
Abstract
Background:
An increase in the incidence of congenital hypothyroidism (CH) with a normally located gland has been reported worldwide. Affected individuals display transient or permanent CH during follow-up in childhood. This study aimed to determine the prevalence of transient CH and to investigate the possibility of distinguishing between transient and permanent CH in early infancy.
Methods:
This observational cohort study included all patients identified by systematic neonatal screening for CH in the northern Parisian region between 2002 and 2012 and treated for CH with a normally sited gland. A standardized data collection form was completed prospectively at diagnosis. Patients were classified during follow-up as having transient or permanent CH.
Results:
Of the 92 patients initially treated for CH with a normally located gland during the neonatal period, 49 (54%) had a transient form of CH after the cessation of levothyroxine (LT4) treatment at 1.5 (0.6–3.2) years of age. Multivariate analysis revealed that transient CH was associated with a lower likelihood of having a first-degree family history of CH (p = 0.03) and a lower LT4 dose at six months of age (p = 0.03) than permanent CH. Sex, ethnicity, neonatal problems (e.g., prematurity, being small for gestational age, and/or neonatal distress), iodine status, coexisting malformations, initial CH severity, and thyroid morphology at diagnosis had no effect. Receiver operating characteristics curve analysis showed that a cutoff of 3.2 μg/kg/day for LT4 dose requirement at six months of age had a sensitivity of 71% and a specificity of 79% for predicting transient CH, with values below this threshold considered predictive of transient CH.
Conclusion:
In patients with CH and a normally located gland, these findings highlight the need to evaluate LT4 dose requirements early, at six months of age, particularly in patients with no family history of CH, for early identification of the approximately 50% of patients for whom treatment should be stopped.
Introduction
A
According to current guidelines, children with CH and a eutopic gland should undergo a re-evaluation of thyroid function at or before three years of age in order to distinguish between cases of transient and permanent CH (21). Over the last 15 years, the prevalence of transient hypothyroidism detected through newborn screening programs has been reported to range between 17% and 65% (4,11,14 –17,19,22 –32). At the authors' screening center in the Parisian region, an increase in the prevalence of the transient form has been seen from 38% in patients born before 2002 to 50% in patients born during the 2005–2008 period (33,34).
The etiology of CH with a eutopic gland remains elusive, and the factors driving its clinical diversity are largely unknown. Neonatal transient hyperthyrotropinemia is generally easily attributed to iodine overload or to the passage of antithyroid antibodies or antithyroid drugs across the placenta (33). No clear effect of borderline moderate iodine deficiency on neonatal thyroid function was found in the catchment area in the northern Parisian region (35), and the incidence of patients with CH and a eutopic gland does not differ significantly between French regions (7). A role for factors other than known dyshormonogenesis-associated genetic variants or TSH receptor gene variants cannot be excluded, and the possible effects of environmental agents toxic to the fetal and neonatal thyroid gland, such as bisphenols, are currently being investigated (36,37).
The early identification of patients with transient as opposed to permanent CH has a number of important implications relating to levels of parental anxiety, expense, and potential chronic overtreatment, which has been shown to be associated with poorer neurodevelopmental outcomes (38). This regional cohort study investigated the current prevalence of transient hypothyroidism in patients initially treated for CH with a eutopic gland, with the aim of identifying clinical characteristics that can be used for the very early prediction of outcomes.
Methods
Patients
This observational cohort study included all patients identified through systematic neonatal screening for CH in the northern Parisian region between 2002 and 2012 and treated for CH with a normally sited gland. During this period, 240 patients with CH were identified in the screening program: 110 had thyroid dysgenesis (athyreosis, n = 34; ectopic thyroid, gland n = 76), and 130 (54%) had a normally located thyroid gland. The inclusion criteria for the study were: use of the same procedure for CH screening during the study period based on TSH measurement and the threshold used in the laboratory (34), treatment with levothyroxine (LT4) started during the neonatal period, and patient at least three years old at the time of the study. The exclusion criteria were: absence of LT4 treatment (neonatal transient hyperthyrotropinemia resolving in the first month of life, n = 31), patient lost to follow-up (n = 5), and death of the patient (n = 2). In total, 92 patients treated for CH with a normally located gland were included in the study (Fig. 1). Patients were a median (25th–75th percentile) of 19 (10 –25) days old at treatment initiation, with median TSH and free thyroxine (fT4) concentrations of 69 mIU/L (35–230 mIU/L) and 12.8 pmol/L (7.3–15.7 pmol/L), respectively. The median initial dose of LT4 was 8.4 μg/kg/day (6.5–10.0 μg/kg/day).
