
Abstract
Background:
Recent reports suggest that prescriptions for thyroid hormones have increased. Recent trends in and determinants of the prevalence of treated hypothyroidism across the United Kingdom were therefore analyzed.
Methods:
Data covering the whole of the United Kingdom held by the National Health Service and the Office of National Statistics were examined. The main outcome measured was trends in the prevalence of treated hypothyroidism between 2005 and 2014. In addition, linear trend forecasting was performed to estimate projected trends in the prevalence of treated hypothyroidism up to the year 2025. Furthermore, determinants of variation of treated hypothyroidism prevalence across each of the 237 health areas in the United Kingdom in 2014 and its association with other health conditions were explored by multivariate linear regression analyses.
Results:
The prevalence of treated hypothyroidism increased from 2.3% (1.4 million) to 3.5% (2.2 million) of the total British population between the years 2005 and 2014 and is projected to rise further to 4.2% (2.9 million) by 2025. There was large geographical variation of treated hypothyroidism across the United Kingdom, with London having the lowest (1.4%) and the Western Isles of Scotland having the highest (6.3%) prevalence. This variation was attenuated, but did not completely disappear, after some potential determinants were accounted for. The prevalence of treated hypothyroidism was independently related to health areas, with a higher proportion of individuals who were female, white, and obese, and negatively associated with prevalent cigarette smoking. The prevalence of treated hypothyroidism was significantly associated with the frequency of prevalent atrial fibrillation but not with other major health conditions, including ischemic heart disease and osteoporosis.
Conclusions:
Between 2005 and 2014, the prevalence of treated hypothyroidism increased across the United Kingdom, has wide geographical variation, and is likely to increase further for the foreseeable future. Clinical effects and cost-effectiveness of the trend in increasing treatment of hypothyroidism remains to be evaluated.
Introduction
Primary hypothyroidism is a common endocrine condition characterized by raised serum thyrotropin (TSH) and reduced circulating thyroid hormone concentrations. Primary hypothyroidism is more common in females, and peak incidence rates occur between 40 and 50 years of age, with autoimmune thyroid disease as the most frequent etiology (1). Furthermore, over the last few decades, there has been an increasing interest in subclinical hypothyroidism (SCH)—a milder condition characterized by a raised serum TSH but with thyroid hormones within the reference range. Current guidelines recommend treatment of SCH only in specific situations such as younger individuals with hypothyroid-symptoms (2) or pregnant women who are thyroid peroxidase antibody (TPOAb) positive (3). Data from small samples suggest that the prevalence of treated hypothyroidism (both overt and SCH) in the United Kingdom and the United States is approximately 3% (4 –6). Levothyroxine (LT4), a synthetic isomer of the thyroid hormone thyroxine, is the recommended and ubiquitously used treatment in patients with hypothyroidism (7,8). Poor control of treated hypothyroidism, as evidenced by abnormal serum TSH levels, is seen in 35–60% of patients (9,10) and is associated with adverse bone and cardiac outcomes (11).
Several recent reports have highlighted that the prescribing of LT4 has increased both in the United States and the United Kingdom (12,13). The reasons underlying these increases in LT4 prescribing are unclear. Previous reports suggest that increased propensity to treat older individuals, those with milder elevation in serum TSH, and reduced length of LT4 prescriptions might be factors associated with increased LT4 prescribing (9,14,15). However, contemporary data on the trends in the prevalence of treated hypothyroidism reflective of the overall population and current clinical practice are lacking. Therefore, British national databases were interrogated to study recent trends in the prevalence of treated hypothyroidism and to evaluate population-based determinants between the various health areas of the United Kingdom.
Methods
The aims of this analysis were to study trends in the overall prevalence of treated hypothyroidism in the United Kingdom between 2005 and 2014 and to quantify variations in the prevalence of treated hypothyroidism at local health area population level. In addition, the study sought to forecast the prevalence of treated hypothyroidism for the future based on recent trends. To achieve this, data covering the whole of the United Kingdom held by the National Health Service (NHS) and the Office of National Statistics (ONS) were examined.
Health areas in the United Kingdom
Information regarding the prevalence of medical conditions and health-related parameters in the year 2014 was obtained from the health body for each geographical area in the United Kingdom (n = 237). These local health bodies have different structures and responsibilities but collect the same information. These are the Clinical Commissioning Groups in England (n = 211), Health Boards in Wales (n = 7), NHS boards in Scotland (n = 14), and Health and Social Care Trusts in Northern Ireland (n = 5).
