >18 mL in women and >25 mL in men (16).
Ethics
The study protocol followed the ethical principles outlined by the Declaration of Helsinki. The Metropolitan Hospital Ethics Review Board approved the study protocol. Written informed consent was obtained from all participants.
Statistical analysis
Data processing was done with IBM SPSS Statistics for Window v21 (IBM Corp., Armonk, NY). Data are shown as the mean ± standard deviation. All continuous variables (age, BMI, duration of therapy, TSH, fT4, total thyroid volume, and LT4 dose) showed normal distribution, as documented by the use of the Kolmogorov–Smirnov test. Comparison of characteristics between groups was performed using the t-test for quantitative variables and the chi-square test for the categorical variables (sex, family history, antithyroid antibodies, and heterogeneity in US). A two-sided p-value of <0.05 was set as the significance level in all analyses.
Results
The study population was comprised of 291 individuals (84% females), 63% of whom had a positive family history for thyroid diseases. The mean age and BMI of the studied subjects were 48 ± 16.43 years and 25.22 ± 4.42 kg/m2, respectively. The duration of treatment ranged from 1 to 37 years (M = 8.06 years). The mean TSH value was 1.55 ± 0.8 IU/mL and the mean fT4 value was 1.15 ± 0.34 ng/dL. Positive antithyroid antibodies were detected in 58% of subjects. Thyroid heterogeneity was detected by US in 62% of the studied subjects.
In 114 (39.2%) of the 291 individuals (p < 0.001), underlying hypothyroidism was found (group A), whereas the rest (group B) remained euthyroid off LT4 administration. Between the two groups, there were no statistically significant differences concerning sex, family history of thyroid dysfunction, age, BMI, years of treatment, basal TSH and fT4 values, LT4, dose, thyroid volume, and positivity of thyroid autoantibodies (Table 1). Diffuse inhomogeneous echogenicity was significantly higher in group A (Fig. 1).
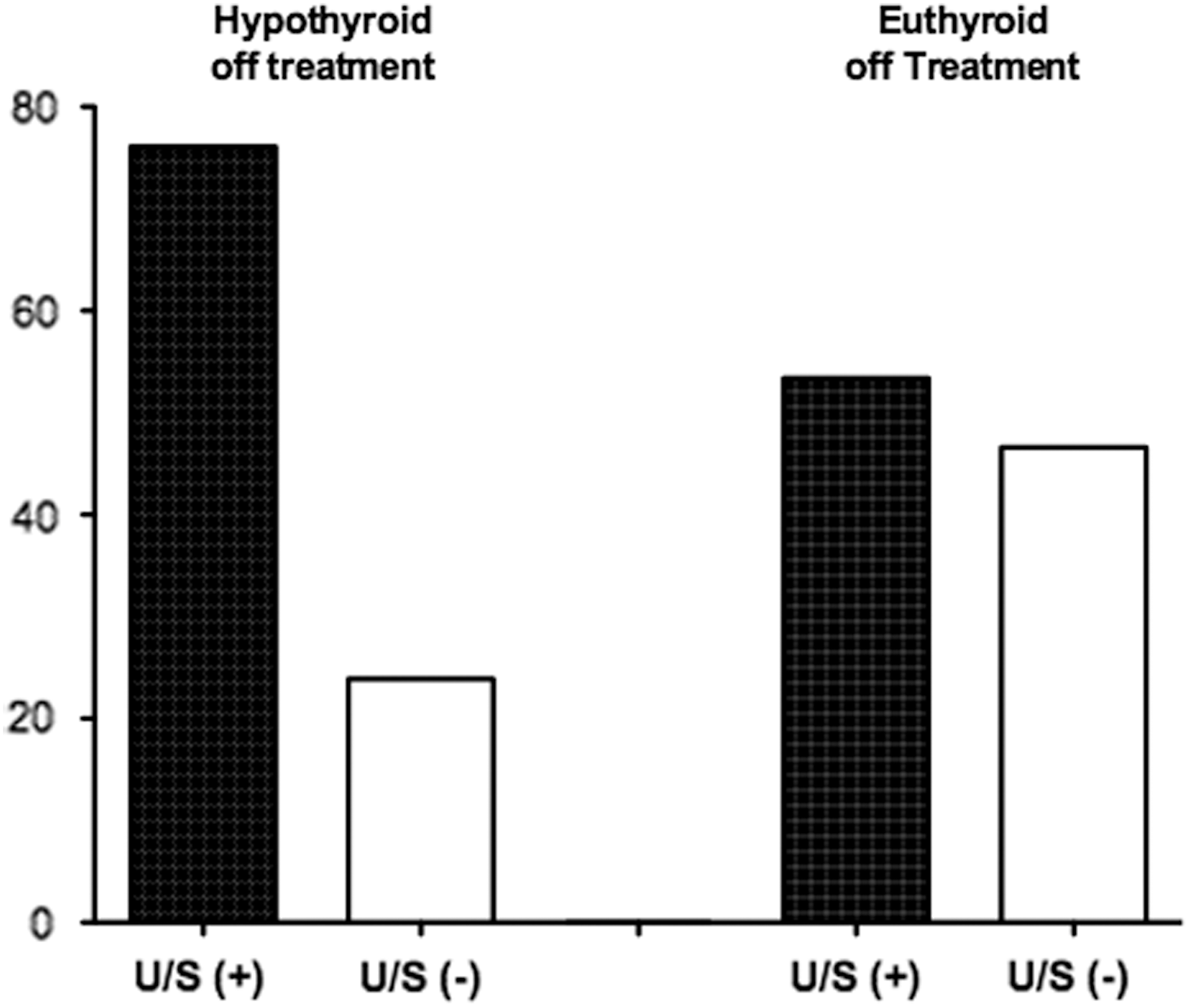
The presence of inhomogeneous echogenicity (black bar) in patients who became hypothyroid off treatment.
Pertinent Characteristics of the Study Group According to Response on Treatment Discontinuation
Data of quantitative and categorical variables are presented as M ± SD and in %, respectively.
BMI, body mass index; TSH, thyrotropin; fT4, free thyroxine; LT4, levothyroxine; SD, standard deviation.
