
Abstract
Background:
Thyroglobulin (Tg) antibodies (TgAb) can interfere with Tg measurement and can be used as “Tg surrogate” in patients with differentiated thyroid cancer (DTC) treated with total thyroidectomy (TTx) and radioiodine remnant ablation (RRA). In contrast, few data, and in patients usually followed for a short-term follow-up, have been reported about the changes of TgAb levels in patients treated with TTx but without RRA. The aims of this study were to evaluate the changes of TgAb levels in DTC patients treated with TTx but not RRA and to identify the factors that influence these changes.
Methods:
The change in TgAb levels in 107 DTC (<1 cm) patients submitted to TTx but not RRA was evaluated. Patients were followed for a median of 6.3 years, and all had at least three determinations of TgAb and neck ultrasound (nUS).
Results:
TgAb levels showed a progressive decrease during follow-up. Initial TgAb levels and degree of lymphocytic infiltration influenced the time but not the rate of TgAb disappearance. No influence on time and rate of the decrease in TgAb was observed when the association with thyroperoxidase antibodies (TPOAb) levels were considered. A TgAb cutoff value of 61.9 IU/mL at first postoperative evaluation was a good indicator for disappearance of the TgAb within six years. No tumor recurrence was observed in the series. In one case, the progressive increase in TgAb anticipated the reappearance of benign thyroid tissue with lymphocytic infiltration.
Conclusions:
TgAb levels decline in the majority of DTC patients treated with TTx but not ablated with radioiodine. The levels decrease rapidly after the surgical treatment and continue to decrease over time. The time of disappearance is influenced by the initial TgAb levels and the degree of lymphocytic infiltration. No influence of the actual TPOAb levels has been observed. An increase in TgAb levels should not be overlooked, since it can indicate the presence or reappearance of either normal thyroid tissue or tumor recurrence.
Introduction
F
In the last five years, the use of 131I for remnant ablation has been reconsidered, and currently, a rather large number of DTC patients (i.e., almost all low-risk and many intermediate-risk patients) are no longer treated with RRA (6). In these cases, the change in the serum Tg levels over the time, more than its absolute value (undetectable or detectable), still represents a good tumor marker (7,8).
It is well known that approximately 25–30% of patients with DTC have serum thyroglobulin antibodies (TgAb) (9,10) that can interfere with Tg measurements, causing false-negative results when Tg is measured with immunometric assays (IRMA), and either false-positive or negative results when it is measured with radioimmunoassays (RIA) (11,12). TgAb expression results from an associated lymphocytic thyroiditis (LT) or an immune reaction to DTC (13). In these cases, serum Tg loses its value as a tumor marker, but the change in the serum TgAb levels over the time can be used as a “Tg surrogate,” since it has been demonstrated that TgAb levels decline and become undetectable in cured DTC patients (14,15). At the same time, the persistence of stable levels of TgAb for a long period of time or the increase in TgAb levels after TTx ±RRA represents an alert indicating the possibility of persistence or recurrence of DTC (16,17). Currently, this concept is so well established that the new American Thyroid Association guidelines for the management of DTC include the TgAb measurement after initial treatment as essential to assess the ongoing risk stratification (6).
While the use of TgAb trend as a “Tg surrogate” marker has been recognized as valuable in patients treated with TTx and RRA (16), few data, and in patients usually followed for a short-term follow-up, have been reported about the changes of TgAb levels in patients treated with TTx but without RRA (18,19).
The primary objective of this study was to evaluate the trend of TgAb levels in DTC patients treated with TTx but not RRA over a median period of 76 months (i.e., 6.3 years). As a secondary objective, the study aimed to identify those factors that potentially influence the TgAb trend over time.
Methods
Study group
The epidemiological, clinical, and pathological data were evaluated of a series of consecutive DTC patients, followed at the Endocrine Unit of the University Hospital of Pisa between 2005 and 2013 who, in accordance with the European consensus indications (20), had not received RRA. In all cases (n = 383), patients who were not treated with RRA had unifocal micropapillary thyroid cancer (no-RRA mPTC) without histological evidence of lymph node metastases.
All patients were treated with TTx at the Endocrine Surgical Unit at the same hospital. Patients were all on levothyroxine (LT4) therapy at the time of enrolment and for the duration of the study. Clinical and biochemical data were collected before and after surgery (M = 6.4 ± 9.9 months; median = 5 months) and approximately every 18 months during the follow-up.
Among all no-RRA mPTC patients, a subgroup of patients was selected according to the following criteria: (i) circulating TgAb >8 IU/mL at the time of first postoperative clinical evaluation and (ii) patients who had at least three determinations of serum TgAb and neck ultrasound (nUS) performed in the department.
According to these criteria, 107/383 (27.9%) patients were included in the present study. All patients, as per hospital policy, signed an informed consent for the collection and the treatment of their clinical and biochemical data. All patients were informed about the study, which was approved by the Institutional Review Board.
