
Abstract
Background:
Extrathyroidal extension (ETE) by papillary and follicular thyroid carcinoma can be associated with increased risk of tumor recurrence and mortality. In the seventh edition of its Cancer Staging Manual, the American Joint Committee on Cancer (AJCC) defined minimal ETE as the involvement of skeletal muscle (i.e., strap muscles) or perithyroidal soft tissue. The eighth edition of the AJCC Cancer Staging Manual has changed the criteria so that only grossly evident (macroscopic) ETE involving strap muscles (not microscopic ETE involving perithyroidal soft tissue) affects tumor staging.
Summary:
Concordance of identifying microscopic ETE (as well as extranodal extension by carcinoma metastatic to lymph nodes) was previously evaluated among 11 expert endocrine pathologists. The overall agreement rate was slight when rendering a diagnosis of ETE. Concordance was highest when pathologists assessed the spatial relationship of carcinoma to skeletal muscle. This article discusses the significance of these findings. It also reviews relevant anatomic and developmental considerations related to the boundaries of the thyroid.
Conclusions:
The results of the concordance study provide additional rationale supporting stringent criteria for diagnosing ETE, as proposed by the eighth edition of the AJCC Cancer Staging Manual. It is expected that these rigid morphologic criteria will potentially reduce interobserver variability and enhance consistency in the diagnosis and staging of thyroid carcinoma.
Introduction
Extrathyroidal extension (ETE) by well differentiated thyroid carcinoma, particularly papillary thyroid carcinoma (PTC), has been the focus of significant investigation and debate. Within the context of PTC, the reported incidence of ETE varies from 5% to 45%, and its presence increases the risk of both recurrence and mortality (1 –12). As discussed forthwith, estimates of its frequency and assessment of its significance depend upon authors' definitions of ETE. In the seventh edition of its Cancer Staging Manual, the American Joint Committee on Cancer (AJCC) stratified ETE into minimal (mETE) and significant ETE (sETE), both of which impacted staging of differentiated thyroid carcinoma (i.e., all histologic types except anaplastic carcinoma) (13). The manual clarified mETE with the parenthetical phrase “e.g., extension to sternothyroid muscle or perithyroid soft tissues” (Fig. 1), and defined sETE as invasion into the subcutaneous soft tissue, larynx, trachea, esophagus, or recurrent laryngeal nerve. Use of the sternothyroid muscle as an example presumably indicated incorporation of other strap muscles into the definition of mETE. The 2014 version (v3.1.0.0) of the College of American Pathologists (CAP) Thyroid Carcinoma Protocol supported this interpretation, stating “minimal extrathyroidal extension includes the presence of carcinoma extending into perithyroidal tissues, including infiltration of skeletal muscle, as well as around sizable vascular structures and nerves” (14). When present, mETE increased the stage of any tumor measuring <4 cm (i.e., pT1 or pT2) to pT3, and significant ETE to pT4. By contrast, the eighth edition of the AJCC Cancer Staging Manual defines pT3b as grossly evident ETE involving only the strap muscles (sternohyoid, sternothyroid, thyrohyoid, or omohyoid muscles), as identified during surgery or gross pathologic inspection (Fig. 2) (15). As described in the current version of the CAP Thyroid Carcinoma Protocol, this requirement warrants review of gross, intraoperative, and radiologic findings. This criterion underscores the importance of adequate dissection technique and thorough macroscopic evaluation, enhancing the importance of the prosector's role. Notably, neither the AJCC manual nor the explicative notes provided by the CAP offer guidance regarding the scenario in which microscopically extensive ETE is not appreciated grossly. Accordingly, macroscopic examination of thyroid cancer resection specimens by an experienced prosector (if not an attending pathologist) may be necessary and is recommended. This more stringent definition also elevates the importance of intraoperative and radiologic correlation, and incorporates review of these findings into the pathologist's workflow. Importantly, microscopic ETE involving perithyroidal soft tissue no longer applies to tumor staging, since many studies showed this finding to have no independent prognostic value (16 –19).