All patients were thoroughly and extensively questioned about any change regarding their quality of life before and after LT4 discontinuation, though no specific questionnaire was administered to them. The majority of them reported “feeling better,” and no significant adverse events were mentioned by any subject.
The mean pre-withdrawal TSH values among group A (1.58 ± 0.84 IU/mL) and group B (1.51 ± 0.32 IU/mL) were comparable. However, the corresponding numbers differed significantly after LT4 discontinuation (8.21 ± 2.35 vs. 2.42 ± 1.32 IU/mL, p < 0.05), that is, 26% of subjects in group A displayed TSH values >10 IU/mL.
In terms of anthropometric changes, nonsignificant differences were observed between those who became hypothyroid compared to those who remained euthyroid off LT4. Specifically, weight gain in group A was 2% vs. 1.2% in Group B (p = n.s.). A similar pattern was observed in systolic (132 ± 7.4 vs. 124 ± 8.4 mmHg, p = n.s.) and diastolic blood pressure values (88 ± 12 vs. 91 ± 9.1 mmHg, p = n.s.).
By using cutoff TSH values >7.5 IU/mL in those subjects >65 years of age, it was noted that the percentage of subjects who remained euthyroid off LT4 rose to 75% compared to 25% in those who needed LT4 reinstitution.
When the above data were stratified according to the reason for treatment initiation, it was found that in 53.8% of the patients who could not provide clarification of the reason for LT4 treatment (S2), underlying hypothyroidism was revealed within the study period. Conversely, the percentage of subjects with underlying hypothyroidism was lower in the other subgroups. Specifically, it was 36.5% in the nodule group (S1), 32.4% in the Hashimoto's group (S4), and 26.7% in those patients who continued the treatment after pregnancy (S3; Fig. 2).

Incidence of hypothyroidism stratified according to the etiology patients reported for treatment initiation.
In order to define the prognostic value of the different factors further among these subcategories according to the reason for treatment, the data were further split according to the latter. The findings are summarized in Table 2. Since 10% of subjects were prescribed LT4 at a dose of ≤50 μg/day, the percentage of subjects with underlying hypothyroidism was analyzed in this subgroup. However, it was comparable to the total group (36% hypothyroid and 64% remained euthyroid off LT4 treatment).