The epidemiological and clinicopathologic features of the study group are reported in Table 1.
PTC, papillary thyroid carcinoma; FV-PTC, papillary thyroid carcinoma follicular variant; TCV-PTC, papillary thyroid carcinoma tall-cell variant; TSH, thyrotropin.
Measurement of serum TgAb and thyroperoxidase antibodies
Serum TgAb and thyroperoxidase antibodies (TPOAb) were measured by a Fluorescence Enzyme Immuno Assay (AIA-Pack 2000; Tosoh Corporation, Tokyo, Japan). For TgAb, the manufacturer recommended a cutoff for the identification of thyroid autoimmune disease with a thyroid gland in situ of 30 IU/mL. The analytical sensitivity, which refers to the precision of the zero matrix, was 6 IU/mL according to the manufacturer and 1 IU/mL according to the authors' laboratory. The functional sensitivity as evaluated in the laboratory, that is, the only parameter relevant for Tg measurement, was 8 IU/mL, as established from the 20% between-run CV, according to the National Association of Clinical Biochemistry guidelines (21). The cutoff suggesting interference with Tg measurements (TgAb value that better discriminates between undetectable and detectable Tg by receiver operating characteristic [ROC] analysis) was 9.3 IU/mL (11). Positive cutoff and analytical sensitivity of TPOAb were 10 and 3 IU/mL, respectively.
Neck ultrasonography
A color Doppler apparatus (MyLab 50; Esaote Biomedica, Firenze, Italy) with a 7.5–12 MHz linear transducer was used to perform nUS. Central and bilateral neck lymph node compartments and the superior mediastinum were inspected. Suspected lesions found at nUS were evaluated by US-guided fine-needle aspiration cytology (FNAC) and measurement of Tg in washing fluid.
Histopathology
In all cases, mPTC was defined on the basis of its largest size ≤1.0 cm. No multifocality and/or lymph node metastases were present in these 107 cases, since, at that time, multifocal mPTC with or without lymph node metastases were treated with RRA. All cases were papillary microcarcinomas on histology and were re-evaluated by two pathologists (L.T. and F.B.) for the identification of an associated LT (22), which was evaluated at low power magnification (10 × ). In the presence of an associated LT, three degrees of lymphocytic infiltration were defined, according to the following criteria (23): (i) focal—focal aggregates of lymphocytes within the follicular epithelium in the absence of oxyphilic metaplasia, follicular atrophy, or follicular disruption; (ii) moderate—diffuse but not extensive lymphocytic infiltration with or without germinal center formation and focal oxyphilic metaplasia; and (iii) massive—extensive lymphocytic infiltration with germinal center formation, atrophic follicles, diffuse oxyphilic metaplasia, and an eventual increase in fibrosis.
Statistical analysis
Statistical analyses were performed in SPSS Statistics for Windows v21 (IBM Corp., Armonk, NY). Skewed variables (TgAb and TPOAb) were log10-transformed to approximate a Gaussian distribution. Data are reported as the mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate.
Changes in TgAb and TPOAb levels (log10 values) at the first postoperative visit were analyzed by paired Student's t-tests, and the results were exponentiated to express changes as a percentage. Linear mixed models were used to analyze data collected at each visit, including “time” as a fixed effect and accounting for repeated measures using a first-order autoregressive covariance structure. Similar models were used to compare trajectories over time between lymphocytic infiltration groups and TPOAb+/− groups, including “group” as fixed effect and the “time–group” interaction term to evaluate potential different rates of Ab change over time between groups.
ROC curves were calculated to identify the best cutoff value for TgAb that better discriminated between patients who achieved negativization during the course of follow-up in terms of sensitivity and specificity (i.e., highest Youden index). The negativization curves of each TgAb group were calculated by the Kaplan–Meier method and compared by the log-rank test.
Results
Time changes of TgAb and TPOAb levels during follow-up in no-RRA mPTC patients
As shown in Figure 1, the comparison of the changes in TgAb and TPOAb levels before and after surgery (i.e., at first postoperative control performed after a mean of 6.4 ± 9.9 months; median 5 months) showed that the mean percentage of decrease was −59% ([confidence interval (CI) −69% to −45%]; p < 0.001) for TgAb, and −52% ([CI −69% to −26%]; p = 0.001) for TPOAb. When we evaluated the mean values of both TgAb and TPOAb levels during the follow-up of the study group (6.3 years; range 76 ± 20 months), they showed a progressive and continuous decrease. The mean percentage of decrease per year was −47%/year ([CI −51% to −42%]; p < 0.001) for TgAb, and −30%/year ([CI −35% to −24%/year; p < 0.001) for TPOAb (Fig. 2).
