
Abstract
Background:
Thyroid cancer constitutes a major and increasing proportion of head and neck cancers in children and adolescents. The purpose of this study was to determine the incidence and survival of thyroid cancer in Danish patients aged 0–24 years from 1980 to 2014.
Methods:
Patients aged 0–24 years registered with primary thyroid cancer in the Danish Cancer Registry or the Danish Pathology Data Bank during 1980–2014 were included. Crude incidence rates and age-adjusted incidence rates (AAIR) per 100,000, average annual percent change (AAPC), and overall survival (OS) were evaluated in relation to sex, histopathological tumor type, age at diagnosis, and year of diagnosis.
Results:
A total of 297 thyroid cancer patients (72% female, 72% papillary carcinoma) were identified. The AAIR per 100,000 increased significantly from 0.36 in 1980 to 0.97 in 2014, with an AAPC of 2.9%. There was no significant increase in incidence among children and adolescents (0–17 years). However, among young adults (18–24 years), a significant increase in incidence was observed (AAPC 3.7%). The incidence of thyroid cancer increased with age from 0.05 among infants aged 0 years to 1.73 among young adults aged 24 years. Female patients and papillary carcinoma showed significant increase in incidence (AAPC 3.3% and 3.2%), whereas male patients and other histopathological tumor types showed no change. The 15-year OS was 99%. The lowest 15-year OS was observed among patients with medullary carcinomas at 96%. There was no significant difference in OS between groups based on histopathological tumor type, and there was no significant change in OS over time.
Conclusion:
In this nationwide study, no change in OS was observed, but a significant increase was seen in the incidence of thyroid cancer among young adults (aged 18–24 years), mainly attributed to an increase among females and patients with papillary carcinoma. No increase in incidence was seen among children and adolescents. These findings demonstrate the excellent prognosis for children and adolescents diagnosed with thyroid cancer.
Introduction
T
The incidence of thyroid cancer among children and adolescents are lower compared to the adult population. However, malignancy in the thyroid appears in up to 43% of palpable nodules among children compared to 5% among adults (6 –11).
Few studies have reported the incidence and survival of thyroid cancer among children and adolescents. The majority of these studies are based on data from the United Stated, and other nationwide data are sparse. The aims of this study were to evaluate the incidence and survival of thyroid cancer according to sex, histopathological tumor type, year of diagnosis, and age at diagnosis among patients aged 0–24 years in Denmark from 1980 to 2014.
Methods
Data were obtained from the following nationwide registries: the Danish Cancer Registry (DCR), the Danish Pathology Data Bank (DPDB), and the central population register (CPR). The DCR contains nationwide data on cancers diagnosed in Denmark from the year 1943 and onwards. Reporting to the DCR became mandatory in 1987 (12). The DPDB serves as a nationwide database of pathology investigation conducted in Denmark since 1970 (including all departments of pathology in Denmark since 1990). Samples are coded according to a Danish version of the Systematized Nomenclature of Medicine (SNOMED) (13).
Age at diagnosis was obtained from the DCR and the DPDB. Vital status and emigration were obtained from the CPR, which since 1968 has provided every resident in Denmark with a unique personal identification number, making individual level linking across registries possible.
All patients between 0 and 24 years of age registered with the first case of thyroid cancer during 1980–2014 in the DCR or DPDB were included in the study. Duplicates were excluded.
Thyroid cancer was defined as registrations in the DCR with the ICD-10 code DC73.9 and from the DPDB with the SNOMED codes T96000, T96010, T96050, T96100, T96200, T96300, and T96400.
The histopathological diagnosis was derived from the ICD-O-3 classification via the MORPHO3 registration from the DCR, and from the SNOMED classification from the DPDB. For statistical analysis, histopathological tumor types were categorized into four groups: papillary carcinoma (MORPHO3 codes: 80503 and 82603), follicular carcinoma (MORPHO3 codes: 82903, 83303, 83313, and 83403), medullary carcinoma (MORPHO3 code: 85103), and others (rhabdomyosarcoma, unspecified carcinomas, and other unspecified malignancies; MORPHO3 codes: 80003, 80013, 80103, 80203, 81403, and 89003). Year of diagnosis was categorized in five-year intervals to create the lowest amount of evenly sized groups. Age at diagnosis of the first incidence of thyroid cancer was categorized into two groups: children and adolescents aged 0–17 years, and young adults aged 18–24 years.