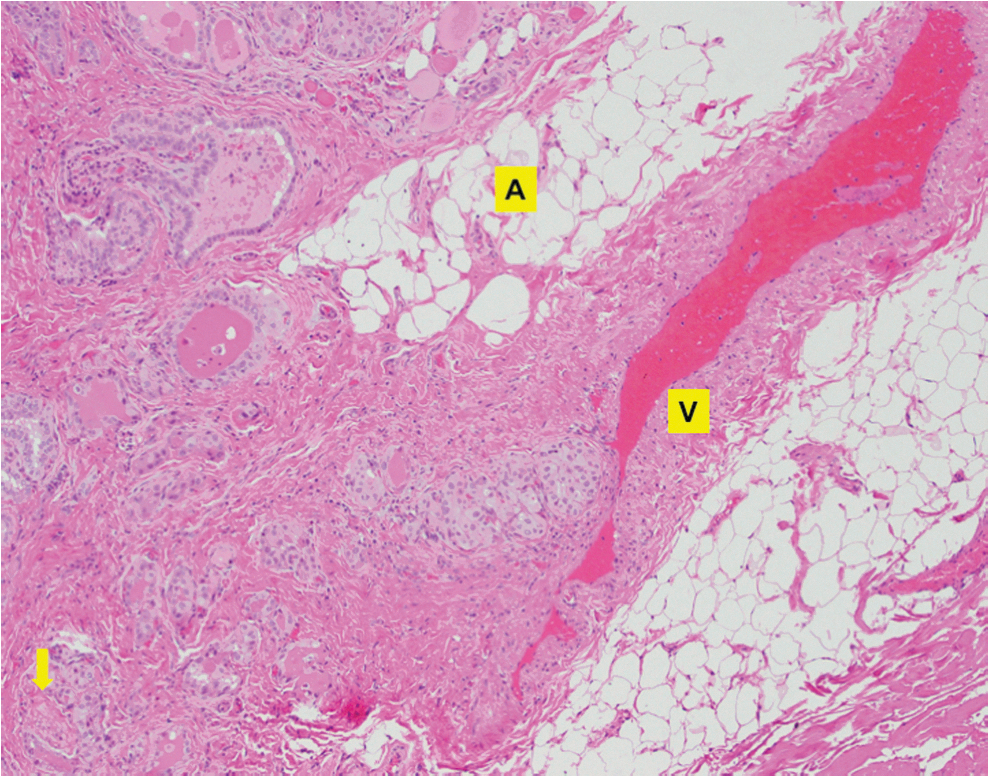
Papillary thyroid carcinoma approaching thick-walled vasculature (V), and involving adipose tissue (A) and nerve (arrow).

Grossly evident extrathyroidal extension (E) of papillary thyroid carcinoma. The macroscopic image shows a transverse cut of the thyroid gland, with right (R) and left (L) lobes indicated. Microscopic examination confirms grossly evident involvement of skeletal muscle (M) by papillary thyroid carcinoma (C), as shown by the inset images.
Analogous to ETE, extranodal extension (ENE) by carcinoma metastatic to lymph nodes represents another diagnostically challenging aspect of thyroid pathology. The thyroid gland contains abundant lymphatic vessels, which drain to pericapsular, paratracheal/pretracheal, prelaryngeal, retropharyngeal, and retroesophageal lymph nodes, as well as to lymph nodes in the internal jugular and recurrent laryngeal nerve chains and anterosuperior mediastinum (20). Lymph node metastases are commonly seen in patients with PTC, occurring in 40–50% of cases (or more) upon initial diagnosis (21 –24). When lymph nodes are positive, reported rates of ENE range from 22% to 45% (25 –27). ENE is a strong and independent predictor of disease recurrence, distant metastasis, and disease-specific survival in some studies (25,27 –30).
Given the clinical significance of ETE and ENE, concordance between expert head and neck/endocrine pathologists was assessed in terms of diagnosing these features (31,32). Herein, the implications of the findings are reviewed, with consideration of the newly updated cancer staging guidelines. The gland's anatomy and embryologic development are also reviewed, as diagnosis of ETE warrants understanding of and attention to these topics.
Review
Thorough knowledge of the embryology and surgical anatomy of the thyroid gland is crucial for histologic assessment of its boundaries, since the developmental trajectory of the gland determines its spatial relationship with surrounding tissues. Formation of the gland begins in the pharynx during the sixth week of embryonic development. The thyroid anlage, a midline thickening of endodermal epithelium, appears at the boundary between the anterior two thirds and the posterior third of the tongue (33). This location is immediately caudal to the tuberculum impar, a median swelling on the pharyngeal surface of the first pharyngeal arch. The thyroid primordium grows into the underlying mesenchyme, expanding laterally to gradually acquire a bi-lobed configuration. As the thyroid anlage descends anterior to the hyoid bone, its site of origin persists as the foramen cecum, a small depression in the terminal sulcus posterior to the tongue (34). Initially, the thyroglossal duct connects the descending gland to the foramen cecum. The lumen of this duct eventually becomes a solid cord (i.e., the thyroglossal duct becomes the thyroglossal tract), and subsequently ruptures at its midpoint. This breakage enables the gland to reach its final destination, at the level of the laryngeal primordium.