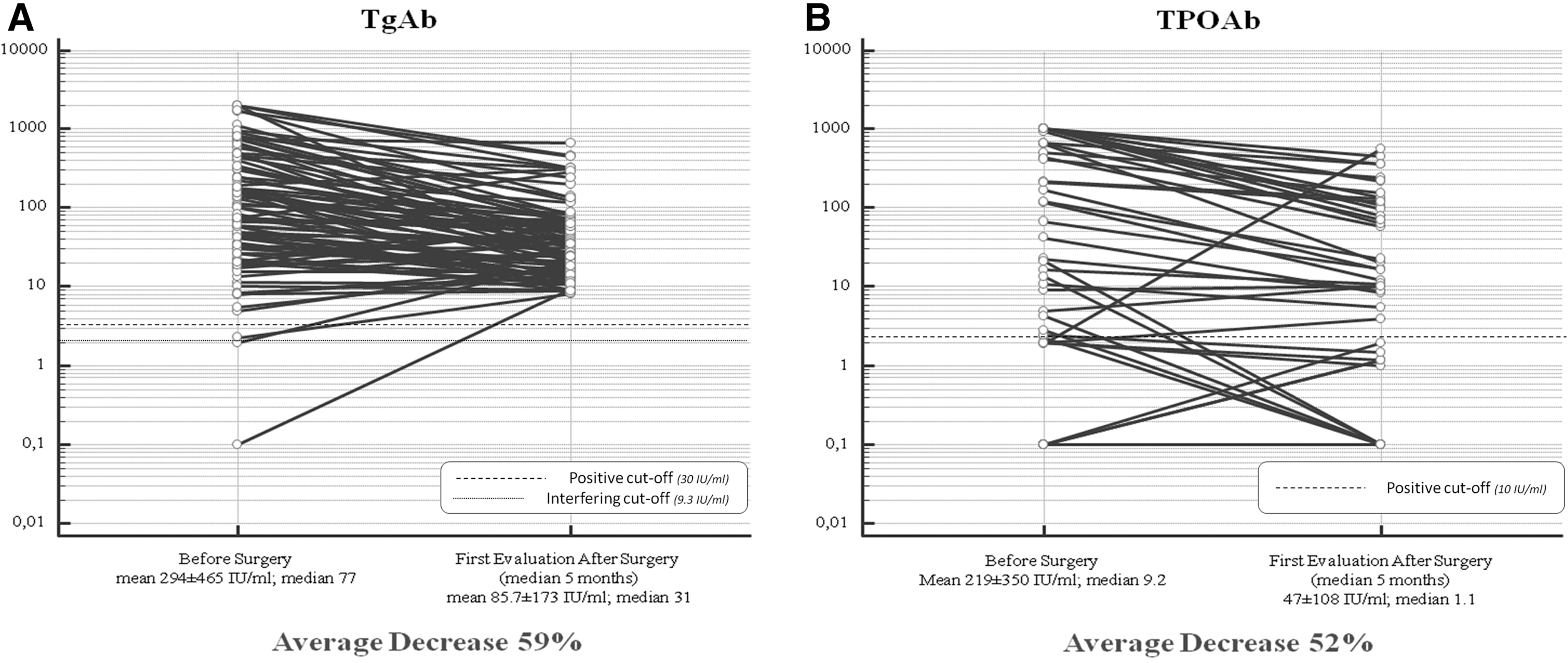
Changes in (

Changes of TgAb and TPOAb levels during the 6.3 years median follow-up.
Factors potentially influencing the decreasing trend of serum TgAb and TPOAb
TgAb levels
In 67/107 (62.6%) patients, TgAb levels became undetectable (<8 IU/mL) during the follow-up and remained negative until the end of the observation. When the cases were divided according to the levels of TgAb as assessed at the first postoperative evaluation (Table 2), it was observed that the time of TgAb disappearance was dependent on the initial value; the higher the initial value, the longer the time of disappearance.
First postoperative biochemical evaluation.
TgAb, thyroglobulin antibodies.
To identify a TgAb cutoff value able to predict TgAb disappearance (<8 IU/mL) at any time during the follow-up period, ROC curve analysis was performed. As shown in Figure 3, when considering the first postoperative value of TgAb, a cutoff value of 61.9 IU/mL was found, with a balanced sensitivity (86.6%) and specificity (47.5%).

The receiver operating curve (ROC) curve analysis of TgAb levels at first postoperative control identified the value of 61.9 IU/mL as the cutoff, with the best sensitivity (86.6%) and specificity (47.5%) to predict the possibility of TgAb to become negative (<8 IU/L) in a median time of 6.3 years.