Information on TNM classification was not included due to missing data in the included registries.
Statistical analysis
Statistical analyses were performed using R statistics v3.3.3 (Stanford University, Stanford, CA) (14). The incidence rates were calculated as crude incidence rates and age-adjusted incidence rate (AAIR). AAIR circumvents that the distribution of age groups can be different between populations, allowing the numbers to be compared to any given population directly. The AAIR were calculated per 100,000 using the direct method with the EpiTools package (15) using the Danish population between 0 and 24 years of age as reference and the World Health Organization world standard population weighing (16). The weight of the age groups between 0 and 24 years were recalculated so the weights of these groups had the sum of 100. Age-specific incidences were calculated using the average population between 1980 and 2014 for the given age. The average annual percent change (AAPC) was calculated using Joinpoint trend analysis software v4.2.0.2, with growth assumed to be logarithmic with the formula ln(y) = xb. The Joinpoint regression analysis estimates possible joinpoints (trend breaks), which are significant changes in trends.
To reduce large fluctuations, incidence curves were created using three-year rolling-average, meaning that the incidence shown is the average of the given years and the two years before. Any given point on the curves can therefore be marginally higher or lower than the actual incidence in a given year.
Survival was analyzed as overall survival (OS), defined as the time from diagnosis to death from any cause. Patients who were alive at the last date of follow-up were censored at this date. The date for the last follow-up was the December 31, 2016. Cox regression analysis was used to illustrate survival differences. p-Values <0.05 were considered to indicate statistical significance.
Results
The study identified 297 patients aged 0–24 years with thyroid cancer from the DCR and the DPDB for the period 1980–2014. Of these, 294 patients were registered in the DCR and 80 were registered in DPDB. Seventy-seven patients were registered in both databases, 217 patients were only registered in the DCR, and three patients were only registered in the DPDB. The patients were predominantly female (n = 213; 72%; Table 1), and there was no difference in the sex distribution between the two age groups (Table 2). The most common histopathological tumor type was papillary carcinoma, accounting for 72% of cases (n = 214; Table 3). The distribution of histopathological tumor types was significantly different between children and adolescents (0–17 years) and young adults (18–24 years), consisting mostly of a difference in the share of medullary carcinomas (Table 2). The overall median age at diagnosis was 21 years (range 0–24 years). In children and adolescents, the median age at diagnosis was 14 years (range 0–17 years).
The p-value was calculated using a t-test.
The p-value was calculated using a chi-square test.
Incidence of thyroid cancer patients aged 0–24 years
The total AAIR per 100,000 increased significantly from 0.36 in 1980 to 0.97 in 2014 (Fig. 1), corresponding to a total number of 7 and 18 cases per year, and accounting for an AAPC of 2.9% [confidence interval (CI) 1.7–4.2].
