
Abstract
Background:
A longitudinal study was conducted in full-term healthy infants who were born between 2015 and 2017 in Athens, Greece, to elucidate the evolution of thyrotropin (TSH) and other thyroidal parameters according to sex, from their day of birth until two years old. Other thyroidal parameters that were taken into account include antithyroid peroxidase antibody (TPO-Ab) and antithyroglobulin antibody (TG-Ab), total triiodothyronine (T3), and free triiodothyronine (fT3), along with total thyroxine (T4) and free thyroxine (fT4).
Methods:
Blood samples were taken at 5-day intervals from the day of birth until the 31st day of life, and then every 5th month until 2 years of age. All thyroid parameters were measured by electrochemiluminescence immunoassays. The study took place at the Iaso General, Maternity and Gynecological Clinic in Athens, Greece.
Results:
The sample consisted of 2916 full-term healthy neonates/infants: 1507 (51.7%) boys and 1409 (48.3%) girls. There were no significant differences in TSH levels between boys and girls in all time periods from birth up to 2 years except between 11 and 15 months of age (p = 0.038). Mean TSH levels for boys exhibited much more fluctuation and variability than for girls. In boys we found a significant association between TSH levels and fT4 (p < 0.001), while we found a significant association between TSH levels and T3 in girls (p = 0.045). Furthermore, we found that mean TPO-Ab and TG-Ab levels for boys exhibited larger variability than those for girls.
Conclusions:
In this study, we were able to plot the development of TSH and other thyroidal parameters by sex from birth up to two years of age. In terms of clinical practice, our findings suggest the need for a re-evaluation of the reference ranges of the studied parameters according to sex, especially in the first months of life and until the first year. Furthermore, our results suggest new optimal ranges for thyroid hormone replacement for that specific period.
Introduction
Thyroid hormones have a vital role in physical growth, differentiation, and brain maturation during fetal and postnatal life (1). The mammalian brain is a direct target organ of thyroid hormones, both during development and during adulthood (2). Although thyrotropin (TSH) regulates the synthesis and secretion of thyroid hormones, a number of important extrathyroidal processes adjust the circulation of thyroid hormones within a relatively narrow concentration range (2,3). Even though embryogenesis of the hypothalamus and pituitary and thyroid glands in the human fetus is largely completed by the 12th week of gestation, differentiation and functional maturation of the hypothalamus, pituitary, and thyroid glands continue into the neonatal period (4).
Experimental and clinical data have had an impact on the understanding of the maturation pattern of the hypothalamic–pituitary–thyroid system from the intrauterine fetus to postnatal age (5). The net effect of this ongoing maturation is reflected in the pattern of change in the prevailing serum thyroid parameters.
Concerning sexual dimorphism, human males and females are known to undergo development at different rates, both in utero and postnatally up until the postpubertal stage (6). In particular, male fetuses are known to grow faster than females. It has been stated that a sex difference in developmental timing is worthy of consideration in the design of clinical studies and that the sexes should be treated by researchers as separate models (7).
The purpose of this study was to investigate the evolution of TSH and other thyroidal parameters according to sex in full-term healthy infants from day of birth until age two years, in Athens, Greece. Other thyroid hormone parameters that were determined included antithyroid peroxidase antibody (TPO-Ab) and antithyroglobulin antibody (TG-Ab), total triiodothyronine (T3), and free triodothyronine (fT3) along with total thyroxine (T4) and free thyroxine (fT4).
Materials and Methods
Our study took place in Iaso General, Maternity and Gynecological Hospital in Athens, Greece, and includes all babies who were born at Iaso between 2015 and 2017. All newborns were from normal pregnancies without any prenatal complications and an Apgar score of >7 in the first minute of birth. Specifically, the inclusion criteria were (i) gestational age (GA) between 37 and 42 weeks, and appropriate weight, height, and head circumference for the GA; (ii) mothers with normal thyroid function; and (iii) no significant perinatal morbidity (defined as discharge before 8 days of life). Infants who fulfilled at least one of the following criteria were excluded from the study: (i) major congenital malformation; (ii) genetic abnormalities; (iii) intrauterine growth retardation; (iv) diagnosis of congenital hypothyroidism (CH) by neonatal screening; and (v) mothers taking medication that affects thyroid function such as T4, corticosteroids, dopamine, propranolol, propylthiouracil, methimazole, or alpha interferon; or (vi) mothers diagnosed with any pituitary disease.
