
Abstract
Background:
Radioiodine (131I) remnant ablation (RRA) has become a key step in the postoperative treatment of differentiated thyroid cancer (DTC). However, inadequate or excessive 131I is common using fixed activities. This study was designed to explore the feasibility of radioiodine uptake and thyroglobulin (RAIU-Tg)-guided RRA.
Methods:
A total of 277 patients were randomized to the RAIU-Tg-based activity group or a fixed activity of 3.7 GBq group at a ratio of 4:1. The RAIU-Tg-based activity was established based on four levels of RAIU (≤2%, 2–5%, 5–15%, and >15%) and Tg levels (≤2, 2–5, 5–10, and >10 ng/mL). Based on this, 131I activities of 1.1, 1.85, 3.7, and 5.55 GBq were administered. If the levels for RAIU and Tg were not in the same category, the higher activity determined by either RAIU or Tg was administered. Successful RRA was defined as negative diagnostic whole-body scan and Tg <1 ng/mL (anti-Tg antibody negative) or negative diagnostic whole-body scan (anti-Tg antibody positive) under thyrotropin stimulation six months or more post RRA.
Results:
There was no statistically significant difference in baseline characteristics between the RAIU-Tg-based activity group (n = 207) and the fixed activity group (n = 58). The activity of 131I used in the RAIU-Tg-based activity group (3.26 ± 1.54 GBq) was significantly lower than that used in the fixed activity group (p < 0.0001), whereas the rate of successful RRA in the RAIU-Tg-based activity group was significantly higher than the rate in the fixed activity group (94.2% vs. 70.7%; p < 0.0001). The rates of successful RRA in the four subgroups of the RAIU-Tg-based activity group were comparable (p = 0.543). Although there was no statistically significant difference in the incidence of total/short-term adverse effects between the RAIU-Tg-based activity group and the fixed activity group, a significantly lower incidence of intermediate adverse effects, which predominantly consisted of xerostomia, was reported in the RAIU-Tg-based activity group.
Conclusions:
Compared to a fixed activity of 3.7 GBq, RAIU-Tg-guided dosimetry can improve the success rate and decrease the incidence of intermediate side effects of RRA in postoperative patients with DTC.
Introduction
The incidence of thyroid cancer has increased dramatically in the past three decades in the United States and China (1,2). It is projected that by 2030, thyroid cancer will be the second leading cancer diagnosis in women and the ninth leading cancer diagnosis in men (3). The most common types of thyroid cancer stem from follicular cells, which account for 90–95% of cases, and are referred to as differentiated thyroid cancers (DTCs) (4). Despite differences in their biologic behavior, papillary thyroid cancer (PTC) and follicular thyroid cancer (FTC) are collectively classified as DTC and are treated with similar therapeutic regimens. The primary options for the initial management of DTC are surgery followed by radioiodine (131I) remnant ablation (RRA) and/or therapy of potential residual thyroid cancer or metastatic disease and thyrotropin (TSH) suppression therapy. These therapies tend to be associated with a favorable prognosis, as reflected by 10-year survival rates of about 90% (5).
RRA is a form of orally administered 131I therapy intended to eradicate normal thyroid tissue and microscopic cancer cells that remain after gross thyroidectomy of DTC, thereby facilitating the detection of recurrent disease, reducing recurrence risk, and facilitating initial staging by examinations such as thyroglobulin (Tg) measurements and post-therapeutic whole-body scanning (RxWBS). If RRA is successful, recurrence rates are usually 1–4% and disease-specific death <1%, resulting in a decrease in the frequency of follow-up and the degree of TSH suppression (6).
Unfortunately, the debate about the optimal activity of 131I required for RRA continues (7,8). Over the past several years, several randomized controlled trials have been published to evaluate the effectiveness of fixed activities (9 –12), adding more information on this subject matter. In these reports, some studies have demonstrated no difference in outcomes between low and high activities of 131I (9,10), whereas other investigations have shown that high activities of 131I have resulted in higher RRA success rates (11,12). These inconsistent results regarding the fixed activities of 131I prescribed for RRA were the driver to analyze further the optimal 131I activity for RRA. Each of the above-mentioned studies used fixed activities, which may yield an inadequate or excessive 131I activity in the background of individualized surgery for thyroid cancer (11,12).