Quality Outcomes Framework database
The Quality and Outcomes Framework (QOF) is a major pay-for-performance program that was introduced into British primary care in 2004 and accounts for approximately a quarter of general practice income (16). The QOF is intended to reward practices for the provision of “quality care” and to reduce variation across the country. QOF points are achieved based on the proportions of patients on defined disease registers who receive defined interventions. Points are scored by maintaining a register and not by the number of patients in each register. Therefore, there is no incentive for initiating treatment or changing clinical practice. Participation by practices in the QOF is voluntary, though participation rates are very high; for example, in 2015, the QOF data set includes data from nearly 99% of GP practices in England that were open and active at some point in the reporting period (17). Hypothyroidism was one of several clinical conditions that were covered by the QOF until 2015 when it was no longer included due to reorganization. Data for each individual component country of the United Kingdom were obtained separately from independent databases for that country for the period 2005–2014 (the last year when data were available; see Supplementary Appendix). A treated hypothyroidism case was defined by a LT4 prescription for any person of any age. The prevalence of treated hypothyroidism was calculated by dividing the number of patients with hypothyroidism on the QOF register with the total number of patients registered with all of the participating practices in each health area across the United Kingdom.
To assess variation in the prevalence of hypothyroidism across the United Kingdom, additional data on demographics (total population size, proportion aged >65 years, race/ethnicity, and sex), mean index of multiple deprivation scores, percentage of tobacco smokers, percentage of population with obesity, and proportion of the population with concomitant potentially related medical conditions (ischemic heart disease, heart failure, atrial fibrillation, hypertension, stroke/transient ischemic attack, diabetes mellitus, depression, dementia, osteoporosis, and chronic kidney disease) were obtained for each health area from the QOF and/or the ONS database registrations in 2014 (details in Supplementary Table S1).
Statistics
The overall prevalence of treated hypothyroidism across the United Kingdom between 2005 and 2014 was adjusted for median age of the population, percentage of women, percentage of smokers, percentage of white individuals, percentage of people who were obese, and year of evaluation.
The association of demographic, social, and life-style-related potential determinants (as independent covariates) with treated hypothyroidism prevalence in 2014 (as the dependent variable) was analyzed using multiple linear regression models. First, univariate regression models were fitted to identify relevant determinants (percentages of individuals aged >65 years, females, white people, obese individuals, smokers, and index of multiple deprivation score), and final models were built using a stepwise approach. For the stepwise approach, variables were entered into the model based on their biological relevance (i.e., outcome analyses adjusted for potential demographic confounders), and these were also adjusted further to identify whether the association of hypothyroidism prevalence with diseases linked to each other (i.e., atrial fibrillation and stroke) could be mediated due to that link. These models were built in a stepwise manner that was not automated, that is, p-values or other criteria were not used to enter/remove variables. A stepwise model building approach was used to assess any large changes after the inclusion of variables to identify potential model problems. Nonlinearity was assessed by adding quadratic terms with subsequent visual inspection of regression plots and assessment of changes in the effect estimates and/or explained variance of the model (relevant nonlinear effects were identified for percentage of individuals aged >65 years, females, and white individuals). Variables that were associated with treated hypothyroidism prevalence in univariate analyses were then combined into a multivariate analysis. Adjusted R 2 values were used to examine the degree of variation in hypothyroidism prevalence that is explained by the model.
In addition, to assess the association of the prevalence of treated hypothyroidism with other major health conditions, similar multivariate models were created with the prevalence of these diseases as dependent variables, and associated demographic, social, and life-style-related factors and the prevalence of treated hypothyroidism as independent variables, and were analyzed using multivariate regression. Furthermore, for each individual dependent variable, other health conditions that could be causally linked were added to the final model. For example, prevalence of atrial fibrillation was added to the model assessing the association between stroke disease and hypothyroidism, and so on. Moreover, due to the number of diseases being evaluated (n = 10), a p-value of <0.005 was used to denote significance for this particular analysis. The variance inflation factor (VIF) was calculated to assess collinearity. To fulfil model assumptions, variables that had a high VIF (>2.5) were centered and standardized (18). The assumption of normal distribution of residuals of the model was assessed and confirmed by visual inspection of standardized residuals and Q–Q plots.