Potential Prognostic Factors for Hypothyroidism Evident after LT4 Withdrawal Among Subgroups
S1, history of thyroid nodules but not on suppression therapy (n = 96); S2, unknown reason for LT4 supplementation, including cases where the treatment was started in the past and there was no evidence of past thyroid dysfunction provided (n = 78); S3, therapy initiated post pregnancy and practically no reassessment of the need having been provided (n = 15); S4, Hashimoto's or hypothyroidism-like or related symptoms (n = 102).
Discussion
The aim of this study was to investigate a common clinical scenario: the management of patients with normal TFTs receiving LT4 therapy for several years in the absence of a solid diagnosis of hypothyroidism, the latter denoting those cases where the primary reason for LT4 supplementation is not further substantiated according to current guidelines, or cases for whom medical records and the patient's history are incomplete. Accordingly, in a cohort of 291 subjects consecutively evaluated, it was found that only 39% required thyroxine treatment. Remarkably, from the prognostic factors evaluated, only the existence of inhomogeneous echogenicity on thyroid US was significantly associated with underlying hypothyroidism (p < 0.001; Fig. 1), whereas other factors such as sex, age, BMI, family history, years on treatment, thyroid volume, and positivity of thyroid autoantibodies did not differ between the two groups (Table 1). Interestingly, when patients were stratified according to the reported diagnosis on the basis of which LT4 was initiated, an underlying hypothyroidism rate of about 30% was noted in the subgroups who reported suffering from nodules (36.5%), Hashimoto's disease (32.4%) and post-pregnancy hypothyroidism (26.7%). Intriguingly, 53.8% of those subjects who could not state the reason for their initial LT4 therapy needed the treatment (Fig. 2).
The finding that only 39% of evaluated subjects required reinstitution of therapy because of documented underlying hypothyroidism is surprising and unveils the presence of a considerable burden on patients' health and finances. First, LT4 treatment, once started, currently constitutes a long-term treatment in about 90% of patients. This affects the life of patients who need to modify their daily routine accordingly. For example, taking LT4 before a meal and waiting until breakfast or the intake of other drugs requires a disease-based plan on a daily basis. It should also be borne in mind that patients treated for hypothyroidism have reduced quality of life compared to their healthy peers (17). Besides, LT4 is not infrequently administered to patients with comorbidities, a population typically characterized by polypharmacy, in whom the attending physician must make a judicious choice over which medications are really needed (18). Moreover, the use of an increasing number of drugs is directly related to reduced compliance, which is one of the most important issues concerning drug efficacy in chronic diseases (19). Lastly, it is crucial to remember that labeling a patient as having a chronic disease is associated with an increased risk of anxiety that can further worsen quality of life (20).
At the other end of the scale, there is the so-called clinical inertia phenomenon: some physicians, having prescribed long-term medication to their patients (i.e., the same dose of LT4 for years), omit to reevaluate the appropriate dose, thereby failing to modify their patients' therapy, which can result in adverse consequences (21). Furthermore, recent data indicate that in clinical practice, in the vast majority of patients, thyroid function evaluation is carried out outside recommended intervals with high within-practice variability (22). Finally, economically speaking, overuse, which involves not only drug and dose adjustment costs but additionally thyroid testing and clinical follow-up, increases outlay for patients and/or insurance companies and unnecessary use of healthcare resources (23).
As far as LT4 overuse is concerned, a very important issue is safety, particularly in older adults. Somwaru et al. showed that among 339 LT4 users aged ≥65 years, only 43% were in the euthyroid range, while 41% had a low TSH (24). Overtreatment at these ages is associated with an increased risk of detrimental skeletal effects such as fractures and adverse cardiovascular effects including atrial fibrillation (25 –28). Moreover, no particular improvement in quality of life was observed in older adults with slightly elevated TSH values (6.40 ± 2.01 IU/mL) treated for one year with LT4 (13).
Concerning initial TSH values as an indication for LT4 initiation, the clinician should be very cautious. Indeed, in the above-mentioned study, it was found that 60% of subjects with a sporadic TSH elevation were found to have normal TFTs at subsequent testing (13). These observations are consistent with other studies showing that a high percentage of subjects with elevated TSH values revert to biochemical euthyroidism during follow-up (29 –31). Analogous findings have been observed in younger subjects. Recently, Radetti et al. reported that not all children suffering from Hashimoto's thyroiditis need lifelong therapy with LT4 and suggested a possible discontinuation of treatment in patients with a TSH level <10 IU/mL at the time of diagnosis (32). These findings could be explained by the natural history of subclinical hypothyroidism, taking into consideration that in different studies previously elevated TSH levels were normalized in all age groups (33 –35).