Radioactive iodine uptake (RAIU), which correlates to some extent with thyroid remnant weight and the activity of the sodium–iodide symporter, has been approved by the American College of Radiology and Society of Nuclear Medicine and Molecular Imaging to estimate the mass of thyroid remnant (13). Tg is produced by thyroid tissue, and an elevated Tg serum level is indicative of the presence of thyroid remnants or metastasis of thyroid cancer (13,14). Thus, postoperative TSH-stimulated serum Tg has been recognized as a reliable marker for remnant thyroid tissue when residual or recurrent disease and metastases have been excluded (8).
This prospective, randomized, open-label, controlled trial was conducted to investigate the feasibility of RRA with regard to the stratification by RAIU combined with Tg (RAIU-Tg) under TSH stimulation.
Methods
Study conduct
All of the patients provided written informed consent prior to the initiation of the trial. The protocol was approved by the Ethics Committee of Shanghai Jiao Tong University Affiliated Sixth People's Hospital (Shanghai, P.R. China). The authors vouch for the completeness and accuracy of the data and analyses.
Patients
Patients with DTC who underwent total, near-total, or sub-total thyroidectomy and who were referred for RRA were enrolled. After the initial surgery, all of the patients were staged with the tumor-node-metastasis (TNM) staging system of the American Joint Committee on Cancer Seventh Edition and stratified into three groups (low, intermediate, and high risk) according to the 2015 American Thyroid Association (ATA) guidelines (8). Patients underwent thyroid hormone withdrawal (THW) and were on a low-iodine diet for four weeks prior to RAIU and serum tests preceding RRA. Patients with persistent/recurrent locoregional disease or distant metastases identified by imaging modalities, such as computed tomography (CT), ultrasonography (US), and technetium-99m methylene diphosphonate single-photon emission tomography/CT (99mTc-SPECT/CT), were excluded. RAIU was measured 24 hours after the administration of 0.185 MBq of 131I by a gamma counter, immediately followed by RRA. TSH, Tg, and anti-Tg antibody (TgAb) levels were measured by an electrochemiluminescence immunoassay on the Cobas analyzer (Roche Diagnostics Gmbh, Roche Ltd., Basel, Switzerland). All of the RRA patients were randomly assigned to either the RAIU-Tg-based activity group or the fixed activity group (3.7 GBq) at a ratio of 4:1. RxWBS was performed three days after 131I administration. All of the adverse effect information was recorded using standard questionnaires before and after RAI treatment.