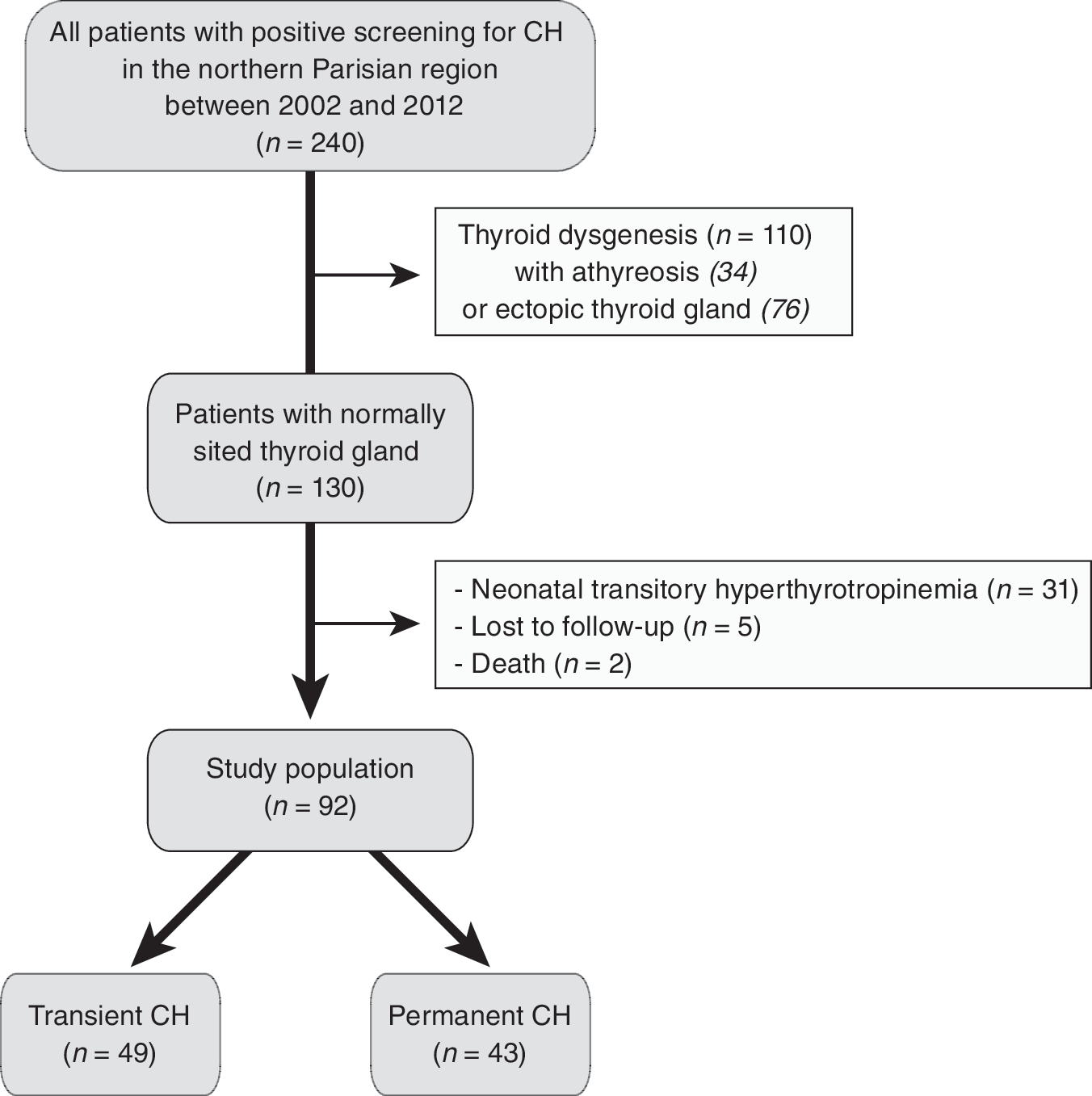
Flow chart of the study.