The final sample included 2916 infants. Levels of TSH, T3, F3, T4, fT4, TPO-Ab, and TG-Ab were measured from the day of birth until the 31st day of life at 5-day intervals, and afterward every 5th month until 2 years of age. Written informed consent was obtained from all parents for the authorized use of their medical records for research purposes. The study was conducted in compliance with all the principles of the Declaration of Helsinki and it was approved by the ethical committee of the Iaso Hospital.
Laboratory measurements
To separate the serum from the cells, we centrifuged the clotted blood samples that were taken by venipuncture from all subjects. Samples were stored at a temperature of −70°C until assayed. All thyroid diagnostics were determined using electrochemiluminescence immunoassay on a Cobas 601 immunoassay analyzer by Roche.
Statistical analysis
Quantitative variables are presented as median and interquartile range, whereas categorical variables are presented as absolute and relative frequencies (%). The Mann–Whitney test was used to compare the median TSH values between boys and girls in each age group. Pearson's chi-square exact test was used to compare the percentage of boys and girls with values of TSH <0.5 or >4.5 or >10 μIU/mL by age group. To investigate the functional form of the relationship of TSH with the age of the children, we used additive mixed effects models; such models allow for an unspecified nonlinear effect of age on TSH by sex, while adjusting for the repeated measurements of the subjects. T3, T4, fT3, fT4, TPO-Ab, and TG-Ab were successively included in these models to identify relationships with TSH levels, after adjusting for age, for all data and separately by sex. Finally, to investigate how TPO-Ab and TG-Ab change over time, we used additive mixed effects models with each of these hormones as the dependent variable, respectively, allowing for a different smooth term of age by sex.
Two-tailed p-values <0.05 were considered statistically significant, after adjusting for multiple comparisons using Bonferonni corrections. All analyses were performed in RStudio (RStudio Team [2016]; RStudio: Integrated Development for R. RStudio, Inc., Boston, MA) using the library mgcv and in IBM SPSS v. 23 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0.; IBM Corp., Armonk, NY).
Results
The sample consisted of 2916 full-term healthy infants from birth to 24 months of age. Of these, 1507 (51.7%) were boys and 1409 (48.3%) were girls. Tables 1 and 2 present the descriptive statistics for the thyroidal parameters of interest by sex.
Descriptive Statistics for the Thyroidal Parameter Levels, in Boys
SD, standard deviation; T3, total triiodothyronine; fT3, free triiodothyronine; T4, total thyroxine; fT4, free thyroxine; TSH, thyrotropin; TPO-Ab, antithyroid peroxidase antibody; TG-Ab, antithyroglobulin antibody.
Descriptive Statistics for the Thyroidal Parameter Levels, in Girls
Tables 3 and 4 present the TSH levels by age group for boys and girls, respectively. According to our data, TSH for boys started at a median value of 7.03 μIU/mL and decreased to 4.17 μIU/mL at 31 days and further decreased to 3.02 at 2 years of age. For girls, TSH levels started at a median value of 5.26 μIU/mL and decreased to 3.92 at 31 days and to 2.96 at 2 years of age. It is interesting to note that approximately half the infants had TSH levels >5 μIU/mL the first 5 days after birth. This fell to 25% for boys and 10% for girls after 1 month and further to 7.5% and 1.4% for boys and girls, respectively, after 20 months. As shown in Tables 3 and 4, median TSH levels did not differ significantly between the two sexes at all age groups for all age groups. Similarly, the percentages of children with TSH levels <0.5 μIU/mL, >4.5, or >10 μIU/mL did not differ significantly between the two sexes, at all age groups.
Descriptive Statistics of the Thyrotropin Levels (μIU/mL) in Boys, by Age Group
N, number of boys.
% of boys with TSH levels <0.5 μIU/mL.
% of boys with TSH levels >4.5 μIU/mL.
% of boys with TSH levels >10 μIU/mL.
Descriptive Statistics of the Thyrotropin Levels (μIU/mL) in Girls, by Age Group
N, number of girls
% of girls with TSH levels <0.5 μIU/mL.
% of girls with TSH levels >4.5 μIU/mL.
% of girls with TSH levels <10 μIU/mL.
Mann–Whitney tests comparing the median TSH levels between boys and girls of the same age group were all nonsignificant.
Chi-square tests comparing the percentage of boys versus girls of the same age with TSH levels <0.5 μIU/mL were all nonsignificant.