RAIU-Tg-based activity
RAIU-Tg-based activity was determined by four levels of RAIU (≤2%, 2–5%, 5–15%, and >15%), and Tg concentrations (≤2, 2–5, 5–10, and >10 ng/mL). Based on this, 131I activities of 1.1, 1.85, 3.7, and 5.55 GBq, respectively, were administered. If the levels for RAIU and Tg were not in the same category, the higher activity determined by either RAIU or Tg was administered (Fig. 1). Prednisone (20 mg, t.i.d., per os) was given to patients with RAIU >15% before 131I administration and was continued for a total of five days.
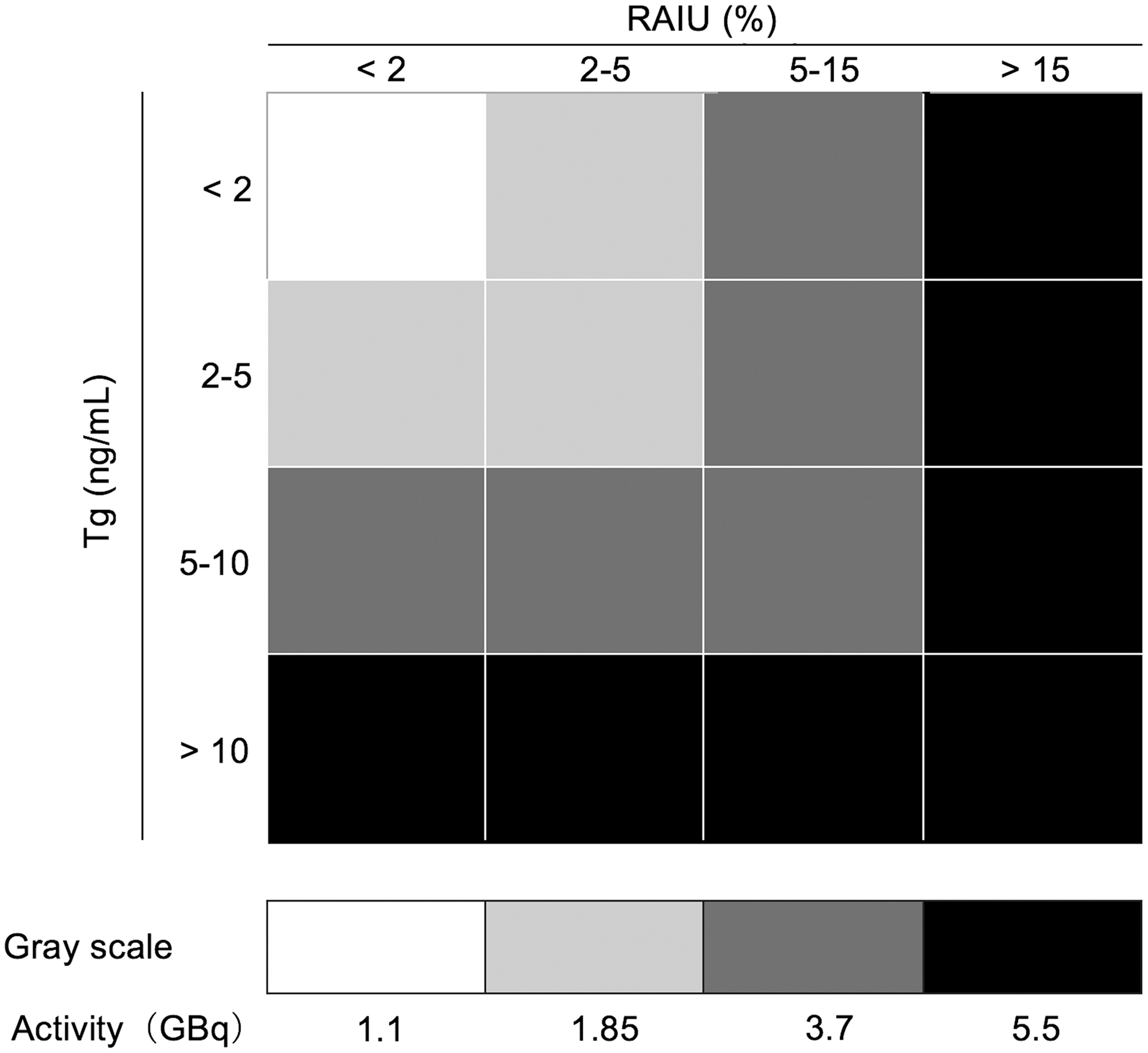
Radioiodine (131I) dosing strategies for 131I remnant ablation based on stratification of radioactive iodine uptake (RAIU) and thyroglobulin (Tg).
Outcome assessment
The primary outcome was the success rate of RRA, which was assessed six months or more after RRA using serum Tg and a diagnostic whole-body scan (DxWBS), with 185 MBq of 131I determined four weeks after THW. The secondary outcomes were short-term (≤1 month) and intermediate (about one year) adverse effects. RRA was considered successful if the levels of TSH-stimulated Tg were ≤1 ng/mL (TgAb level ≤100 IU/mL) and if the DxWBS was negative at follow-up. In cases where Tg antibodies were positive (TgAb level >100 IU/mL), successful RRA was defined as the absence of visible RAI uptake on DxWBS. To estimate the interference of TgAb, stratified analyses in patients with TgAb ≤10, 10–100, and >100 IU/mL were also performed using the defined criteria of successful RRA described above.
Statistical analyses
Descriptive quantitative data are expressed as means ± standard deviations; qualitative data are expressed as percentages. Primary and secondary comparisons were performed in the two main groups (RAIU-Tg-based activity group and fixed activity group) and four subgroups (1.1, 1.85, 3.7, and 5.55 GBq) in the RAIU-Tg-based activity group, respectively. Statistically significant differences of continuous variables were determined by independent samples t-test, Mann–Whitney U-test, or analysis of variance test as appropriate. Categorical variables were compared with Pearson's chi-square test or Fisher's exact test. The difference in observed rates of successful RRA and its bilateral confidence interval are also presented. Statistical analyses were performed using IBM SPSS Statistics for Window v24.0 (IBM Corp., Armonk, NY).