Study protocol
Clinical data for each patient were obtained from the standardized data collection forms completed prospectively at the time of diagnosis and from the medical data recorded at each evaluation. The following data were recorded at diagnosis: sex; perinatal parameters and events such as gestational age, birth weight, birth length, mode of delivery, and neonatal distress (Apgar score <7 or neonatal resuscitation, infection, respiratory or neurological distress, or requirement for neonatal intensive care); and neonatal history, including iodine overload, ethnicity, consanguinity, biochemical thyroid parameters, bone maturation, and the results of thyroid ultrasonography and thyroid scintigraphy, with a perchlorate discharge test performed at CH diagnosis. The presence of associated malformations or dysmorphic features or of a first-degree family history of CH was recorded at diagnosis and during follow-up.
Patients underwent a physical examination at baseline and at subsequent visits, with biochemical parameters (TSH and fT4) checked after 15 days, every one to two months until six months of age, and two to three times per year thereafter. The management of LT4 treatment during follow-up, total LT4 treatment duration, clinical and laboratory test results, and outcomes were recorded. In France, all pediatricians prescribe a preparation of LT4 in solution until the patient is 6–12 months old, after which this treatment is replaced by LT4 tablets. Pediatricians did not follow a particular study protocol for the timing of thyroid function reassessment. Such reassessments were therefore performed at various times during follow-up in patients with inadequate treatment or following the decrease or cessation of treatment.
LT4 dose was adjusted in accordance with established recommendations (21). Patients were considered to have a permanent form of CH if serum TSH concentrations were ≥7 mIU/L after the age of six months either spontaneously on treatment or after LT4 treatment was decreased or stopped. Transient CH was defined as serum TSH concentrations <7 mIU/L at least four weeks after LT4 was stopped. All decisions concerning the management of LT4 treatment were made on an individual basis.
The study protocol was approved by Robert Debré Hospital, Paris 7 University, Assistance Publique Hôpitaux de Paris Ethics Review Committee for Biomedical Research Projects (CEERB No. 2016/319). Informed consent was obtained from the parents.
Methods
Prematurity was defined as birth before a gestational age of 37 weeks. Birth weight and length are expressed as standard deviation score (SDS) for sex and gestational age, and small for gestational age (SGA) was defined as a birth length and/or weight ≤ −2 SDS. Children were classified as Caucasian or non-Caucasian (African, Asian, and Caribbean) based on the geographic origin of their parents. Iodine overload was defined as a positive history of iatrogenic iodine overload and/or high urinary iodine concentration (>2400 nmol/day).
The severity of hypothyroidism was determined by assessing serum fT4 concentration at diagnosis (<5, 5–9.9, ≥10 pmol/L) and bone maturation delay, evaluated at diagnosis by X-ray assessment of the epiphyseal ossification centers of the knee (distal femoral and proximal tibial ossification centers absent, or at least one present) (21). The size of the thyroid gland was estimated by clinical examination and by measurement on an ultrasound scan at diagnosis, with classification as normal, hypoplastic (including hemithyroid), or goiter. Thyroid scanning (123I) was performed before treatment, and a discharge of >10% of 123I dose two hours after the administration of perchlorate (positive perchlorate discharge test) was considered to indicate an organification defect (21). LT4 dose is expressed in μg per kg per day.
Neonatal screening for CH was based on whole-blood TSH determinations on dried blood samples collected on filter paper at the age of four (three to four) days (range 2–22 days) as a primary marker, and TSH concentration determined by immunofluorimetry (DELPHIA; Perkin Elmer, Turku, Finland), with a cutoff at 15 mIU/L during 2002–2012. Serum TSH and fT4 concentrations were determined in competitive immunoassays by direct chemiluminescence or fluorescence depolarization.
Statistical analysis
Data are expressed as medians (25th–75th percentiles) for continuous variables or numbers (percentage) for categorical variables. For comparisons of the characteristics of the two outcome groups of patients (permanent vs. transient), two-tailed Wilcoxon tests were used for quantitative variables, and chi-square tests were used for categorical variables. No adjudication was performed for missing data. A multiple logistic regression model was used to investigate the association between outcome group (permanent vs. transient CH) and other clinical variables: sex, prematurity, SGA, neonatal problems, the presence or absence of associated malformation/syndromic features, iodine overload, first-degree familial history of CH, serum TSH concentrations at diagnosis, CH severity based on serum fT4 concentration or bone maturation delay at diagnosis, thyroid morphology (three categorical groups: normal, hypoplastic, or goiter), and dose of LT4 at treatment initiation and at six months of age. Ethnicity, consanguinity, and the result of a perchlorate discharge test (positive or negative) were not included in the model due to limited data availability. For the same reason, patients were considered to have “a neonatal problem” for the purposes of this analysis if they were born premature and/or were SGA and/or had suffered neonatal distress. LT4 dose at 12 months of age was not included in the model due to its interaction with LT4 dose at six months of age. In the multivariate analysis, variables independently correlated with outcome were included at the p < 0.20 level in univariate analysis. Statistical analysis included the plotting of a receiver operating characteristic (ROC) curve and determinations of sensitivity and specificity from this curve.