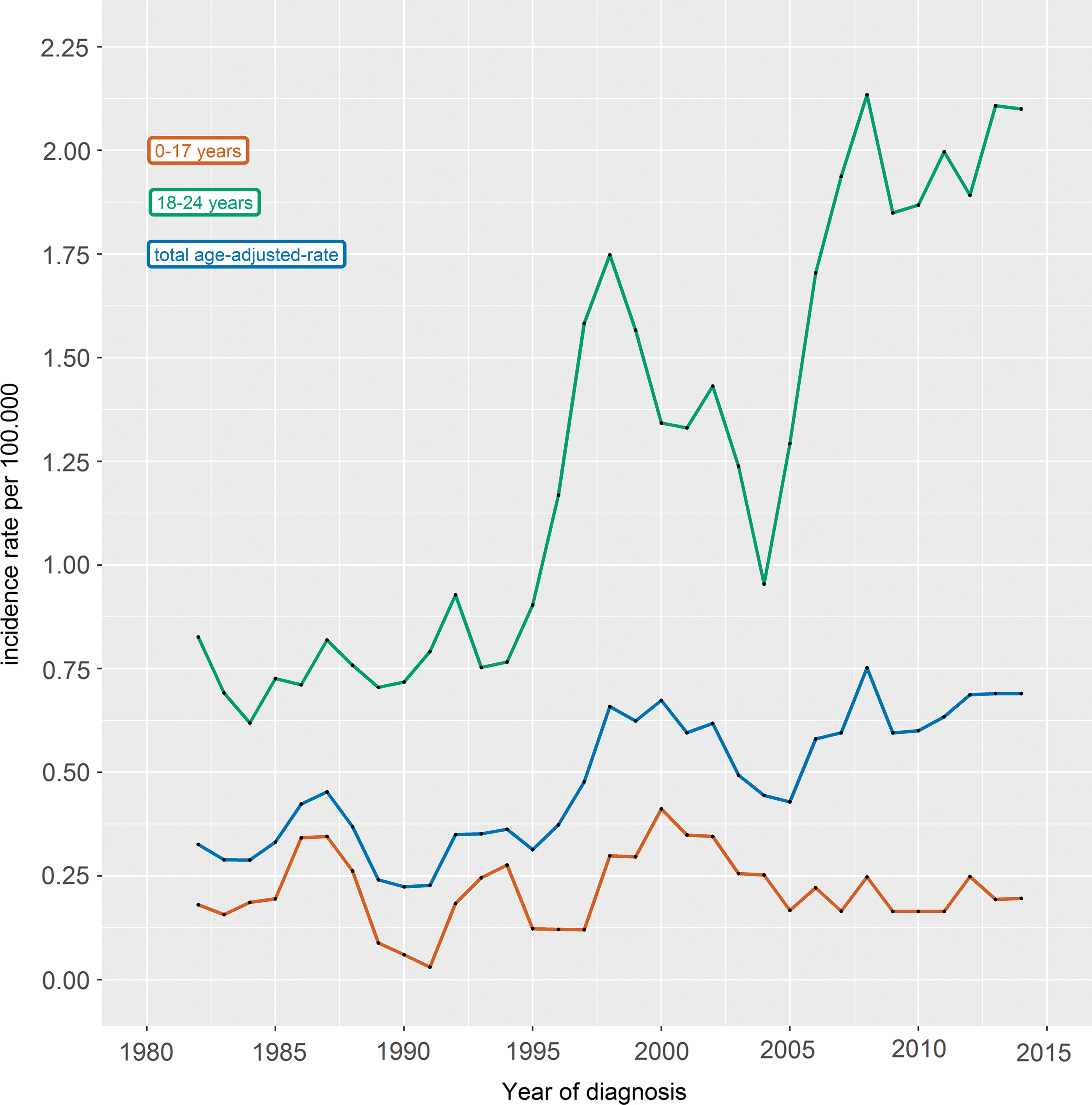
Three-year rolling average of crude incidence rates per 100,000 for patients aged 0–17 years and patients aged 18–24 years, and total age-adjusted incidence rates per 100,000. Color images available online at
The incidence among children and adolescents was significantly lower compared to young adults (Table 1), and no significant change in incidence over time was observed. Among young adults, the incidence increased significantly (AAPC 3.7% [CI 2.4–5.0]) from a crude incidence rate per 100,000 of 1.15 in 1980 to 2.91 in 2014 (Fig. 1).
For female patients, the AAIR per 100,000 increased significantly from 0.21 in 1980 to 0.75 in 2014, corresponding to an AAPC of 3.3% [CI 1.8–4.8]. The AAIR per 100,000 for males was 0.15 in 1980 and 0.21 in 2014, with no significant change.
In patients with papillary carcinomas, the AAIR per 100,000 increased significantly from 0.26 in 1980 to 0.79 in 2014, and showed an AAPC of 3.2% [CI 1.7–4.7], whereas no significant change was observed among patients with other tumor types.