In all patients, except one, nUS was persistently negative for the presence of local thyroid tissue (i.e., normal remnant tissue or persistent/recurrent tumor tissue). Only one patient experienced the reappearance of thyroid tissue in the thyroid bed four years after TTx and previously negative nUS findings; FNAC confirmed the presence of normal thyroid tissue with lymphocytic infiltration (Fig. 4). Simultaneously, an increase in TgAb levels, which was never completely undetectable, was observed and persisted up to the end of follow-up (Fig. 5).
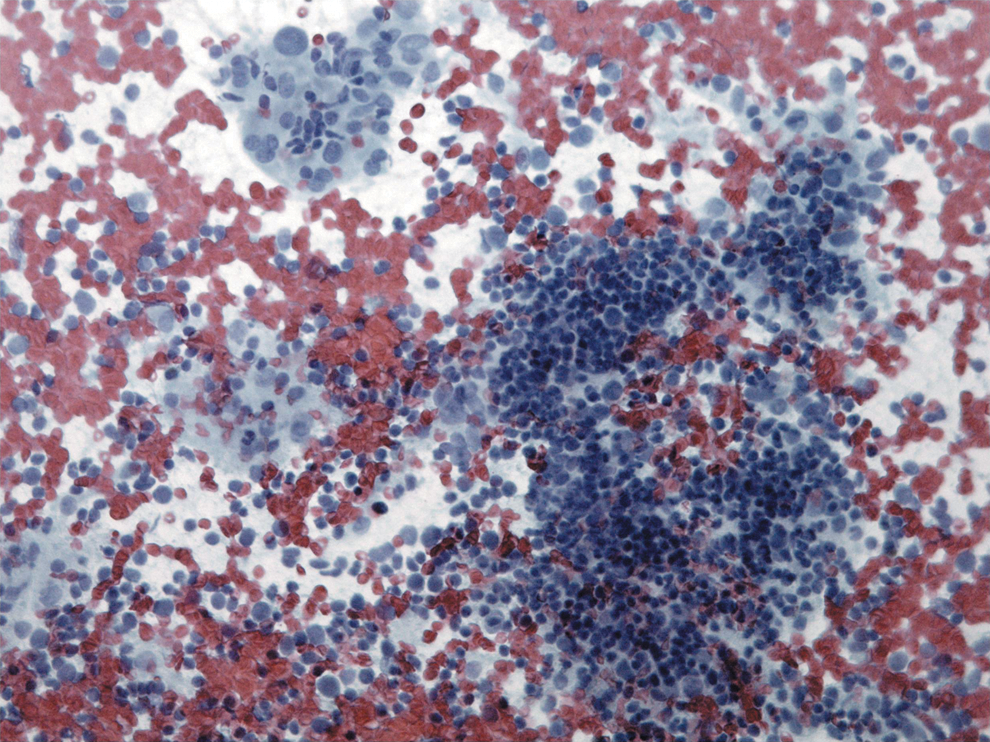
Cytological smear of the only case with reappearance of benign thyroid tissue with lymphocytic infiltration. The aspirate is composed of abundant heterogeneous population of lymphocytes and occasional small groups of follicular cells with oncocytic features (Papanicolau, original magnification 20 × ). Color images available online at
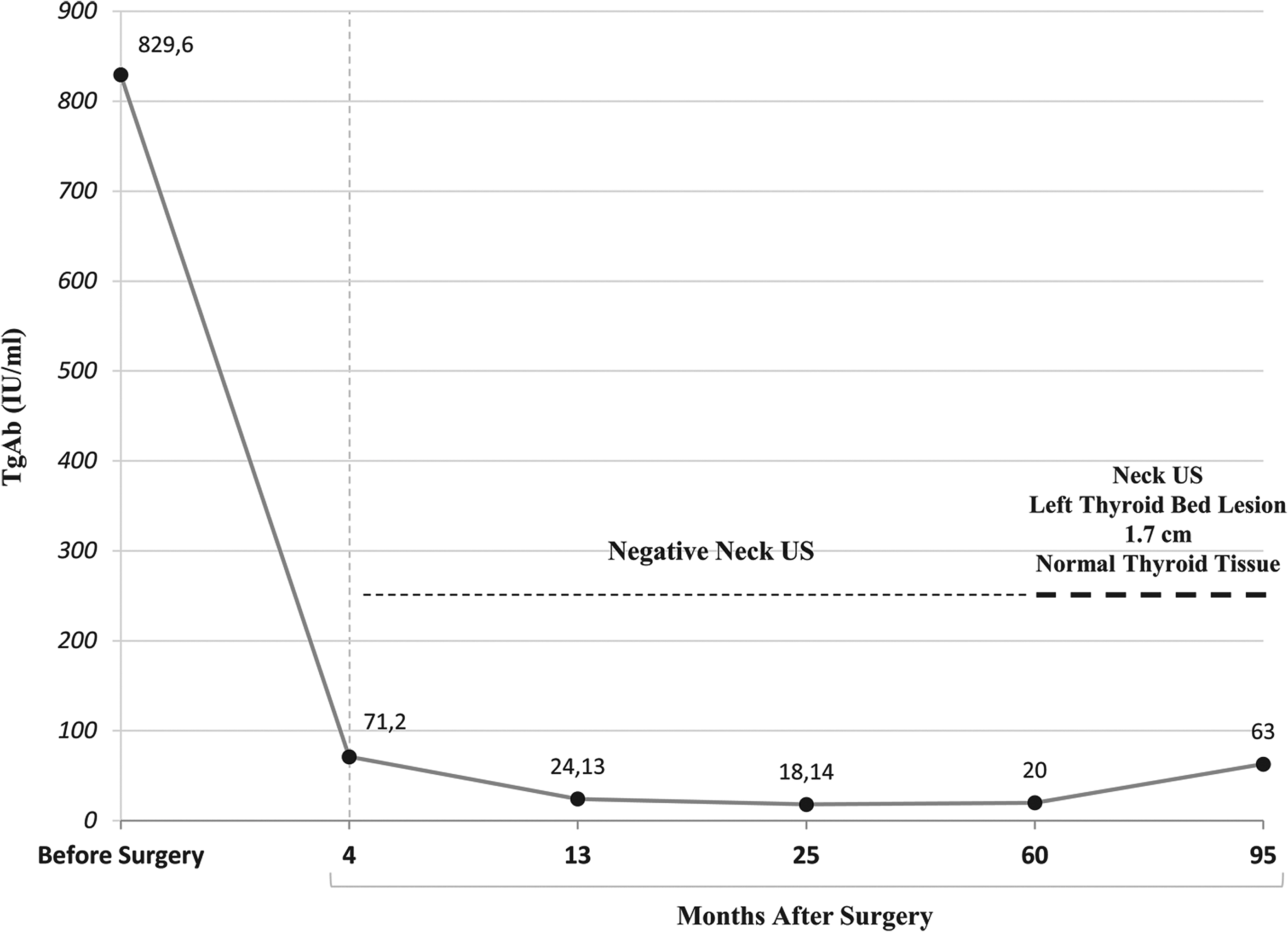
Changes in TgAb levels in the single patient with evidence of reappearance of normal thyroid tissue as demonstrated by neck ultrasound and fine-needle aspiration cytology.
Lymphocytic infiltration