Linear trend forecasting was performed to estimate the projected estimate of the prevalence of treated hypothyroidism in the United Kingdom, taking into account previous trends and the predicted changes in total population. Observed and fitted values were calculated using autoregressive integrated moving average modeling adjusted for the projected total British population until 2025. These population projections take into account population demographic change estimates (migration, deaths, births, and longevity) (19). From these forecasting models, a stationary R 2 value (a measure that compares the stationary part of the model to a simple mean model is preferable to ordinary r 2 when there is a trend or seasonal pattern, and can range from negative infinity to 1) was calculated. The statistical software Minitab v17.0 (Minitab, Inc., State College, PA) and IBM SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY) were utilized for all analyses. Geo-mapping was undertaken using Tableau® v10.3 (Tableau Software, Seattle, WA).
Results
Trends in prevalence of treated hypothyroidism, 2005–2014
Overall, in the United Kingdom, the crude prevalence of treated hypothyroidism has increased by 57% from 1.43 million (2.3%) to 2.24 million (3.5%) between 2005 and 2014. All the constituent countries in the United Kingdom have seen an increase in the prevalence of treated hypothyroidism over this period. However, there are consistent differences in the prevalence between the constituent countries, with England having the lowest and Scotland and Wales having the highest prevalence (Fig. 1). Adjustment for potential confounders made a slight difference to these results. For example, adjusted prevalence rates for treated hypothyroidism for the United Kingdom were 2.4% for 2005 and 3.4% for 2014. The adjusted year-on-year increase in the prevalence of treated hypothyroidism between 2005 and 2014 was significant (p = 0.03).
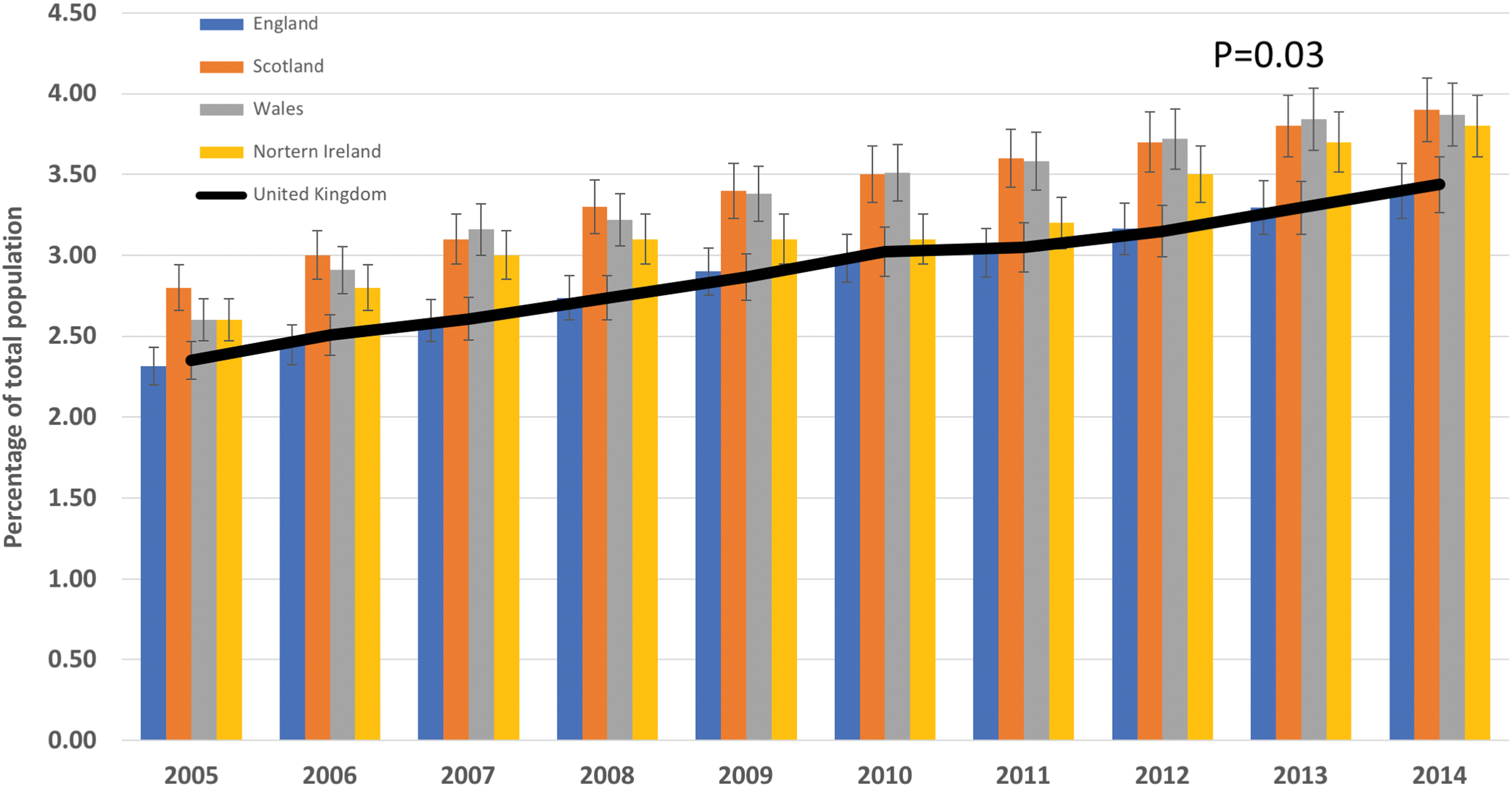