Results
Patient characteristics before RRA
In total, 277 patients were enrolled between 2013 and 2017. After the exclusion of 12 patients (five patients with distant metastases, four patients lost to follow-up, and three patients because of TSH levels <30 mIU/L), there were 265 eligible subjects with data that could be evaluated between the two groups and among the four subgroups in the RAIU-Tg-based cohort (Fig. 2). Most patients were female (77.4%) with a mean age of 42.8 ± 10.8 years. Most patients had undergone total thyroidectomy (87.5%). Sub-total and near -total thyroidectomies were performed in 6.8% and 5.7% of patients, respectively. PTCs accounted for 88.7% of all of the eligible patients. After surgery and before THW, patients received thyroid hormone therapy at a mean dose of 1.9 ± 0.4 μg/kg. Four weeks after THW, TSH levels reached >100, 60–100, and 30–60 mIU/L in 65.7%, 20.4%, and 14.0% of all of the eligible patients, respectively. Tg and RAIU ranged from <0.04–150.1 ng/mL and 0.1–40.6%, respectively. Tg levels ≤2, 2–5, 5–10, and >10 ng/mL were found in 41.1%, 23.4%, 21.1%, and 14.3% of patients, respectively. RAIU ≤2%, 2–5%, 5–15%, and >15% was found in 35.1%, 26.4%, 25.7%, and 12.8% of patients, respectively. Baseline characteristics before RRA in the RAIU-Tg-based activity and fixed activity groups are described in Table 1. In addition to the histologic subtype of DTC, the distribution of age, sex, dose of administered thyroxin before THW, interval between RRA and follow-up, operation type, and ATA risk stratification between the two groups were comparable. Furthermore, in the analyses of the characteristics of the four subgroups in the RAIU-Tg-based activity group, significant differences in the dose of administered thyroxin before THW, histologic subtype of DTC, ATA risk stratification, and stimulated TSH, Tg, and RAIU four weeks after THW were found (Table 2).

Algorithm for the inclusion and exclusion of the studied patients.
Baseline Characteristics of Patients Before Radioiodine Remnant Ablation with Regard to Dosing Strategy (n = 265)
T stage and N stage were evaluated based on American Joint Committee on Cancer 7th Edition/Tumor-Node-Metastasis Classification System for Differentiated Thyroid Carcinoma.
RAIU, radioiodine uptake; Tg, thyroglobulin; THW, thyroid hormone withdraw; ATA, American Thyroid Association.
Baseline Characteristics of Patients in RAIU-Tg-Based Activity Subgroups Before Radioiodine Thyroid Ablation Categorized by Administered 131I Activity (n = 207)
T stage and N stage were evaluated based on AJCC 7th Edition/TNM Classification System for Differentiated Thyroid Carcinoma.
TSH, thyrotropin.
Efficacy analyses of RRA
Three days post 131I administration, RxWBS showed 131I uptake in the thyroid bed in 97.1% patients in the RAIU-Tg-based activity group and in 100% of patients in the fixed activity group (p = 0.173). To analyze efficacy at follow-up, the evaluation of efficacy was performed at 11.6 ± 4.4 months (5.4–29.5 months) after RRA. TSH-stimulated Tg levels ≤1, 1–10, and 10–100 ng/mL were found in 239, 19, and 6 patients, respectively. TgAb ≤10, 10–100, and >100 IU/L were found in 72, 179, and 17 patients, respectively. The DxWBS showed an absence of 131I uptake in the neck in 93.2% of all of the eligible patients. There was no statistically significant difference in the time interval between RRA and efficacy evaluation between the two groups and among the four subgroups (Tables 3 and 4).
Outcome Analyses After Radioiodine Remnant Ablation with Regard to Dosing Strategy (n = 265)
Both local recurrence and distant metastasis were found in one patient.
TgAb, antithyroglobulin; RRA, radioiodine remnant ablation; RxWBS, post-therapeutic whole-body scan; DxWBS, diagnostic whole-body scan.
Outcome Analyses of RAIU-Tg-Based Activity Subgroups After Radioiodine Remnant Ablation Categorized by Administered 131I Activity (n = 207)
Total success rate in the RAIU-Tg-based activity group was significantly higher than the fixed activity group (94.2% vs. 70.7%; p < 0.0001), including patients with negative and positive TgAb levels. After the exclusion of patients with positive TgAb, RRA was considered successful in 89.4% patients in the RAIU-Tg-based activity group and in 69.0% of patients in the fixed activity group (p = 0.001). Table 3 summarizes the outcome of RRA in the 265 eligible patients with regard to dosing strategy. Moreover, equivalent success rates of 98.1%, 95.6%, 94.7%, and 88.7% were achieved in the four subgroups using the RAIU-Tg-based dosing strategy (p = 0.245). Table 4 shows the analysis of the main characteristics of the 207 eligible patients in the RAIU-Tg-based activity group with regard to administered activity of 131I.