The incidence increased significantly with age from a total crude incidence rate per 100,000 of 0.05 at the age of 0 years to 1.70 at the age of 24 years (AAPC 50.3% [CI 28.2–76.3]), for males from 0 at the age of 0 years to 0.70 at the age of 24 years (AAPC 63.2% [CI 39.5–91.0]), and for females from 0.94 at the age of 0 years to 2.73 at the age of 24 years (AAPC 70.4% [CI 40.2–107.1]; Fig. 2). No significant changes in trends were demonstrated in any trend analysis.
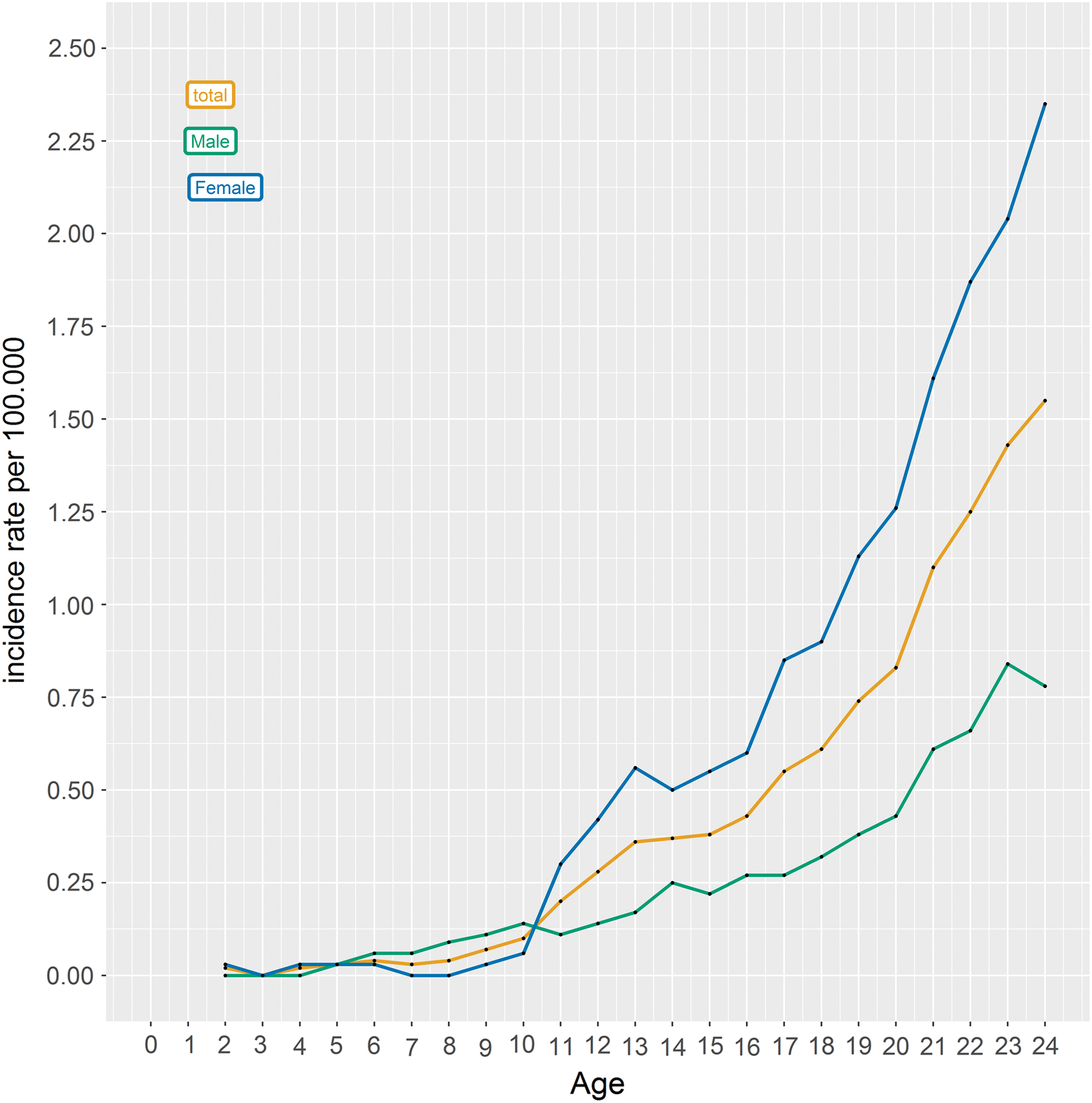
Three-year rolling average of age-specific incidence rate per 100,000 for sexes and total. Color images available online at
Survival of patients diagnosed with thyroid cancer aged 0–24 years
At a median follow-up of 15.4 years (range 0.5–37 years), nine deaths were registered, all among young adults, four among females and five among males. Considering tumor type, there were six deaths among patients with papillary carcinoma, two among patients with medullary carcinoma, and one death of a patient with a carcinoma that was not otherwise specified (Table 3). Age at death among the patients with fatal outcome was between 21 and 56 years. Three patients were <30 years of age at death (aged 21, 24, and 28 years), one patient was 38 years old, and the remaining patients were >40 years of age at death (aged 42, 49, 52, 54, and 56 years). The 15-year OS was 99%. Patients with follicular carcinoma and other histology had a 15-year survival of 100%. Medullary carcinoma had the lowest 15-year survival at 96%. There were no significant differences in the OS between the sexes or histopathological tumor types (Table 3). Also, no significant change was observed in the OS during the 35 years (Table 3).