Statistical significance was defined as p < 0.05. Analyses were conducted with SAS v9.4 (SAS Institute, Inc., Cary, NC).
Results
In total, 49 (54%) of the 92 patients initially treated for CH during the neonatal period had a transient form of CH. For these patients, LT4 treatment was discontinued at a median age of 1.5 (0.6–3.2) years. The characteristics of the 92 patients at the time of CH diagnosis are provided in Table 1 according to the transient or permanent nature of their CH. Patients with transient forms of CH were more likely than the patients with permanent forms to have smaller increases in serum TSH concentrations at diagnosis and to start LT4 treatment later during the first month of life, with lower doses of LT4 dosage initially and at 6 and 12 months of age. The two groups were similar in terms of ethnicity, but patients with transient forms of CH were less likely to have familial forms of CH, to be the offspring of consanguineous parents, and to have positive perchlorate test results than patients with permanent forms of CH.
p-Values <0.05 are shown: a p < 0.05; b p < 0.02; c p < 0.01; d p < 0.001. Data are n (%) or median (25th–75th percentiles).
Familial CH: all but one of the affected relatives were siblings (the affected relative was the mother in the remaining case).
CH, congenital hypothyroidism; SDS, standard deviation score; SGA, small for gestational age; TSH, thyrotropin; fT4, free thyroxine; LT4, levothyroxine.
A logistic regression analysis was performed on clinical variables in order to identify factors predictive of a transient form of the disease (Table 2). In the multiple logistic regression model, transient CH remained significantly associated with both family history of CH and LT4 dose at six months of age. These variables were the strongest independent predictors of the course of the disease. Patients with transient CH were less likely to have a familial form of CH and tended to have lower doses of LT4 at six months of age than those suffering from permanent CH (p < 0.03). Sex, being born SGA, having neonatal problems, associated malformation, iodine overload, CH severity as assessed by serum TSH and fT4 levels or bone maturation delay at diagnosis, and thyroid gland morphology were not associated with the course of the disease. Ethnicity, consanguinity, and the results of perchlorate discharge tests were not analyzed due to limited data availability.
Statistically significant values are shown in bold.
OR, odds ratio; CI, confidence interval.
As shown by the ROC curves in Figure 2 (area under the ROC curve: 0.83 [confidence interval (CI) 0.75–0.92] at six months, and 0.82 [CI 0.72–0.92] at 12 months), the optimal cutoff values for LT4 dose at 6 and 12 months of age for the individual prediction of transient CH were 3.2 μg/kg/day and 2.5 μg/kg/day, respectively, with a sensitivity of 71% for both time points and a specificity of 79% and 78% for LT4 dose at 6 and 12 months, respectively.