Chi-square tests comparing the percentage of boys versus girls of the same age with TSH levels >4.5 μIU/mL were all nonsignificant.
Chi-square tests comparing the percentage of boys versus girls of the same age with TSH levels >10 μIU/mL were all nonsignificant.
Figure 1 presents the estimated curve for the relationship between TSH levels and age of the children by sex from our additive mixed effects models. For boys, mean TSH levels were lower at birth than those for girls, then approximately at 3 months of age they increased and up to ∼18 months old they were higher than mean TSH levels for girls. From 18 to 24 months, mean TSH levels for boys and girls were very similar. Also, the TSH curves for girls and boys exhibit similar variability.
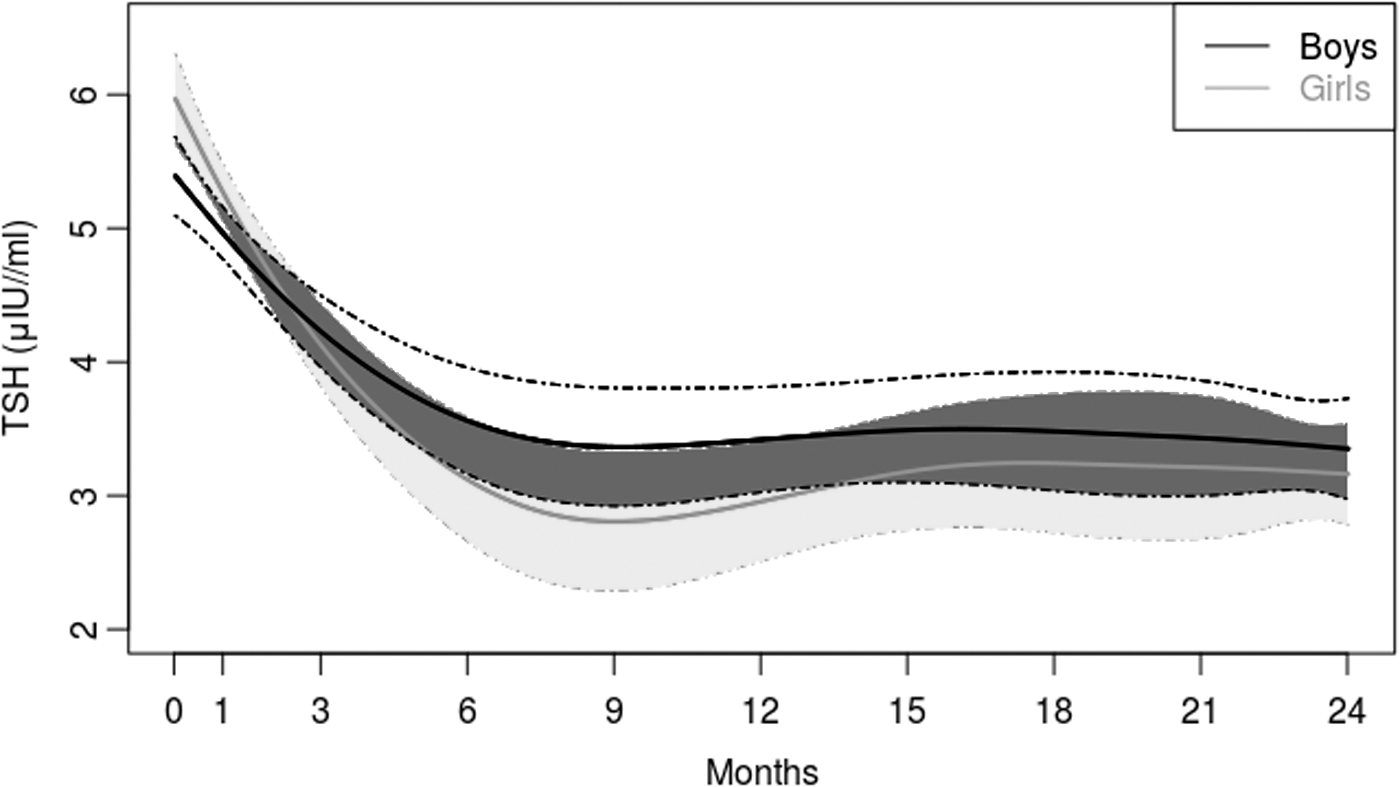
Mean TSH levels (μIU/mL) by age for boys (black line) and girls (gray line): results from the additive mixed model that adjusts for a nonlinear effect of age on TSH. Light gray region and medium gray region correspond to the 95% pointwise CI for mean TSH levels in boys and girls, respectively. Dark gray area denotes the intersection between the CIs of boys and girls. CI, confidence interval; TSH, thyrotropin.