By this point, the thyroid comprises pear-shaped left and right lobes, connected by an isthmus. This configuration can be variable: up to 10% of individuals lack an isthmus, whereas approximately 40% have an additional pyramidal lobe extending superiorly from the central portion of the isthmus (35). This pyramidal lobe represents a remnant of the thyroglossal duct. Another structure, alternately described as a small strap muscle versus a fibrous band that occasionally contains some muscle fibers, connects the hyoid bone to the central aspect of the isthmus (or the apex of the pyramidal lobe, if present) as well as the thyroid cartilage. Various authors have conferred multiple names upon this muscular structure, including the “levator glandulae thyroideae of Soemmerring,” the “levator glandulae thyroideae superficialis medius et longus of Krause,” the “musculus thyroideus of Merkel,” and the “hyo-thyro-glandulaire of Pointe” reviewed in April (34) and Mete et al. (36). This multiply eponymous structure creates an intimate relationship between thyroid parenchyma and skeletal muscle. This anatomical proximity complicates evaluation of skeletal muscle involvement by thyroid carcinoma in the isthmus, a criterion often used for the diagnosis of ETE.
Identification of ETE by a tumor also requires evaluation of the relationship between the thyroid and its adjacent tissues. The thyroid resides anterior to the trachea (predominantly), with the isthmus just caudal to the cricoid cartilage, and the right and left lobes extending inferiorly to the level of the fifth tracheal ring (34,37). Thickened fascia known as the posterior suspensory ligament of Berry attaches the gland to the cricoid cartilage, trachea, and cricopharyngeus muscle (36). Branches of the inferior thyroid artery and the recurrent laryngeal nerve course between anterior and posterior layers of the pretracheal fascia, posterior to the thyroid, positioning them in close proximity to and occasionally within the gland. In addition, the thyroid gland sits posterior to and is partially covered by the sternohyoid and sternothyroid muscles. The insertion of the sternothyroid muscle onto the thyroid cartilage demarcates the superior edges of both lobes. Bilaterally, the gland extends around the trachea and esophagus to abut the carotid sheaths.
Beyond these anatomic and developmental features, several caveats obfuscate the demarcation and extent of the thyroid parenchyma, as well as the diagnosis of ETE. The thyroid gland lacks a complete fibrous capsule, and is instead surrounded by a partial fibroadipose pseudocapsule of variable thickness, usually continuous with intraglandular fibrous septa that delineate parenchymal lobules (36). Given the composition of this pseudocapsule, the presence of carcinoma in adipose or fibrous tissue beyond thyroid parenchyma does not necessarily indicate ETE. Additionally, adipose tissue metaplasia of the interfollicular stroma sometimes occurs (Fig. 3), further complicating the relevance of adipose tissue in the assessment of ETE (38). Due to the association between Soemmerring's muscle and the isthmus and pyramidal lobe (as discussed above), involvement of skeletal muscle around these locations may not be diagnostic of ETE. Skeletal muscle fibers or bundles other than Soemmerring's muscle can be seen within the thyroid gland parenchyma, as are nerves and thick-walled blood vessels (Figs. 4 and 5; reviewed in 31). Therefore, invasion of these structures juxtaposed against thyroid parenchyma is most likely an unreliable criterion for the identification of ETE.