Discussion
In this nationwide study spanning nearly four decades, an increasing incidence of thyroid cancer is reported among young adults in Denmark, with no incidence change among children and adolescents. Further, the increased incidence of thyroid cancer among young adults was mainly attributed to an increase among females and patients with papillary carcinoma.
A lower incidence of thyroid cancer is reported among children and adolescents compared to other studies, with no change in incidence observed in contrast to other reports (1,2). These differences might partly be explained by the fact that the age group was categorized as 0–17 years, where similar studies have included patients up to 20 years of age. The increased incidence among young adults in the present study is similar to reports of the adult population (17,18).
A higher incidence was observed among females compared to males. This has been demonstrated previously (1,2,4), and it has been suggested that this difference may be caused or modulated by estrogens (19,20).
No significant changes in trends were demonstrated in the age-specific incidence rates. However, the curve seems to demonstrate a change around the age of 10 years, especially among female patients. An increase in incidence at the onset of puberty has also been demonstrated by others (20,21). The explanation for this is plausibly the increase in female sex hormones at puberty.
A significant difference was observed in the distribution of tumor types between children and adolescents and young adults. This finding is most likely explained by the fact that medullary carcinomas in patients with a hereditary genetic predisposition for this cancer most commonly present in childhood, explaining why this tumor is more common among children and adolescents (22).
Further, an excellent OS of thyroid cancer is reported, especially among children and adolescents. Because there were no deaths in this group, it was not possible to analyze the difference in survival between the age groups. However, other studies report that poorer survival is correlated to higher age at diagnosis (2).
There were no significant differences in survival between the sexes, histopathological tumor types, or year of diagnosis groups. The hazard ratio that was closest to demonstrating a significant difference was a better survival among female patients compared to males (p = 0.10). Better survival for female patients has been demonstrated before (1,4).
Although patients with medullary carcinomas, similar to other studies, had the lowest survival rate compared to patients with other thyroid cancers, survival remained very high, with no significant difference compared to the other histopathological tumor types (1,2,4). The lack of a significant difference in survival between the sexes and histopathological tumor types might be explained by the few events and relatively few patients.
There is a large discrepancy between the numbers of registered patients in the two databases included in this study. This is mostly due to a number of patients that are registered in the DCR but not in the DPDB. Therefore, it seems that the problem mostly relies on incomplete registration in the DPDB. This is, however, a minor concern in this study because the patients missing in the DPDB were registered in the DCR, although registration errors should be considered as a possible bias.
In summary, this study reports an increasing incidence of thyroid cancer in young adults (aged 18–24 years). However, no change in incidence was seen among children and adolescents (aged 0–17 years). The increase among young adults is mainly attributed to an increase among female patients and those with papillary carcinomas. Further, excellent 15-year OS of 99% is reported, with no registered deaths among children and adolescents, demonstrating the superior prognosis of children, adolescents, and young adults diagnosed with thyroid cancer.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.