Table 5 presents the results for the relationship between TSH levels and other thyroid hormone parameters by sex, after adjusting for the nonlinear effect of the age of the children in the additive mixed effects models. For boys, fT4 was significantly associated with TSH levels (p < 0.001). For girls, the results were statistically significant only for T3 (p = 0.045), revealing a positive association.
Results from the Additive Mixed Effects Models on Thyrotropin That Adjust for a Nonlinear Effect of Age
The models are stratified by sex and the thyroid hormone parameters were added in the model separately (i.e., one parameter at a time).
Statistically significant results.
SE, standard error.
For boys, the median TPO-Ab levels were 10 IU/mL, while for girls median levels were 11 IU/mL. Similarly, median TG-Ab levels for boys were 15 IU/mL, while they were 14 IU/mL for girls. For TPO-Ab (Fig. 2), the results from the additive mixed effects models showed that mean levels of TPO-Ab started at much larger values for boys than for girls, and then approximately between the third and fourth months, mean TPO-Ab levels became equal for both sexes. Moreover, as shown in Figure 2, mean TPO-Ab levels for boys exhibited much larger variability than those for girls. Results for TG-Ab are shown in Figure 3: for girls, the relationship between mean TG-Ab and age was almost linear, with a negative slope. For boys, we observed much larger fluctuation in mean TG-Ab levels than those in girls. Also, as in TSH and TPO-Ab, the observed variability for mean TG-Ab was larger in boys than in girls.
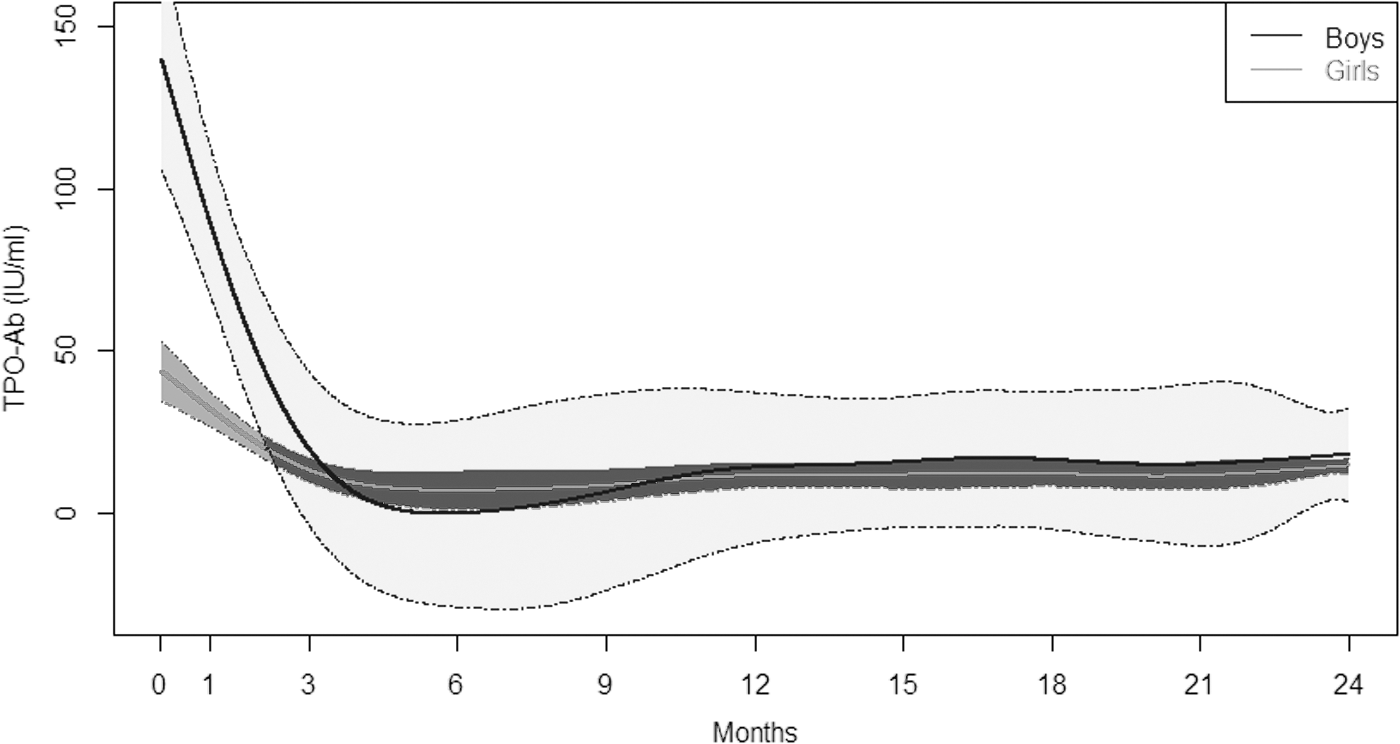
Mean TPO-Ab levels (IU/mL) by age for boys (black line) and girls (gray line): results from the additive mixed model that adjusts for a nonlinear effect of age on TPO-Ab. Light gray region and medium gray region corresponds to the 95% pointwise CI for mean TPO-Ab levels in boys and girls, respectively. Dark gray area denotes the intersection between the CIs of boys and girls. TPO-Ab, antithyroid peroxidase antibody.