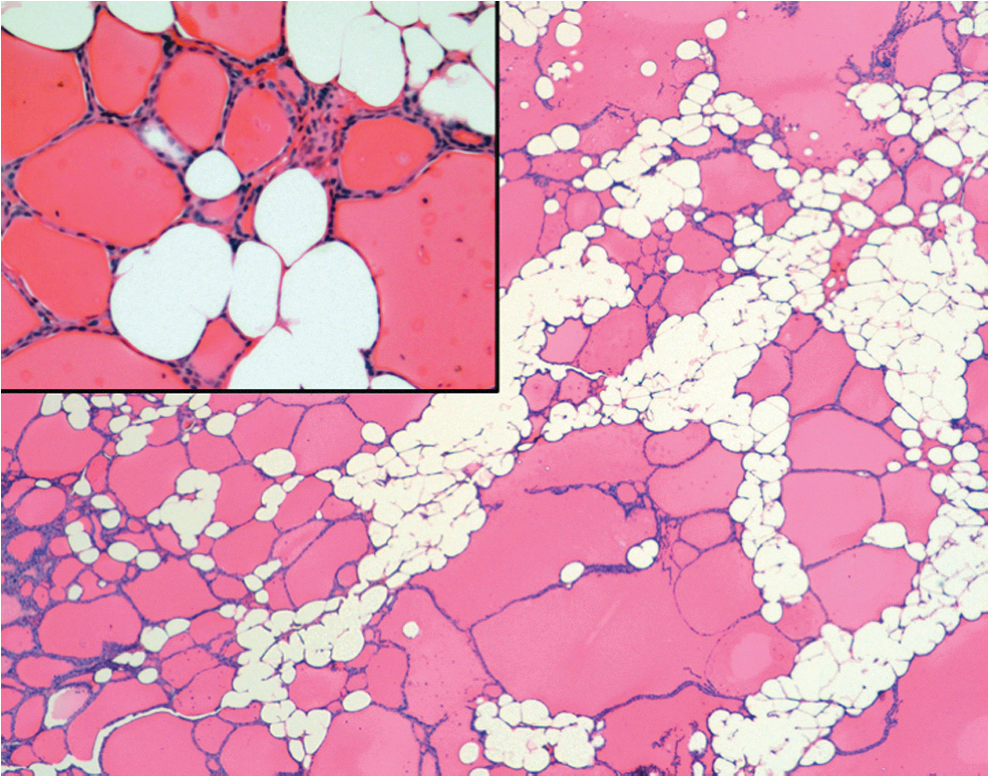
Adipose metaplasia of interfollicular stroma. Higher-power magnification shows bland cytomorphologic features (i.e., no evidence of carcinoma).
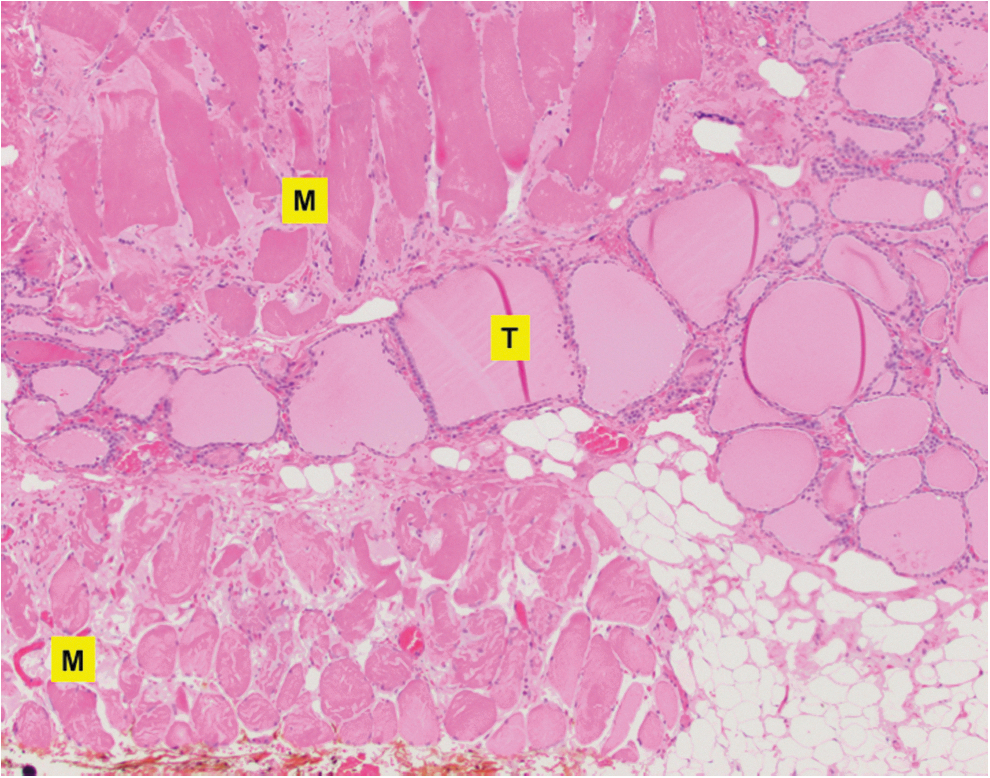
Commingling of skeletal muscle (M) and non-neoplastic thyroid parenchyma (T) in the thyroid isthmus.