Adjusted prevalence of hypothyroidism in the United Kingdom and constituent countries between 2005 and 2014. Adjusted for median age of the population, percentage of women, percentage of smokers, percentage of white individuals, percentage of people who were obese, and year of evaluation. The p-value is derived from the regression analysis for the year of evaluation. Color images are available online.
Variation in prevalence of treated hypothyroidism across the United Kingdom in 2014
Data were available from all 237 health areas of the United Kingdom, comprising 9711 participating general practices. The smallest area by population was Orkney (population of 20,803), whereas the largest was Greater Glasgow and Clyde (population of 1,316,735). There were striking differences in the prevalence of treated hypothyroidism across the various geographical areas of the United Kingdom, with the lowest prevalence in Central London (1.4%) and the highest in the Western Isles of Scotland (6.3%; Fig. 2A).

Variation in prevalence of hypothyroidism (as percentage of total local population) in 2014 by Clinical Commissioning Group (CCG) area in England. (
Determinants of prevalence of treated hypothyroidism across health areas
In univariate analysis, a number of variables were associated with the prevalence of treated hypothyroidism in each health area in the United Kingdom (Supplementary Table S2). In the multivariate analysis, the prevalence of treated hypothyroidism was positively associated with the population health area percentage of females, percentage of white individuals, and percentage prevalence of obesity, and negatively associated with the percentage of smokers (Supplementary Table 3 and Fig. 3). The proportion of individuals aged >65 years and the index of multiple deprivation score of each health area were no longer significantly related to the prevalence of treated hypothyroidism after multivariate adjustment. The final model explained 52% of the variation in prevalence of treated hypothyroidism between the different health areas.
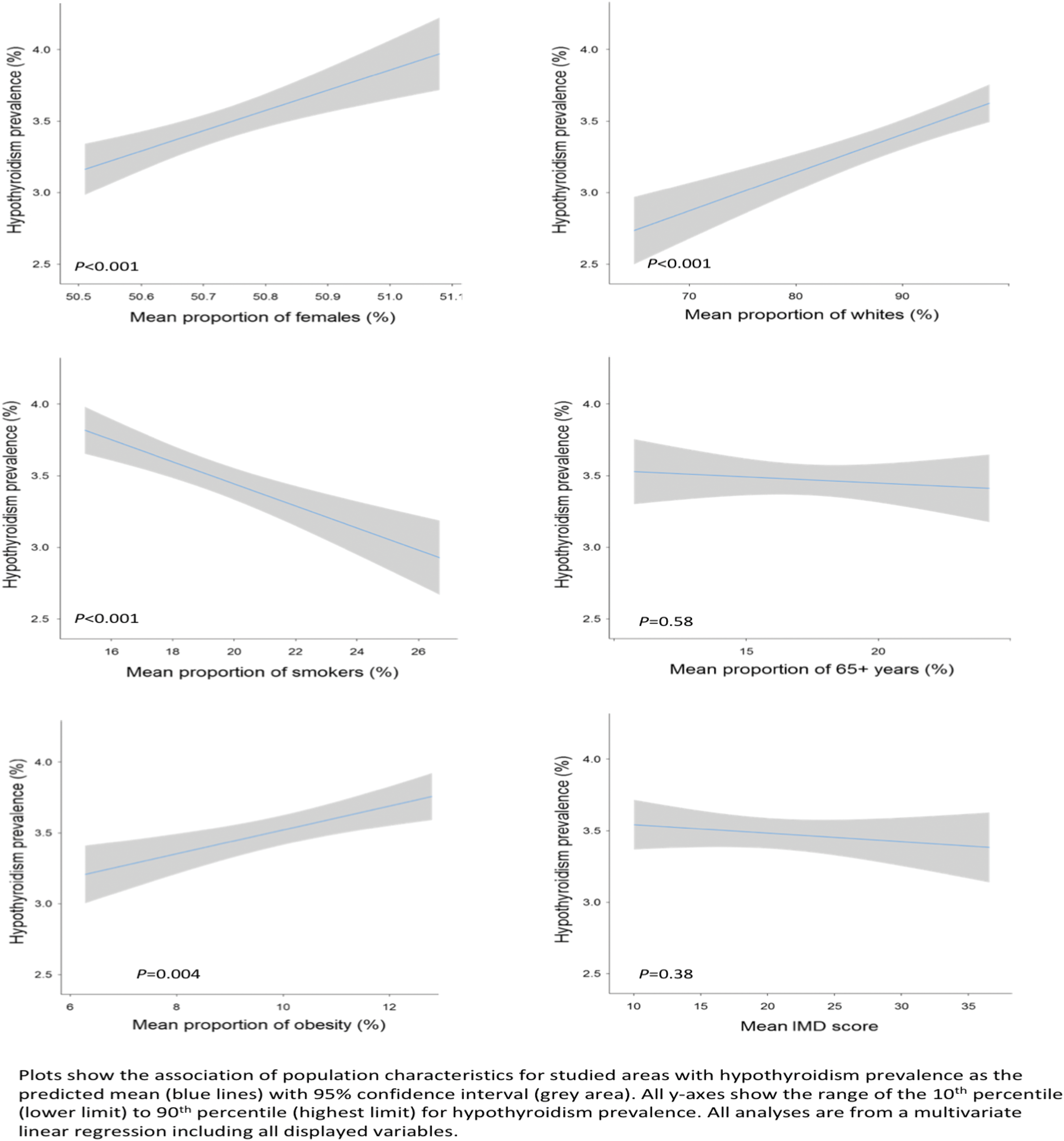
Determinants of treated hypothyroidism with population characteristics across different health areas of the United Kingdom. Color images are available online.