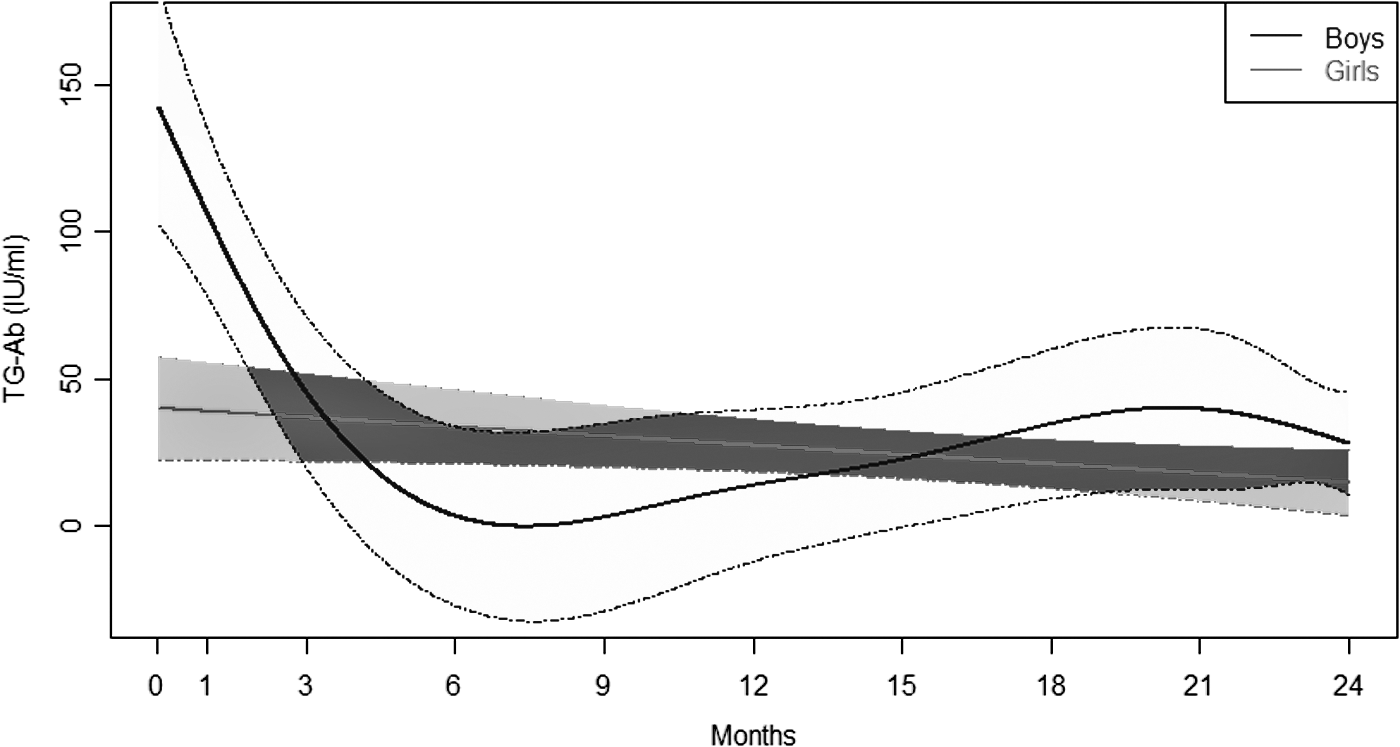
Mean TG-Ab levels (IU/mL) by age for boys (black line) and girls (gray line): results from the additive mixed model that adjusts for a nonlinear effect of age on TG-Ab. Light gray region and medium gray region correspond to the 95% pointwise CI for mean TG-Ab levels in boys and girls, respectively. Dark gray area denotes the intersection between the CIs of boys and girls. TG-Ab, antithyroglobulin antibody.