As previously reported, histological samples were distinguished on the basis of the degree of lymphocytic infiltration (i.e., absent, focal, moderate, and massive). As shown in Figure 6, it was found that the values of both TgAb and TPOAb detected before surgery correlated with the degree of lymphocytic infiltration, being higher in cases with massive infiltration and lower in those with no infiltration. The comparison of TgAb levels before surgery between massive/moderate (M = 347 ± 444 IU/mL; median = 146 IU/mL) and focal/absent (M = 240 ± 485 IU/mL; median = 49 IU/mL) lymphocytic infiltration showed a slight but not significant difference (p = n.s.). In contrast, TPOAb levels significantly differed when considering massive/moderate (M = 394 ± 398 IU/mL; median = 257 IU/mL) compared to focal/absent (M = 41 ± 156 IU/mL; median = 1 IU/mL) lymphocytic infiltration (p < 0.001). Nevertheless, the presence and the amount of the lymphocytic infiltration did not affect the downward trend during the time of either TgAb (Fig. 6A) or TPOAb (Fig. 6B). In particular, TgAb levels showed the same rate of decrease in all four categories (p = n.s.; Fig. 6A). In contrast, TPOAb levels showed a significantly faster rate of decrease in massive (−46%/year; p < 0.001) and moderate (−42%/year; p < 0.001) infiltrated cases compared to cases with no infiltration (Fig. 6B). No difference in the rate of decrease in TPOAb levels was observed in cases with focal infiltration compared to those without infiltration (−35%/year; p = 0.08).