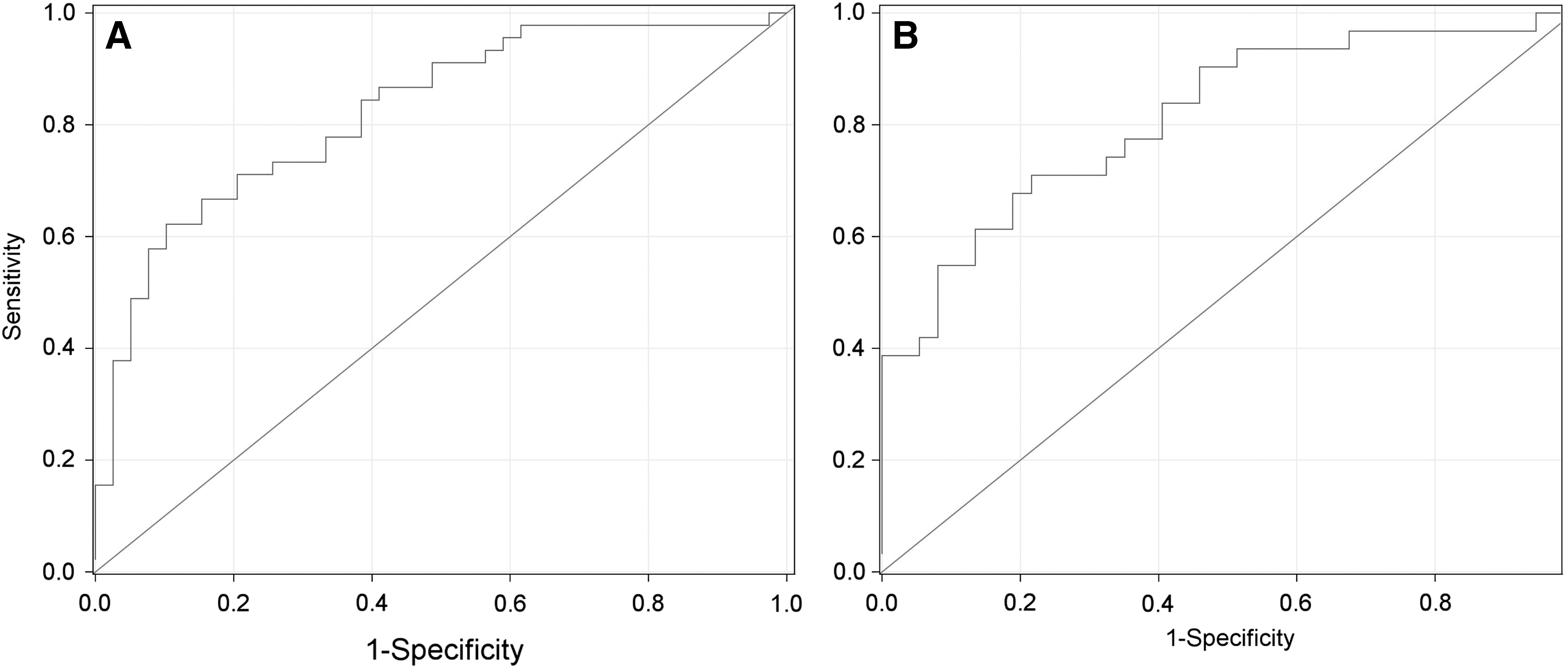
Receiver operating characteristics (ROC) curves for levothyroxine (LT4) dose at 6 (
Discussion
This observational cohort study in well characterized patients with CH and a normally located thyroid gland treated at a single center from the neonatal period provides extensive longitudinal data for various clinical presentations and outcomes. Overall, 54% of the patients in this cohort had transient CH and stopped treatment at a median age of 1.5 years. One of the key findings of this study is the first ever demonstration of an association between the LT4 dose required and thyroid function outcomes, detectable as early as six months of age. Patients with transient CH had lower LT4 dose requirements than those with permanent CH, with an optimal cutoff dose of 3.2 μg/kg/day at six months of age, with values below this threshold considered predictive of transient CH. A positive first-degree family history of CH significantly increased the risk of permanent CH.
The prevalence of transient CH has steadily increased in recent years (11,14 –17,19,22 –34). However, discrepancies have been found between studies due to differences in inclusion/exclusion criteria. Some studies have analyzed all patients with CH, regardless of etiology, including those without thyroid imaging data. This has resulted in patients being included not only with normally located glands, but also with athyreosis or ectopic thyroid glands, which are known to be associated with permanent CH (14,22,23,26,28). It has also resulted in those born premature (14,28,34), with associated congenital abnormalities (11,14,17,31), and a normally located hypoplastic gland (32) being excluded. Other studies have included a significant proportion of patients for whom the transient or permanent subtype could not be determined because the patients were lost to follow-up or too young (11,16,19,25,26,28 –30,34). These discrepancies introduce bias into estimates of the prevalence of transient CH, accounting for the considerable variation observed in reported values.