Once the significant determinants of treated hypothyroidism were adjusted for, the variation in treated hypothyroidism across the United Kingdom was attenuated (Fig. 2B). For example, the adjusted prevalence of treated hypothyroidism in Central London was higher (2.6%) and was lower in the Western Isles of Scotland (4.1%).
Associations of treated hypothyroidism with major health conditions across health areas
The prevalence of treated hypothyroidism in each health area was significantly associated with the prevalence of atrial fibrillation (β = 0.20 [confidence intervals (CI) 0.14–0.26], p < 0.001). This association attenuated after further addition of prevalent ischemic heart disease (β = 0.10 [CI 0.04–0.15], p < 0.001; Fig. 4). All other major health conditions evaluated, however, showed no significant association with the prevalence of hypothyroidism. Specifically, there was no statistically significant association between the prevalence of ischemic heart disease, heart failure, or osteoporosis with the prevalence of treated hypothyroidism across each of the health areas studied. The only exception was for the prevalence of hypertension, which remained significantly associated with the prevalence of treated hypothyroidism, even after additional adjustment for multiple analyses. However, the VIF was high, suggesting a high level of multicollinearity. This association therefore needs to be interpreted with caution (Supplementary Table S4).

Association of prevalent treated hypothyroidism with prevalent atrial fibrillation. Color images are available online.
Projected trends in the prevalence of treated hypothyroidism between 2015 and 2025
Forecasting trend modeling (stationary R 2 = 0.965) suggests that the prevalence of treated hypothyroidism will increase further to 4.65% [CI 4.47–4.83] of the total population in the year 2025, considering British population projected changes and assuming there is no alteration to current prescribing habits (Fig. 5). In 2025, the population of the United Kingdom is estimated to be just over 69 million, and based on these models, the number of people with treated hypothyroidism is therefore projected at 3.23 [CI 3.10–3.35] million.