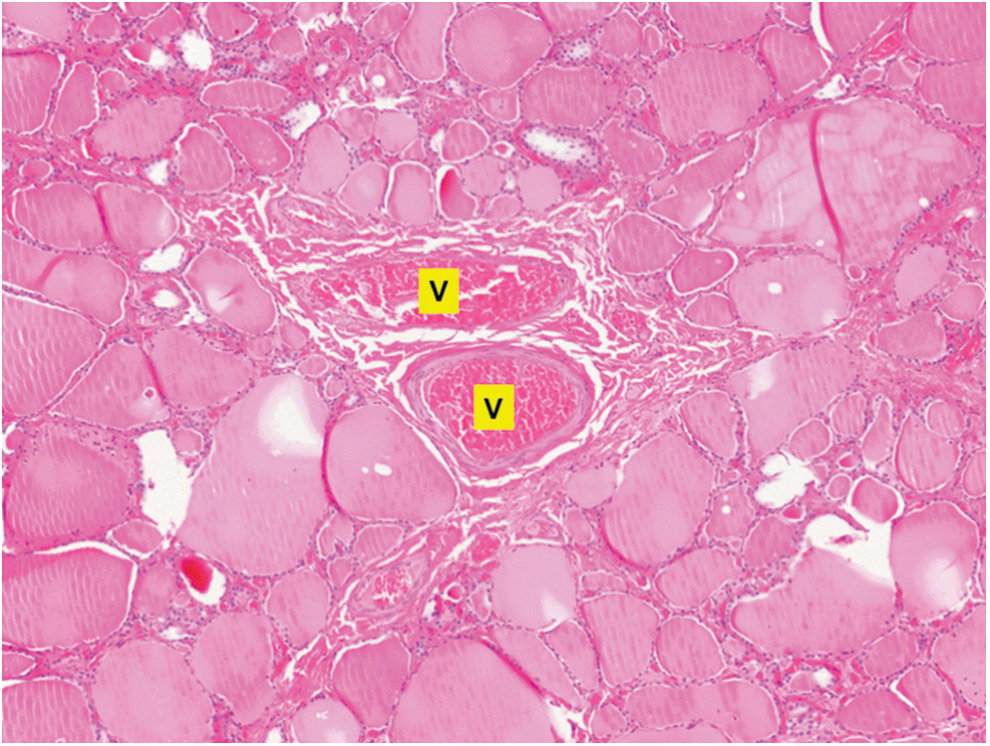
Thick-walled vasculature (V) surrounded by non-neoplastic thyroid parenchyma.
Given the prognostic significance of ETE and ENE, concordance between expert head and neck/endocrine pathologists was assessed in terms of identifying these clinically important histopathologic parameters (31,32). These studies were conducted prior to implementation of the AJCC eighth edition guidelines. According to Institutional Review Board (IRB) guidelines and with IRB approval, a panel of 11 expert pathologists from the United States, Canada, and Italy was asked to review scanned slides of PTC resection specimens for potential ETE (69 cases) and ENE (61 cases). These numbers were determined by availability during the interval of the study, and included carcinomas arising in all portions of the gland (isthmus, lateral lobes, etc.). Cases were initially reviewed by two pathologists (A.T.T. and B.M.W.), with some examples considered unequivocal and others considered ambiguous by these pathologists. In addition to assessing ETE and ENE, the panel also commented on the involvement of perithyroidal and perinodal adipose tissue, skeletal muscle, nerves, and thick-walled vasculature, and annotated whether these findings contributed to their diagnoses.
In terms of ETE, overall agreement was slight. Su et al. summarized their findings and statistics in Table 1 of their manuscript (31). Concordance was highest when pathologists assessed potential ETE using the spatial relationship between carcinoma and skeletal muscle. Agreement was lowest when pathologists evaluated carcinoma relative to thick-walled vasculature. This low interobserver agreement resulted in part from the lack of well-defined morphologic criteria for the identification of ETE. All pathologists evaluated perithyroidal skeletal muscle involvement for diagnosing ETE. Two pathologists also assessed involvement of perithyroidal fat and proximity to nerves (but not proximity to thick-walled vasculature), and seven pathologists considered each of the four specified features (involvement of skeletal muscle and perithyroidal fat, as well as proximity to nerves and thick-walled vasculature). Additionally, six pathologists used different assessment criteria for carcinoma arising in the thyroid isthmus; four of these six pathologists considered skeletal muscle involvement less significant, and two considered adipose tissue involvement less likely indicative of ETE in this location.