Previous studies have identified several risk factors associated with transient CH, such as sex (with boys more susceptible to the transient form) (14,25), low birth weight (16,18), neonatal distress requiring neonatal intensive care (16), ethnicity (non-white patients being more likely to have transient CH) (16), lower CH severity at diagnosis, as assessed by TSH blood tests at screening (15,25,26,28), serum TSH (14,19,29,30,32), or serum fT4 concentrations at diagnosis (28). Likewise factors more commonly associated with permanent CH have been identified, such as prematurity (11,17,20), concomitant congenital abnormalities (19), a family history of thyroid disease (17), thyroid morphology (thyroid hypoplasia at diagnosis is mostly associated with permanent CH (13,17)), and higher LT4 dose requirement at one to three years of age, with conflicting results between studies (14,17,22,24 –26,28 –32). However, to the authors' knowledge, no study has yet presented comprehensive data to determine the independent effects of all these variables on predictions of the transient or permanent nature of CH as early as possible. The present logistic regression findings provide no evidence that sex, neonatal problems (e.g., prematurity, SGA, or neonatal distress), concomitant congenital malformation, thyroid morphology, or initial CH severity could be used as predictors of the permanent or transient nature of the disease. The independent association found between LT4 dose requirement at six months of age and the form of CH (transient or permanent) in this study supports the clinical use of LT4 dose requirement as early as six months of age to identify those patients for whom LT4 treatment can safely be stopped. This association is consistent with the finding of previous studies that the risk of permanent CH is higher in patients with a high LT4 dose requirement at one to three years of age, with an optimal cutoff dose of 2.7 μg/kg/day at one year and 2.1–2.8 μg/kg/day at three years of age, depending on the study considered (24,30,32), and consistent with the mean dose required in patients treated for permanent CH with a normally located gland: 4.3 ± 1.3, 3.5 ± 1.0, and 3.2 ± 1.0 μg/kg/day at six months and one and three years, respectively (39). However, further prospective studies are required to confirm the use of the LT4 dose requirement with a cutoff at 3.2 μg/kg/day at six months of age (or even 2.5 μg/kg/day at 12 months of age) in patients with no history of familial CH during the routine monitoring or re-evaluation of thyroid function in patients with CH and an eutopic gland for the detection of transient CH.
This is the first study to demonstrate predictors of transient CH in infants as young as six months of age diagnosed and treated for CH with a eutopic gland during the neonatal period. One of the major strengths of this study is the inclusion of all patients in a defined population for whom comprehensive data were prospectively collected at birth at a single pediatric clinical center, making it possible to evaluate all demographic, clinical, biological, and thyroid imaging characteristics. The main limitation of this study is the observational nature of the retrospective data collection during follow-up, with treatment stopped at various time points. It was also not possible to control for the effect of consanguinity and for the results of the perchlorate discharge test, with transient forms appearing less likely in patients born to consanguineous parents and with a positive perchlorate test compared to patients with permanent forms of CH. Despite the inclusion of all patients treated for CH with a eutopic gland, the sample size is small, and the study provides no further insights into the mechanism underlying the transient and permanent forms of CH. However, the comprehensive collection of data in this study made it possible to estimate several important explanatory variables simultaneously and to use all observations in the estimation process.
In conclusion, based on the current findings, two groups of children with CH and an eutopic gland were identified. One group has the classical form of CH requiring long-term appropriate LT4 therapy. The second group consists of patients with transient CH, generally requiring lower doses of LT4 and displaying a spontaneous resolution of CH within a few months.
Further prospective studies are required to improve our understanding of the outcomes of patients with CH and a eutopic gland, but these original findings for patients with CH and a eutopic gland have important clinical implications for long-term patient management and highlight the need for appropriate and vigilant clinical and biological monitoring to prevent unnecessary long-term treatment during childhood. They highlight the need to evaluate LT4 dose requirements in patients as young as six months old, particularly for those with no familial history of CH. Parents should be made aware when they are informed of their child's diagnosis during the neonatal period that subsequent re-investigation will be necessary to determine whether the CH is persistent during childhood. However, the natural course of thyroid function of patients with transient CH during early childhood remains to be determined, and it is unknown whether these patients need to resume LT4 treatment later in life during times of increased thyroxine need due to increases in metabolism, such as puberty and pregnancy. The possibility of thyroid function deterioration in a subset of these patients warrants careful long-term follow-up of this population.
Footnotes
Acknowledgments
We thank the Association Française and the Fédération Parisienne pour le Dépistage et la Prévention des Handicaps de l'Enfant for helping to organize the study, all patients for participating in the study, and all the physicians involved in the follow-up of patients. This study was supported in part by the French Ministry of Health (Rare Disease Plan). Data collection, analysis, and interpretation and the decision to submit the paper for publication were the responsibility of the authors alone.
Author Disclosure Statement
No competing financial interests exist.