The pattern for the mean T3 levels (Supplementary Fig. S1) was almost identical for boys and girls: mean T3 started from very low levels at birth, rose until approximately the fourth and fifth month, and then followed an almost linear relationship with age, with a negative slope. The relationship between mean T4 levels and time (Supplementary Fig. S2) was linear for both sexes, and the difference in the slopes was not statistically significant (p > 0.05).
Discussion
We investigated the progression of TSH and other thyroidal parameters over time and by sex, in full-term healthy neonates and infants up to two years of age in Athens, Greece. We show that in all periods from birth up to two years, there were no significant differences in TSH levels between boys and girls. Moreover, we show that mean TSH levels for boys and girls exhibited similar variability. We found significant positive association between TSH and fT4 levels in boys, and between TSH and T3 levels in girls. Finally, we investigated, by sex, how the levels of other thyroid parameters change over time. To the best of our knowledge, this is the first longitudinal study with the aim of elucidating the evolution of thyroid function parameters in both sexes in full-term healthy newborns and infants, in a distinct sampling scheme from birth up to 24 months old and in a large sample. In addition, as far as we are aware, such a detailed timing protocol for a newborn screening sampling had not previously been applied to any population worldwide.
In humans, healthy thyroid function is a prerequisite for normal growth and mental and physical development. According to numerous clinical studies, the reference range values of thyroid function tests depend on age, sex, method of analysis and ethnicity, various medications, and clinical conditions (8, 9, 10). To this end, our study provides reference ranges and plots the longitudinal development of thyroid parameters examined by sex for full-term healthy newborns and infants up to two years of age.
Thyroid disease in children is well known to be associated with impaired physical and cognitive development. According to the American Thyroid Association, TSH levels are considered the most sensitive parameter for diagnosing hyperthyroidism and hypothyroidism and for monitoring thyroid replacement therapy, because of their high sensitivity. fT4 levels are also essential, since they directly reflect hormone production by the thyroid gland (11), and fT3 serum concentration appears to influence the onset of puberty (12). In our study, we focused on TSH levels and their relationship with other thyroid parameters.
Optimization of TSH borderline cutoff points is critical, since it ensures that true cases of CH are not missed. Although efforts have been made to optimize these points, there is still controversy regarding this issue. To reduce the false positive and recall rates and to minimize the false negative rate, each country defines a conservative TSH cutoff point for its CH screening protocol. On the basis of several reports, TSH levels between 5 and 20 μIU/mL are used as screening cutoff points in various regions (10,13). In Greece, the newborn screening program for CH was initiated in 1979 (14) and was gradually generalized to cover the total newborn population. Initially a blood spot TSH value of 30 μIU/mL was used as a cutoff point and eventually this was lowered to 20 μIU/mL in the 1990s, following the recommendations of the European Society of Pediatric Endocrinology (15). In 2010, Mengreli et al. (16) called for a modification of the screening methodology and follow-up, since they found that a significant number of cases with permanent CH are missed when a TSH threshold of 20 mU/L is applied.
According to our results, TSH concentrations were >5 μIU/mL in the first 5 days after birth in approximately half of our infant population, and then fell to 25% for boys and 10% for girls after 1 month and further to 7.5% and 1.4% for boys and girls, respectively, after 20 months. Our results show an overall inverse relationship between age and serum TSH concentration for both sexes during the study period, and a similar pattern of TSH progression was recorded for boys and girls. Moreover, we observed a similar variability in the mean TSH levels in both sexes. As also reported in developmental clinical studies, our findings can be attributed to slower neural maturation occurring in boys (17) or to undefined biological or environmental/cultural factors. Nevertheless, given the equivalence in anthropometric indicators of growth between boys and girls, these findings most probably support the long-standing notion that girls are more mature than boys at birth (18).