Local disease, distant metastases, and retreatment
Upon follow-up, local disease and distant metastases were found in four patients in the RAIU-Tg-based activity group: one, one, and two patients had local disease or distant metastasis after RRA with activities of 1.85, 3.7, and 5.55 GBq, respectively. Three of these patients underwent 131I retreatment due to the identification of 131I-avid local disease (n = 2) and pulmonary metastases (n = 1). In the fixed activity group, two patients underwent 131I retreatment due to local disease, one had distant metastases, and one had both local disease and distant metastases. The distribution of local disease, distant metastases, and retreatment in the RAIU-Tg-based activity and fixed activity groups is detailed in Table 3, and Table 4 shows the findings in the four subgroups in the RAIU-Tg-based activity group.
Adverse effects of RRA
The incidence of total adverse effects of RRA was comparable between the RAIU-Tg-based activity group and fixed activity group within similar follow-up time (11.4 ± 4.5 vs. 12.5 ± 3.8 months; p = 0.135), and it was mainly comprised of short-term adverse effects. However, the incidence of intermediate adverse events and xerostomia was lower in the RAIU-Tg-based dosimetry group (Table 5). The incidence of intermediate adverse effects, xerostomia, xerophthalmia, and total adverse effects were activity dependent among the four subgroups in the RAIU-Tg-based activity group (Table 6).
Comparison of Adverse Events After Radioiodine Remnant Ablation with Regard to Dosing Strategy (n = 265)
Comparison of Adverse Events After Radioiodine Remnant Ablation Among RAIU-Tg-Based Activity Subgroups Categorized by Administered 131I Activity (n = 207)
Discussion
131I has been used in the treatment of thyroid disease for more than seven decades. RRA is one of the key steps in the initial management of appropriately selected DTC patients, and its main objective is the complete destruction of normal or cancerous thyroid tissue to make Tg a more reliable marker and radioiodine scanning a more accurate imaging modality, and to improve therapeutic outcomes (8,15). In the era of precision medicine, an individualized administration of 131I may be of value.
Traditionally, fixed activities of 1.1 and 3.7 GBq of 131I have been commonly prescribed, but they may be insufficient or excessive if the remnant is not appropriately evaluated (9 –12). Although previous studies comparing the efficacy of RRA with fixed 131I activities of 1.1 and 3.7 GBq in DTC patients using either recombinant TSH or THW have demonstrated non-inferiority of the low 131I activity and recombinant TSH, only patients who underwent a total or near-total thyroidectomy were enrolled. Notably, the second ablation was needed in >10% of these patients (9,10). An individualized surgical approach aimed at eradicating the tumor while reducing the risk of complications, such as hypoparathyroidism and damage of the recurrent laryngeal nerve, are widely used. For patients who have only been subjected to sub-total thyroidectomy, higher administered activities may be needed, especially for patients with larger remnants (8). In the present study, an individualized RAIU-Tg-based dosimetry was used, and it is demonstrated that this regimen is more precise in determining the prescribed activity for RRA, as it could significantly improve success rates and decrease the incidence of intermediate adverse effects. The findings are in line with the pooled data from 11 studies from a meta-analysis, which revealed that treatment with higher activities of 131I is significantly more efficient for remnant ablation, particularly after less-than-total thyroidectomy (16).
Calculated and RIAU-based activities were recently compared to traditionally fixed activities (17,18). Since the usefulness of a calculated activity has not been confirmed by clinical outcome data, an exploratory RAIU-based RRA protocol has been created (1.1 GBq for RAIU ≤5%, 1.85 GBq for RAIU 5–10%, and 2.8 GBq for RAIU >10%) and compared with fixed activities of 3.7 and 5.55 GBq. However, the success rate of 43% in the RAIU-based activity group versus 56% in the fixed activity group was disappointing (17). The present study stratified the RAIU group into more subgroups (≤2, 2–5, 5–15, and >15%), used higher activities (1.1, 1.85, 3.7, and 5.55 GBq), and considered the Tg concentration, which allowed higher activities to be administered to 26.6% of patients. This modified protocol resulted in a much higher success rate of 94.2% compared to the aforementioned study. Thus, the findings suggest that the combination of RAIU and Tg concentration can be helpful in characterizing the thyroid remnant and predicting the optimal activity for successful RRA. Moreover, this RAIU-Tg-based approach may pave a new way for thyroid remnant eradication in patients in whom complete thyroidectomy is contraindicated. Additionally, it seems that the success rate in each subgroup of the RAIU-Tg-based activity group was higher than in the fixed activity group, suggesting that accurate assessment of thyroid remnant and discriminatory treatment via this RAIU-Tg-based stratification may be of value. Notably, upon further stratification of patients in the RAIU-Tg-based activity group to subgroups based on the levels of RAIU and Tg, it was observed that the baseline characteristics in each subgroup differed in comparison to the fixed activity group. Thus, comparisons between the fixed activity group and each subgroup in the RAIU-Tg-based activity group were not performed.