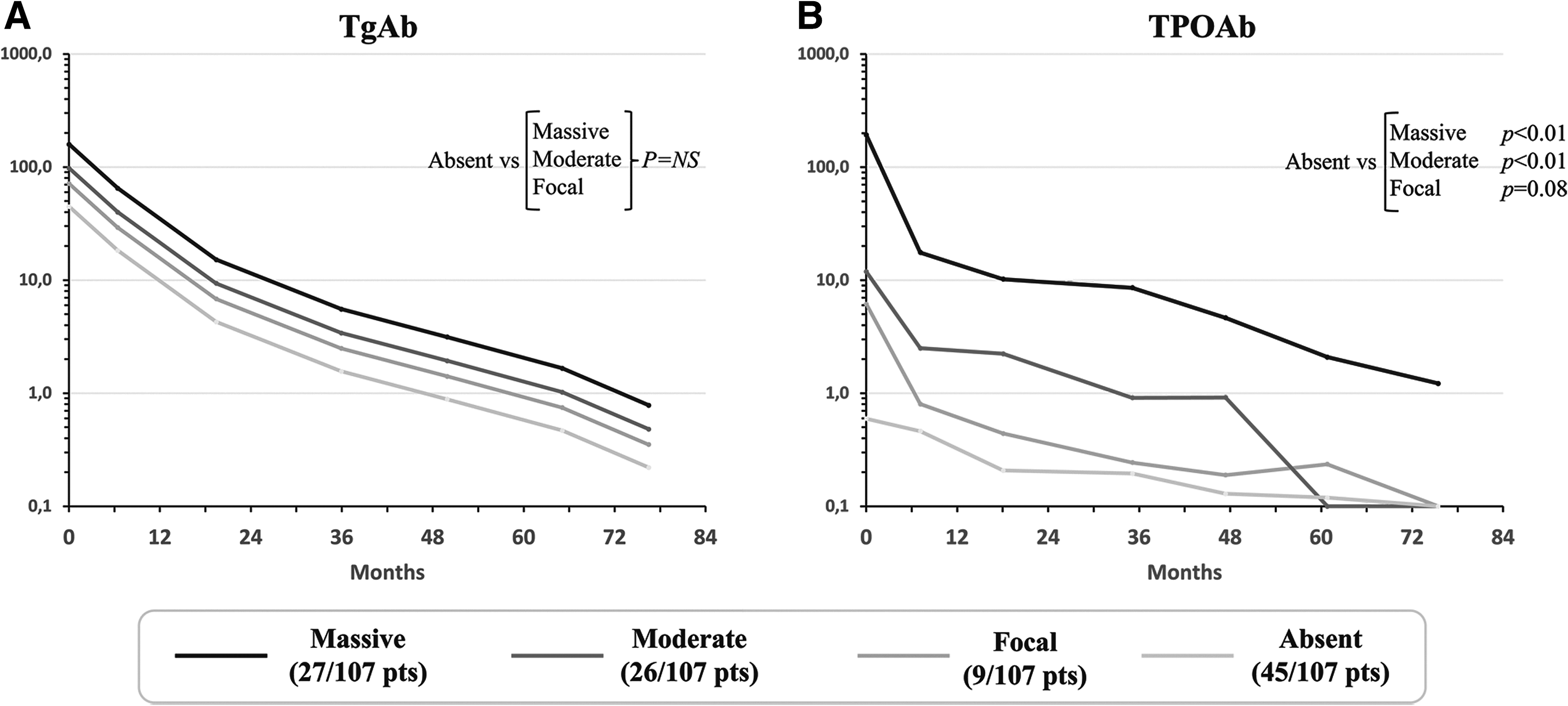
Correlation between (
TPOAb levels
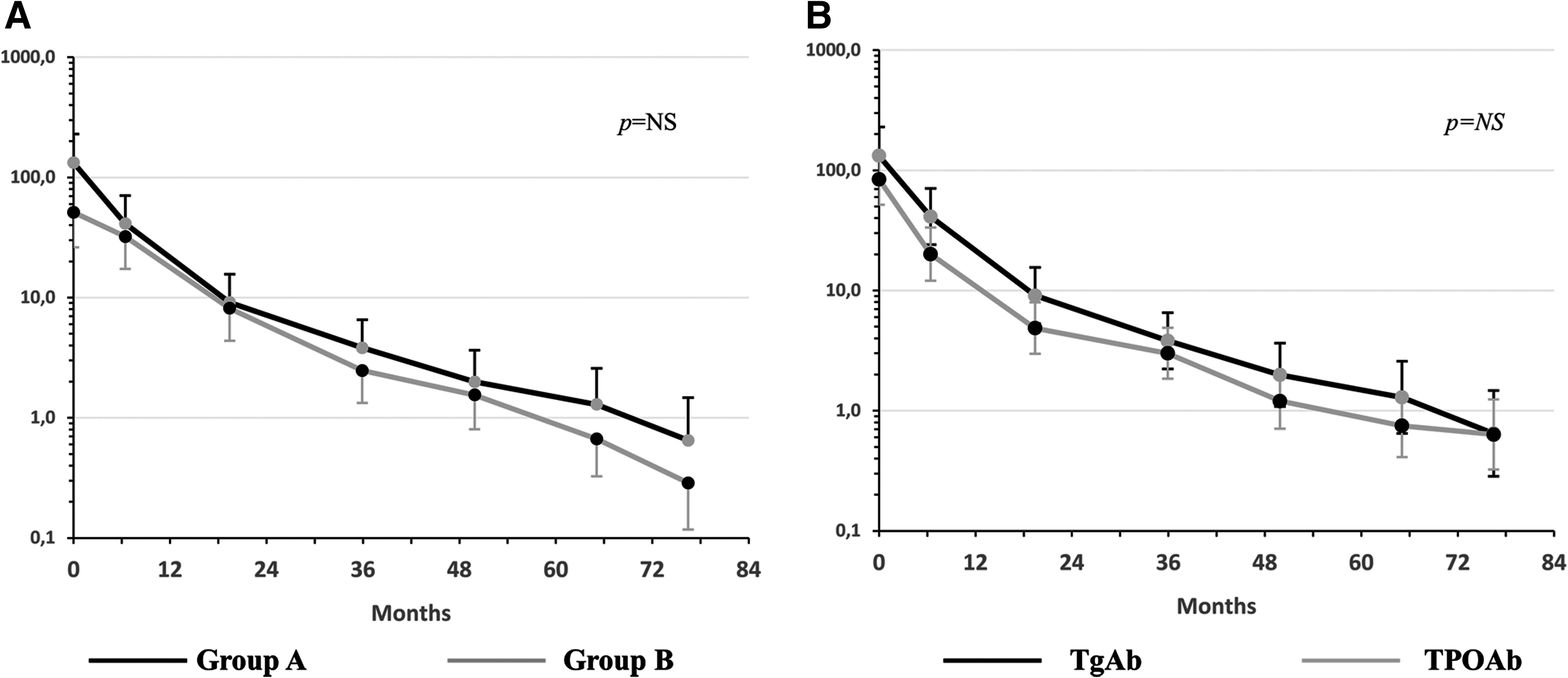
We then distinguished two groups of patients according to TPOAb status at the first postoperative evaluation: group A with positive (>1 IU/mL) TPOAb (TgAb+/TPOAb+; 61/107; 57%) and group B with negative TPOAb (TgAb+/TPOAb–; 46/107; 43%). When the rate of decrease in TgAb over time was compared between these two groups of patients, no statistically significant differences were observed (p = 0.67; Fig. 7A). When comparing only group A with the entire cohort, there was no statistically significant difference between the rates of decrease in both TgAb (−48%/year) and TPOAb (−49%/year; p > 0.05; Fig. 7B).
(
Discussion
Approximately 25% of DTC patients have positive TgAb as a consequence of an associated LT or the immune reaction to thyroid cancer (9,10). In these patients, the role of serum Tg as a tumor marker is severely impaired, and it cannot be used to establish disease status (24). However, it is accepted that the change in serum TgAb levels can be used as a “Tg surrogate” marker, and in particular, they can become undetectable in a median time of approximately three years (15). The most likely explanation of this behavior is that, as in chronic lymphocytic thyroiditis (25), the disappearance of the antigenic stimulus (i.e., the absence of any thyroid tissue) induces a progressive reduction and ultimately a disappearance of thyroid antibody production, although the survival of a substantial fraction of plasma cells can be responsible of a temporary persistence of humoral immunity (26). If this concept is accepted, it is plausible that the persistence or the growth of thyroid tissue—particularly when a lymphocytic infiltration is present—can trigger the immune system to continue or reinitiate the production of thyroid antibodies.