Regarding prognostic factors, only inhomogeneous echogenicity on thyroid US was associated with underlying hypothyroidism. This finding may be explained as being a result of chronic thyroiditis. Although thyroid volume was comparable between the two groups, thyroid function seems to be compromised in those subjects with inhomogeneous echogenicity. The fact that thyroid autoantibodies were not associated with increased rate of hypothyroidism may be due to the fluctuating levels of autoantibodies over time and the natural history of Hashimoto's disease, where 25% of patients who are hypothyroid may spontaneously return to normal function over the course of several years. It has been hypothesized that this phenomenon is a result of the initial effect of high titers of thyroid-stimulation blocking antibodies, which may fall with time and allow normal thyroid function to return (36,37).
Based on subgroup analysis, a reasonable approach is to withdraw LT4 administration in those subjects reporting nodules, post-pregnancy hypothyroidism, or Hashimoto's disease, since the rate of underlying hypothyroidism is low (∼30%). Evaluation based on the combination of US findings and subgroup analysis seems a very safe approach for treatment discontinuation in those subjects reporting nodules with a negative US. On the other hand, in the presence of a positive US finding consistent with underlying thyroiditis, the decision to continue treatment or not should be taken based on TFTs and the general condition of the patient.
Another important issue impacting LT4 administration is the application of age-specific cutoff values for the diagnosis of hypothyroidism in older adults. Indeed, there is a significant amount of evidence supporting this approach (36), which again is more patient specific. For practical reasons, in the current study, a TSH cutoff value of 4.5 IU/mL was universally applied. However, by using cutoff TSH values >7.5 IU/mL in those subjects >65 years of age, it was observed that the percentage of subjects who remained euthyroid off LT4 rose to 75% compared to 25% in those who needed LT4 reinstitution. This finding strongly suggests that a more discerning approach should be adopted in the case of LT4 administration in older adults.
The findings suggest that there is a need for a personalized approach for LT4 supplementation. Furthermore, in the light of recent findings arguing against the treatment of subclinical hypothyroidism in older patients, it is likely that some older patients on LT4 replacement should be reevaluated. A suggested strategy in the case of a borderline elevated TSH value and/or unclear hypothyroidism-like symptoms is to establish a diagnosis of hypothyroidism only if the above findings are corroborated by repeatedly abnormal elevated TSH levels after an interval of two to four months. If they are still abnormal, then a therapeutic trial with LT4 should be carried out. The clinician should adequately inform the patient about the benefits and risks of LT4 treatment, since, as has recently been emphasized, shared decision making constitutes the ideal patient approach (38). This includes information about symptoms of hyperthyroidism and the risk of inappropriately high substitution. On the other hand, if after a thorough review of the patient's personal history and previous medical records, and taking the patient's general health status into account, the clinician is not convinced as to the absolute need for LT4 administration, a treatment cessation of two months is recommended. This should be particularly considered in the absence of inhomogeneous echogenicity of the gland on US.
This study has three limitations: the absence of a second elevated TSH value, the absence of long-term data concerning thyroid status of those patients in whom treatment was paused, and the potential risk of LT4 discontinuation. However, the present study reflects everyday practice and was based on real-world data. Finally, the risk of LT4 cessation for two months in hypothyroid patients is considered minimal, since this regimen has been widely used for the evaluation of patients with thyroid cancer before the implementation of recombinant human TSH in clinical practice.
To sum up, the main challenge in patients with a poorly documented diagnosis of hypothyroidism is to recognize whom to treat and whom to follow up, as well as, crucially, to identify those patients in whom their injudiciously prescribed lifelong LT4 treatment should be ceased to prevent the harmful and costly overuse of this therapy. It is clear that a well defined strategy is urgently needed for the clinical community at large. It is therefore strongly recommended that large-scale prospective studies be set up to establish precise criteria and predictive factors specifying in which patients a temporary LT4 cessation should be considered. In the case of patients on long-term thyroxine supplementation without confirmed diagnosis of hypothyroidism, a thorough review of their personal history, medical records, and thyroid US may inform the clinician in whom a trial without LT4 substitution should be implemented.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest in this work.