The diagnostic agreement was fair among pathologists for identification of ENE. Assessment of ENE showed the highest proportion of observed agreement when pathologists examined carcinoma relative to perinodal muscle. Proportion of observed agreement for consideration of perinodal nerve involvement was also high. The proportion of observed agreement was lowest when pathologists evaluated perinodal fat involvement as a diagnostic criterion for ENE. As with ETE, variability exists among pathologists in using different histopathologic parameters for the diagnosis of ENE. All pathologists in the expert panel regarded perinodal fat involvement as diagnostic of ENE (Fig. 6). Seven pathologists also considered involvement of skeletal muscle, nerve, and thick-walled vasculature diagnostic of ENE. The remaining four pathologists evaluated either one or two (but not all three) of these structures.
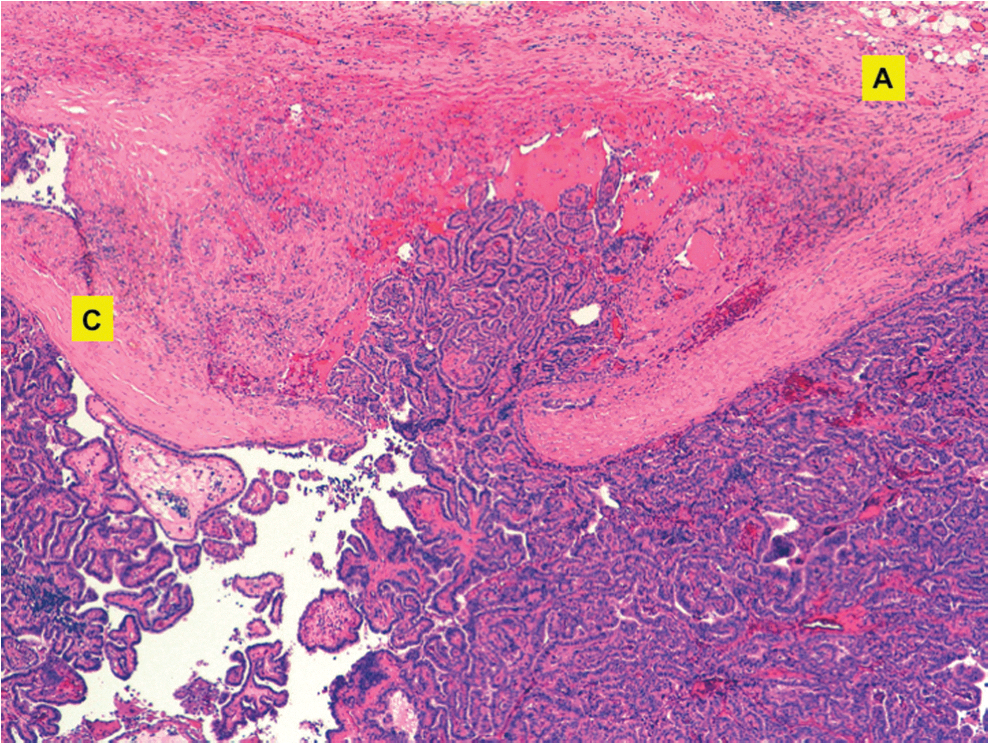
Extranodal extension by metastatic papillary thyroid carcinoma. Carcinoma has extensively replaced this node, and penetrates the capsule (C) to approach perinodal adipose tissue (A).
Additional information about these studies, including demographic data and pathological characteristics of the study cohort, is available in the cited publications. The authors are unaware of other prior studies regarding interobserver variability in diagnosis of ETE/ENE.
Summary
The microscopic identification of ETE represents a subjective aspect of endocrine pathology, particularly when the diagnosis results from consideration of only adipose tissue, vasculature, or nerves rather than skeletal muscle. The complexity of diagnosing ETE results in part from the gland's unique histologic, anatomic, and developmental properties. Additional data about patient outcomes when carcinoma involves or approaches adipose tissue, vasculature, and/or nerves may be contributory. Without such studies, however, designation of ETE based on these features remains controversial.
Conclusions
The findings reflect those of many other studies involving thyroid pathology in which agreement between pathologists is limited regarding several morphologic features (39 –42). The relatively strict criteria for ETE included in the eighth edition of the AJCC Cancer Staging Manual are appropriate, given the anatomy and histology of this gland, and may decrease interobserver variability, leading to greater consistency in diagnosis and staging of thyroid carcinoma.
Footnotes
Author Disclosure Statement
The authors have no relevant conflicts to disclose, pertinent to the submitted manuscript.