Although the incidence of total adverse effects of RRA was comparable between the RAIU-Tg-based groups and the fixed activity group, the incidence of intermediate adverse effects, such as xerostomia, was significantly lower in the RAIU-Tg-based activity group than in the fixed activity group. It is well known that damage to the salivary glands is the most frequent intermediate adverse effect of RRA, since the salivary glands physiologically concentrate 131I, resulting in radiation. In this study, the occurrence of intermediate adverse events, total adverse events, xerostomia, and xerophthalmia correlated with the 131I activity, which is consistent with previous studies (9,19). Similarly, short-term adverse effects were more frequently observed in patients who received a higher activity of 131I, which is also in accordance with previous studies (20,21). Although 13.0% of patients in the RAIU-Tg-based activity group had an RAIU >15%, the incidence of neck pain was only 5.7%, which may be attributed to the prophylactic use of prednisone.
In the 2015 ATA guidelines, criteria for successful RRA involving low TSH-stimulated Tg together with negative TgAb and DxWBS were defined (8). Although negative US has been occasionally adopted as an additional criterion for successful ablation (9,10,22,23), the still existing nonviable and nonfunctioning post-ablation remnants detected by US do not necessarily mean a failure (Fig. 3). Currently, a defined cutoff for TgAb positivity is lacking. In this study, TgAb levels ≤100 IU/mL were considered as negative and >100 IU/mL as positive according to the experience of the authors' group and others (24).
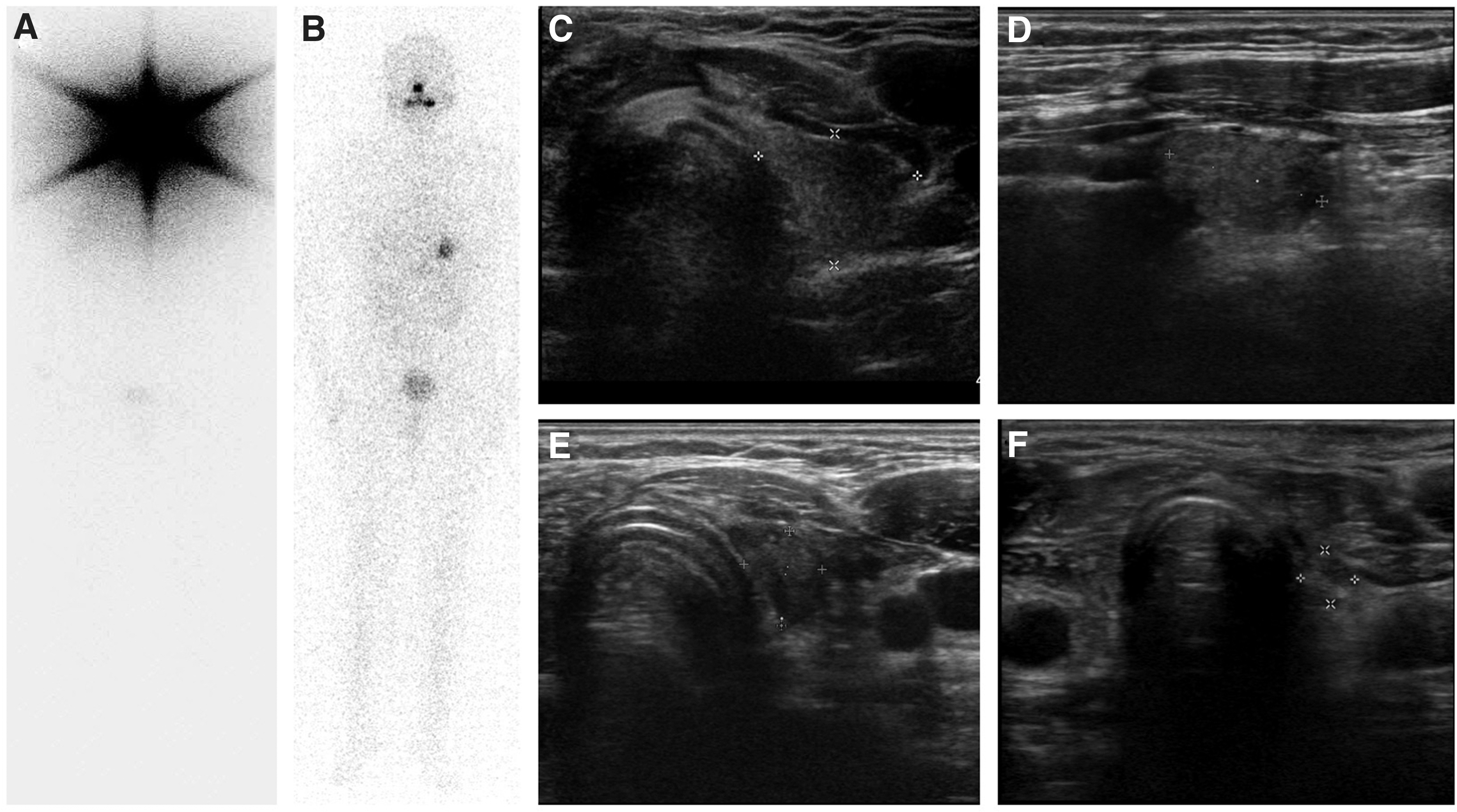
131I whole-body scan and neck ultrasonography of a 34-year-old male patient with papillary thyroid carcinoma post sub-total thyroidectomy. Whole-body scintigraphy three days after the administration of 131I (5.55 GBq) showed robust 131I uptake in the thyroid remnant (
Stunning is defined as decreased 131I uptake and efficacy mainly due to prior 131I administration (25). To reduce the possibility of stunning, the pre-therapeutic 131I activity used for diagnostic procedures should be as low as possible. In this study, only 0.185 MBq of 131I was used for the RAIU test, which is not thought to result in relevant stunning, but a pre-therapeutic DxWBS was not performed (26). Admittedly, the