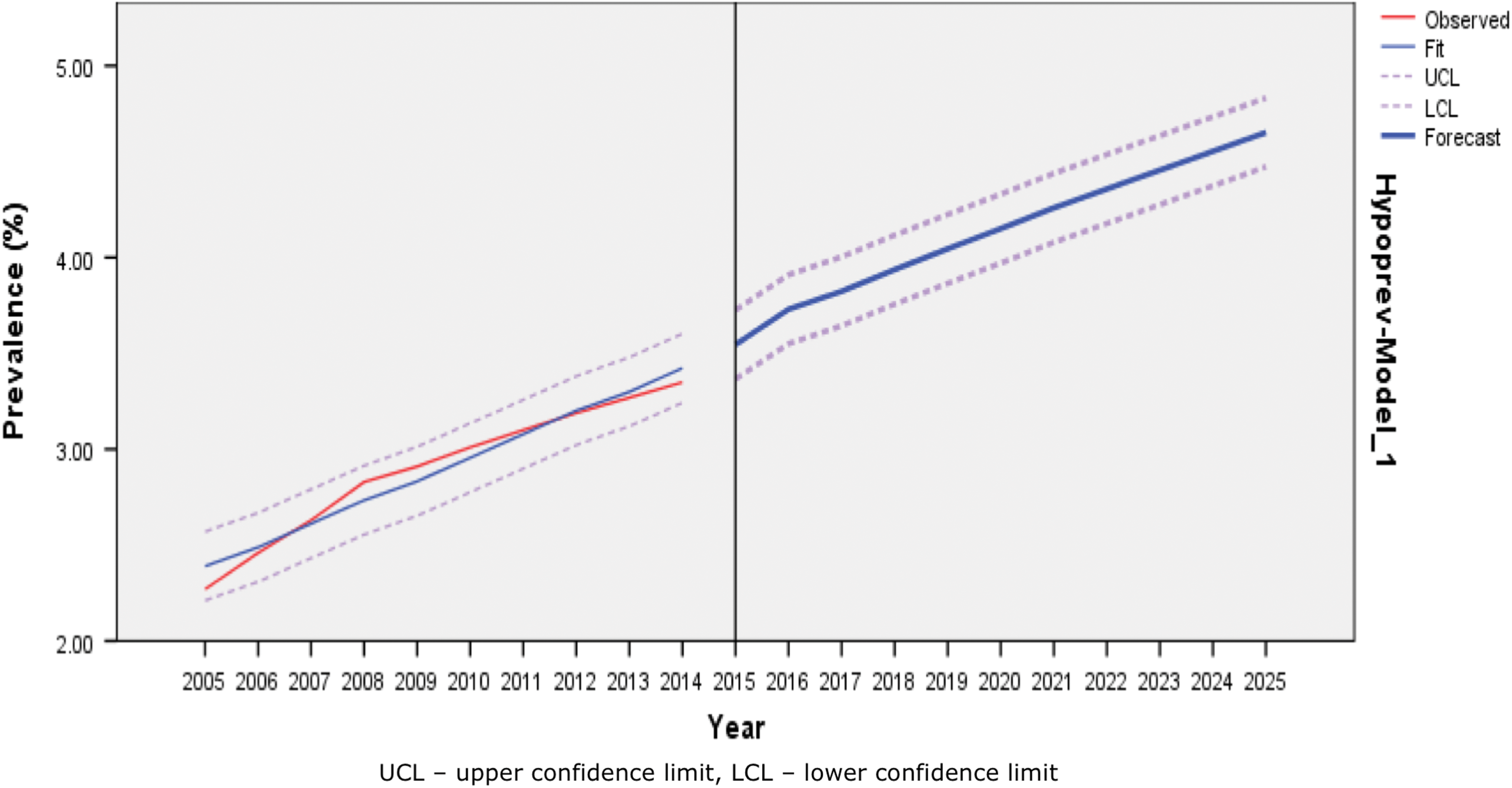
Observed and forecasted prevalence of treated hypothyroidism in the United Kingdom up to 2025. Color images are available online.