The question of whether the presence of a normal postoperative thyroid remnant could maintain the stimulus for the antibody production, thus affecting the disappearance of the serum TgAb, has not been clarified so far. As a consequence, the positivity of TgAb levels in the follow-up of patients with DTC and positive TgAb treated with TTx but not with RRA represents a matter of concern.
There are studies showing that patients with a >50% reduction of TgAb within one year after TTx and RRA have a very low risk of structural disease (27). In this study, it was observed that although patients were not treated with RRA, both TgAb and TPOAb levels were progressively and continuously decreasing during the follow-up, with an annual decrease rate of 47% for TgAb and 30% for TPOAb. In both cases, the decreasing trend continued over the years, and even if 62.6% became negative (<8 IU/L) at the time of the end of the follow-up (median time from surgery = 6.3 years), the other cases, with the exception of one, were all still stable or decreasing. It is worth noting that a significant decrease in both antibodies was already observed when the levels before and five to six months after TTx were compared. This is not unexpected, since at least in the authors' local experience in a tertiary care center, surgical ablation (i.e., undetectable levels of serum Tg and negative nUS) of patients with low and intermediate risk DTC, is obtained in approximately 30% of patients (28), and this rate of surgical ablation can also be expected in cases with LT, thus explaining the rapid decrease in thyroid antibodies just after surgery. A similar result was observed in a Spanish series in which 27.6% of patients became TgAb negative just one year after TTx (19). It is still unclear why in a few cases TgAb and/or TPOAb levels increased after surgery, as assessed at the first postoperative evaluation. One hypothesis is that the surgical procedure determined a release of thyroid antigens that induced a rise of the autoantibodies (29).