downside of not performing a pre-therapy scan is recognized, which is associated with the risk of not identifying patients with distant metastases prior to the first 131I treatment. To avoid for this limitation, the majority of the patients with local disease or distant metastases (high risk) had been identified by Tg testing in combination with other medical imaging modalities and excluded before RRA. Distant metastases were identified in only four (1.5%) patients by post-therapy scan, which may in part be due to the fact that a pre-therapy scan was not performed.
Other imaging modalities, especially evaluation with 18F-FDG-PET/CT, 124I PET/CT, 99mTc-SPECT/CT, or 131I-SPECT/CT, may provide more accurate postoperative assessments and facilitate planning for RRA (27 –29). It is also important to mention that the proposed RAIU-Tg-based activity determination may not be informative for complex clinical situations such as patients with renal insufficiency (30), children (31), and older individuals (32). Further studies are still needed to optimize this regimen of RRA using a neural network model, wherein the neural layers receive patient characteristics traveling from the input (characters) to the output layer (outcomes) to form a character-aided calculation flow for individualized dosing (33). Moreover, compared to the other subgroups, a relatively lower success rate of RRA (88.7%) was achieved in the RIAU >15% subgroup, despite the high activity of 131I (5.55 GBq) with concomitant administration of prednisone. Whether the administration of glucocorticoids has an impact on the ablation rate is currently unclear. Lastly, multicenter studies with a larger sample size and longer periods of follow-up are required to confirm the current findings and explore factors correlating with levels of Tg and RAIU.
In conclusion, the data suggest that compared to a fixed activity (3.7 GBq) approach, the application of the RAIU-Tg-guided RRA dosing strategy is feasible in patients with DTC, and it is associated with improved success rates and with decreased intermediate adverse effects.
Footnotes
Acknowledgments
This study was sponsored by the National Natural Science Foundation of China (grant nos. 81671711 and 81701731) and Shanghai Key Discipline of Medical Imaging (grant no. 2017ZZ02005).
Author Disclosure Statement
None of the authors have any conflicts of interest to declare.