Discussion
The prevalence of treated hypothyroidism has increased in the United Kingdom in the last 10 years (between 2005 and 2014) from 2.3% to 3.5%, thereby affecting 0.8 million more individuals. The reasons behind this increase are unclear but are likely to be multifactorial and include a growing population with changes in demographic features and life-style. The results of the present analysis do not provide any data on whether there is an increase in the incidence of hypothyroidism or if there is an increased propensity to detect and treat milder (subclinical) forms of the condition. There is wide geographic variation within the United Kingdom in the prevalence of treated hypothyroidism, which is partly explained by population demographics and life-style habits in that area such as the proportion of women, white population, obesity levels, and smoking habits. In 2014, 2.25 million individuals were being treated for hypothyroidism in the United Kingdom. If the current trend continues, then it is likely that the prevalence of treated hypothyroidism will rise further to 4.65% of the total population (affecting just over 3.2 million individuals).
There are limited data available on trends in the prevalence of treated hypothyroidism at a national level. Analysis from several cycles of the National Health and Nutrition Examination Survey (NHANES) in U.S. adults (aged ≥20 years) showed that the prevalence of thyroid hormone use increased from 5.1% in 1999–2000 to 6.4% in 2011–2012 (p = 0.007 for trend) (5). There were increases observed in both men and women (from 2% to 3.2% and from 8% to 9.3%, respectively), and also in younger (40–64 years) and older (>65 years) individuals (from 5.9% to 6.9% and from 13% to 15%, respectively) over this time period. However, these data were obtained from a relatively small group (approximately 5000 participants per each NHANES cycle), although data were weighted to be nationally representative. Interestingly, the biggest increase in thyroid hormone use was seen in non-Hispanic whites. An interrogation of a large population-based health database in Tayside, Scotland, found that the prevalence of treated hypothyroidism increased in both men and women from 0.5% to 0.9% and from 3.1% to 5.1%, respectively, between 1994 and 2001, which was attributed to an increasing incidence and earlier diagnosis and treatment (20). Analysis of community prescription data from England showed that the number of prescriptions for thyroid hormones and the ingredient costs increased between 1998 and 2007, while the average length of prescriptions reduced (15). The data provided in the current analysis not only confirm these earlier results but also provides a more accurate and contemporary representation of treated hypothyroidism prevalence and variation across the entire population of the United Kingdom. Furthermore, as treated hypothyroidism is no longer on the QOF list of conditions for which data are gathered, it is unlikely that updates to the results of this analysis will be possible in the future using a similar methodology.
There are several possible explanations for the increased trend observed in the prevalence of treated hypothyroidism. The total population of the United Kingdom has increased from 60.4 to 64.6 million (an increase of 6.9%) between 2005 and 2014 (21), partly due to the increase in longevity (the average life-span increased from 79.1 to 81.1 years between 2005 and 2015, an increase of 2.5%) (22). These small increases, however, do not fully explain the large relative increase in the prevalence of treated hypothyroidism. Other possible reasons could be an increase in thyroid function test checking, leading to higher case finding and treatment (23), increased propensity to treat milder forms of hypothyroidism particularly in older individuals (9), and a decline in cigarette smoking (24), leading to a rise in TSH and TPOAb levels (25). A raised serum TSH—a diagnostic hallmark of hypothyroidism—is influenced by increases in age, but age-specific reference ranges are not utilized (26,27). The current analysis, however, does not confirm that areas with a higher proportion of older individuals (>65 years) have a greater prevalence of treated hypothyroidism once other factors are taken into account. At the start of the time period corresponding to the analysis reported here, some experts believed that the upper limit of the TSH reference range should be reduced, which could have influenced some clinicians to prescribe treatments at lower TSH levels (28). Other possible explanations for the increase in the prevalence of treated hypothyroidism could be due to the increasing use of ablative radioiodine and surgical therapies for both benign and cancerous thyroid diseases (29,30), as well as increasing use of thyroid hormones during pregnancy (31). Finally, an increase in body mass index leads to an increase in serum TSH levels (32), and the present analysis suggests that areas with a higher prevalence of obesity are associated with a higher prevalence of treated hypothyroidism.