As previously stated, >60% of patients became TgAb negative (<8 IU/mL) during the six years of follow-up, but it is important to note that the time of antibody disappearance was related to the initial levels, since it was clearly observed that the higher the initial level, the longer the time to antibody disappearance. This concept must be taken into account during the follow-up of these patients, and if the postoperative serum TgAb levels are still high, patients and physicians must be aware that while a slow but continuing decreasing should be a good prognostic factor, the time required for TgAb disappearance can be long and of a duration of up to three years after TTx plus RRA (15). In the present series, a level of 61.9 IU/mL at the first control after TTx (i.e., 5–6 months later) can be used as a threshold to predict those patients who will become TgAb negative within six years, in the absence of recurrence. It is important to underline that this numeric value identified by ROC analysis cannot be applied across TgAb methods and is only valid for this assay.
The degree of lymphocytic infiltration is also a predictor of the time of disappearance of the serum antibodies. Cases with higher levels of infiltration degree showed higher levels of antibodies and, as a consequence, a longer time to disappearance of the antibodies compared to those with lower levels. Nevertheless, the rate of disappearance was the same in cases with high or low degree of infiltration. The same phenomenon was observed by Chiovato et al. who showed that changes in TgAb levels were similar in cases with LT, Graves' disease, or focal thyroiditis (15). In this regard, it would be of practical usefulness to have an accurate description of the degree of lymphocytic infiltration in the pathology report to predict the time required for their disappearance.
Not all cases of LT are positive for both TgAb and TPOAb (10,25). Currently, TPOAb are considered the best serological marker for the diagnosis of LT, since they represent the results of a long-time standing immune response, and their levels directly correlate with the degree of lymphocytic infiltration and with the development of hypothyroidism (30). Conversely, TgAb are related to an early immune response and often are the ones present at disease onset (31,32). The question of whether the presence of TPOAb could influence or interfere with the rate of decrease in TgAb levels seemed reasonable. However, according to previous data obtained in ablated patients (15), in the present series, it appeared that neither the time nor the rate of disappearance of TgAb was affected by the presence of TPOAb, and that when both are present in the same patient, the rate of decrease is similar to that of the entire group, including cases positive for each one or the other.
Among 107 patients of this series, there was no structural nUS recurrence during follow-up, in agreement with both the low level of risk of these cases and the decreasing levels of the TgAb. The only observed exception was a patient with rising TgAb levels that anticipated the detection of new thyroid tissue in the thyroid bed that had not previously described at nUS. The FNAC demonstrated that this was benign thyroid tissue with lymphocytic infiltration. This case confirms the positive predictive role of the TgAb levels increasing, which was well demonstrated by Yamada et al. in a large series of patients with DTC and positive TgAb (18). They observed that when the trend of TgAb level was increasing, according to the higher or lower rate of increase, the prognosis of the cases was more or less severe. In the present case, the newly detected tissue in the thyroid bed was benign tissue with lymphocytic infiltration, supporting the concept that the presence of thyroid tissue is required to sustain TgAb production and that its reappearance or enlargement promotes a larger TgAb production. To the authors' knowledge, this is the first case of a significant rise of TgAb linked to the reappearance of benign thyroid tissue in a subject treated and followed for PTC. It is worth noting that a massive lymphocytic infiltration was present in the recurrent tissue. As previously stated, TPOAb represent the best serological marker of LT, and for this reason they were also expected to reappear in this case. Unfortunately, we do not have the correspondent values of TPOAb since during the follow-up of DTC patients, as standard of care, we measure only TgAb because of their interference in the measurement of serum Tg. The question of whether the increase in TgAb alone reflects the recurrence of an autoimmune process rather than of a “truly normal” or malignant thyroid tissue cannot be answered and deserves further studies.
The group of patients studied (i.e., unifocal microPTC) will often not be treated with TTx anymore. However, this group represented a good example of thyroidectomized but not 131I ablated patients with a follow-up long enough to study the trend of thyroid antibodies. It is felt that the results obtained in this study can also be applied to cases with bigger tumors for which TTx is the first choice treatment, but is not necessarily followed by RRA (6).
In conclusion, this study demonstrates that TgAb levels decline in the majority of DTC patients treated with TTx but not ablated with 131I. The levels decrease rapidly after the surgical treatment and continue to decrease over time. The time of disappearance is influenced by the initial TgAb levels and by a higher degree of lymphocytic infiltration. No influence of the TPOAb levels has been observed. Additionally, as happens in ablated patients, an increase in TgAb levels should not be overlooked, since it can indicate the presence or reappearance of either normal or cancerous thyroid tissue.
Footnotes
Acknowledgments
A.M. contributed to this paper as recipient of the PhD program in Clinical and Translational Science of the University of Pisa. We would like to thank Ministero dell’ Istruzione, dell’ Università e della Ricerca (MIUR, investigator grant 2015 project code PRIN 2015HPMLFY) for the continuing research support.
Author Disclosure Statement
The authors have nothing to disclose.