Several neonatal screening programs and studies performed worldwide obtained similar results (10,19 –22). Specifically, a cross-sectional study conducted in Iran on 246 healthy term neonates aged between 2 days and 1 month showed that serum TSH was inversely correlated with age, especially after 7th day of life (10). Mean serum TSH concentrations were significantly higher in newborns of 5–14 days in than in those aged >2 weeks, in which a decline in serum TSH level starts, in agreement with our results. Moreover, there was a significant negative correlation between age and serum TSH concentration, T4, and fT4. Najam et al. (20) stated that the decline in TSH and T4 levels was more pronounced in the first week, and in a study of 5817 patients aged from 1 month to 20 years, Zurakowski et al. (21) also showed an inverse association between age and the mean serum levels of T3, TSH, and free T4. In contrast, Mansourian et al. (22) reported no association between age and serum TSH and T3 levels in a study conducted in Iran on a sample of children between 1 and 21 years of age. Nevertheless, the authors (22) found an inverse association between serum T4 and age.
To determine reference intervals for TSH and fT4 levels, blood samples were taken from 1639 neonates at a university teaching hospital in Nairobi, Kenya (23). This study also established a decline in TSH and fT4 levels with an increase in age, with a lower reference interval of TSH for female neonates (23).
In terms of sex differences, Mansourian et al. (22) also reported higher levels of TSH and T3 and lower T4 in girls, although these results were not significant. Kapelari et al. (9) found no significant sex differences in the distribution of thyroid hormone levels except for T3, which was higher in boys. Furthermore, Mutlu et al. (19) detected no sex difference in the serum hormone levels of 296 Turkish newborns from birth to 28 days of age. In contrast, Zurakowski et al. (21) reported a more rapid decline in serum TSH and T3 levels with age and a higher level of total T4 in females than in males, with no sex difference in free T4 levels. These differences were assumed to be caused by discrepancies in ethnicity, sample size, laboratory material, and methods used (24). In our study, the statistically significant association of TSH with T3 levels in girls can be attributed to adequate upregulation of type 2 deiodinase activity, known to occur in girls (25).
It is of interest that the observed variability for mean TPO-Ab and TG-Ab levels was larger in boys than in girls in the first months of life. Data from epigenetic studies suggest that sexually dimorphic genes contribute to immune-related differences between males and females (26). Clinical studies using immunophenotyping of blood lymphocytes showed a trend toward having a higher percentage of lymphocyte subsets in female, with the absolute counts of lymphocyte subsets peaking during the first year and then steadily decreasing with age (27). In addition, although clinical studies reported positive correlations between maternal thyroid hormones and thyroid function of offspring, they did not find any correlation between maternal thyroid hormones and autoantibodies in the offspring (28). Other studies reported a positive correlation between TPO-Ab titers done in mothers during pregnancy and samples obtained in newborn at 48 hours of life (29). Furthermore, no effect of maternal TPO-Ab titers on the thyroid function of the infants could be detected. Previous studies have shown that the incidence of subclinical hypothyroidism is rather high during early pregnancy and that positive TPO-Ab values have predictive value on the thyroid dysfunction of the mother (29,30).
In our sample, all babies were born at Iaso General, Maternity and Gynecological Hospital in Athens, Greece, which is one of the major private gynecological hospitals in Athens. In Greece, ∼61.6% of women gave birth in private hospitals between January 2013 and August 2015, and this percentage is even higher in Athens (31). Therefore, our sample is characteristic for the Greek neonate population. Nevertheless, the fact that our sample comes from a specific private gynecological hospital in Athens and no data are included from public hospitals is a limitation of this study. Another limitation is that we do not have information which children later developed hypothyroidism. If information was available (e.g., longer follow-up) on which children later developed hypothyroidism, we would have excluded these children from the analysis and would have studied only the healthy children population in terms of thyroid function.
In population studies like ours, differences in thyroidal parameter levels are usually assumed to be due to different characteristics of the analytical methods used, and variability in ethnicity, sample size, or unknown geographic covariates. However, divergence observed in thyroid hormone maturation pattern between boys and girls in our longitudinal study might reflect differences in the maturation of the hypothalamic–pituitary–thyroid axis. In terms of clinical practice, our findings suggest a need for re-evaluating the reference ranges of thyroid parameters according to sex, especially in the first months of life and until the first year. Furthermore, our results suggest new optimal ranges for thyroid hormone replacement for that specific period.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.