The results of the current analysis have several implications. It is increasingly becoming apparent that a mildly raised serum TSH (subclinical hypothyroidism) is not associated with adverse outcomes, particularly in older individuals (33 –35). Importantly, short-term trials for the treatment of subclinical hypothyroidism in older individuals have not shown any improvement in symptoms or quality of life (36,37). In addition, several observational studies in older individuals have shown that higher serum thyroxine levels and/or lower circulating TSH concentrations are associated with worse outcomes (38 –40). There are economic implications of increased LT4 prescribing, as well as sparse evidence of cost-effectiveness, particularly in the elderly. In the United Kingdom, a diagnosis of hypothyroidism leads to exemption from payment of prescription charges (i.e., free medication) in people who would otherwise have to pay (41). Poor control of hypothyroidism while on treatment, as evidenced by abnormal serum TSH levels, is common (9,10) and has been associated with increased risk of cardiovascular disease, atrial fibrillation, and osteoporotic fractures (11). It is concerning that the data suggest that areas with a higher prevalence of treated hypothyroidism have a higher frequency of atrial fibrillation, independent of other risk factors. However, it is unclear from the data whether there is a causal link between the two conditions and whether this is related to poor control (abnormal TSH levels). It is likely that a significant number of older community-dwelling treated hypothyroid patients have iatrogenic thyrotoxicosis and therefore are at risk of developing atrial fibrillation (42). Reassuringly, the current analysis does not suggest that areas with higher prevalence of treated hypothyroidism are associated with a higher occurrence of other major diseases such as ischemic heart disease, heart failure, osteoporosis, depression, or dementia.
The study has several strengths. This is the first report, as far as the authors are aware, outlining the prevalence of treated hypothyroidism using a national-level database. The data obtained from the QOF have been shown to be reliable and accurate in other conditions (43). In addition, it was possible to analyze geographical variation across the entire country and study population-level factors that may be associated with the variation in prevalence. Another strength of the data is that they reflect contemporary clinical practice. It was not possible to assess if the management of hypothyroidism was “appropriate” or following guidelines. However, it does confirm, not surprisingly, that clinicians vary in how they manage primary hypothyroidism (9).
This study also has some weaknesses. The results obtained may not be generalized to other countries, as the healthcare model and data-collection methodology may be different. In addition, data were collected at the population level, and therefore several important individual- or subgroup-level factors such as demographic details (age, sex, and smoking status), underlying etiology of hypothyroidism, serum TSH, and thyroid hormone level at diagnosis, control of hypothyroidism based on serum TSH levels on treatment, and symptoms and quality of life could not be assessed, thus leading to potential ecological inference fallacy. In addition, these data are unable to indicate whether the treatment of hypothyroidism was “appropriate.” There is evidence to suggest that approximately 6% of individuals are started on treatment with thyroid hormones when they are euthyroid (9), although there is also evidence that this is not associated with any benefit and could potentially cause harm (44). Furthermore, the iodine status of each health area and the effect of endocrine disruptors on the prevalence of treated hypothyroidism could not be assessed (45,46). The prevalence of some determinant factors (such as smoking and obesity) and associated chronic major health conditions (such as diabetes mellitus, depression, and chronic kidney disease) were not available for children (<15–18 years of age, depending on condition) or in younger individuals (<50 years for osteoporosis). This may have led to some error in the results, although the number of individuals that may have been excluded is likely to be very small. Finally, the projections for the future are based on previous years' data on prevalence, and changes in population numbers and/or demographics as well as clinical practice (including TSH thresholds for considering treatment) may affect actual observations.
In conclusion, this analysis demonstrates that the diagnosis of treated hypothyroidism increased in the United Kingdom between 2005 and 2014. There is wide geographical variation in the prevalence of the condition, partly related to population demographics in each area, and therefore this could change as a result of demographic or life-style changes. There appears to be an association between the prevalence of treated hypothyroidism and atrial fibrillation, which requires further evaluation. The use of age- and race/ethnicity-appropriate reference ranges for TSH need to be considered. In addition, the clinical outcomes and cost-effectiveness of increased treatment of hypothyroidism across various age and racial/ethnic groups—mostly for marginally elevated serum TSH levels—need to be studied in a prospective manner.
Footnotes
Acknowledgments
S.R. is funded by a NIHR Career Development Fellowship (CDF-2012-05-231). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, or the Department of Health and Social Care. The funder was not engaged in the study design; in the collection, analysis, and interpretation of the data; in the writing of the report; or in the decision to submit the article for publication.
Author Disclosure Statement
None of the authors report any conflicts of interest in this work.
Supplementary Material
Supplementary Appendix
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4