
Abstract
Background:
In areas with incomplete salt iodization coverage, infants and children aged 6–24 months weaning from breast milk and receiving complementary foods are at risk of iodine deficiency. However, few data exist on the risk of excessive iodine intake in this age group. Thyroglobulin (Tg) is a sensitive marker of iodine intake in school-age children and adults and may be used to estimate the optimal iodine intake range in infancy. The aim of this study was to assess the association of low and high iodine intakes with Tg and thyroid function in weaning infants.
Methods:
This multicenter cross-sectional study recruited infants aged 6–24 months (n = 1543; M age = 12.2 ± 4.6 months) receiving breast milk with complementary foods, from seven countries in areas with previously documented deficient, sufficient, or excessive iodine intake in schoolchildren or pregnant women. Urinary iodine concentration (UIC) and Tg, total thyroxine, and thyrotropin were measured using dried blood spot testing.
Results:
Median UIC ranged from 48 μg/L (interquartile range 31–79 μg/L) to 552 μg/L (interquartile range 272–987 μg/L) across the study sites. Median Tg using dried blood spot testing was high (>50 μg/L) at estimated habitual iodine intakes <50 μg/day and >230 μg/day. Prevalence of overt thyroid disorders was low (<3%). Yet, subclinical hyperthyroidism was observed in the countries with the lowest iodine intake.
Conclusions:
Tg is a sensitive biomarker of iodine intake in 6- to 24-month-old infants and follows a U-shaped relationship with iodine intake, suggesting a relatively narrow optimal intake range. Infants with low iodine intake may be at increased risk of subclinical thyroid dysfunction. In population monitoring of iodine deficiency or excess, assessment of iodine status using UIC and Tg may be valuable in this young age group.
Introduction
Universal salt iodization (USI) is the most effective means to assure optimal population iodine status (1 –3). In countries where USI is well implemented, iodine requirements of young infants are covered through breast milk (4), but USI may not meet dietary requirements in later infancy when infants transition from breast milk to solid food (5). Home-prepared complementary foods are generally low in native iodine (6). Pediatric guidelines recommend no extra salt be given to infants during the first year and that cow's milk should not be introduced as a drink before the age of 12 months (7). The dietary sources of iodine for this age group may thus be limited.
The weaning period begins at about four to six months of age, and covers the latter part of the first 1000 days of life, which are the most important for both growth and cognitive development (8,9). The rate of thyroid hormone synthesis is high, and consequently the requirement for iodine is increased (10,11). It has previously been shown that weaning infants are at risk of iodine deficiency (12) and may be vulnerable to thyroid dysfunction with chronic excess iodine intake (13). Yet, data reporting on iodine intake in this age group are sparse (14,15). Thyroglobulin (Tg) has proved to be a reliable biomarker of iodine intake and is recommended by the World Health Organization (WHO) to complement urinary iodine concentration (UIC) measured in spot urine samples in population surveys (2). A U-shaped association between iodine intake and thyroid function has been demonstrated for school-age children and pregnant women (16 –18). Population thresholds for UIC reflecting optimal iodine nutrition have been established in these groups (2). The WHO applies the same lower UIC threshold for 6- to 24-month-old infants as for school-age children, but the evidence for this recommendation is weak. Considering the high dietary iodine requirements per kilogram of body weight at this age (19,20) and the low urine volume (0.5 L) (21), the UIC thresholds reflecting adequate iodine intake compared to older children may be higher.
The aim of the study was to assess the association of low and high iodine intakes with Tg and thyroid function in weaning infants. It was hypothesized that thyroid function follows the same U-shaped association in 6-to 24-month-old infants as observed in other population groups, and that this association may be used to estimate the optimal intake range. The data can also inform and guide recommendations on iodine content in complementary foods in this age group.
Methods
Subjects
All infants were apparently healthy, aged between 6 and 24 months, resident at the respective study site for >12 months (or since birth), and consuming both breast milk and complementary foods at inclusion. Various terminology exists for infants during this phase of dietary transition. For the purposes of this article, 6- to 24-month-old infants receiving both complementary foods and breast milk are hereafter referred to as “weaning infants.”
Weaning infants were recruited in seven countries from areas with previously documented deficient, sufficient, or excessive iodine intake. The study sites were purposefully selected based on UIC in school-age children or pregnant women populations for whom intake thresholds are established, and are not considered representative of national status in any country. Sites were as follows (location, median UIC, population): (i) Amizmiz, Morocco, 32 μg/L (n = 245 pregnant women) (22); (ii) West Kiang, Lower River Region, The Gambia, 50 μg/L (n = 203 school-age children; Wegmuller R, Andersson M, unpublished data, 2013); (iii) Dipolog City, Zamboanga del Norte, The Philippines, 68 μg/L (n = 342 school-age children) (23); (iv) Linfen, Shanxi Province, P.R. China, 201 μg/L (n = 388 school-age children) (4); (v) Zagreb, Croatia, 205 μg/L (n = 159 school-age children) (24); (vi) Kinondoni, Dar-es-Salaam, Tanzania, 520 μg/L (n = 317, school-age children) (25); (vii) Kibwezi, Makindu County, Kenya, 424 μg/L (n = 284, school-age children) (25).
The study design was cross-sectional with convenience sampling. Allowing for a 15% margin for subject withdrawal, the aim was to enroll 300 participants per group per study site in order to determine the median UIC per group with a 90% confidence and 5% error (26). The same sample size and precision was estimated as sufficient to also assess Tg as a co-primary outcome based on proportions of subjects of school-age with an elevated Tg >40 μg/L (since Tg thresholds are not defined in 6- to 24-month-old infants) (27).
The study finally recruited 232 eligible infants in Morocco, 95 in The Gambia, 105 in The Philippines, 324 in P.R. China, 38 in Croatia, 275 in Tanzania, and 320 in Kenya. In Croatia, the desired sample size could not be reached within the set recruitment period; these data and the data from China are part of a larger study (4), as are those from Tanzania and Kenya (25). The sites in The Gambia and The Philippines were pilot studies for a randomized controlled trial that was withdrawn after the pilot phase (Trial Identification NCT02421653). Sample sizes for these pilot studies were set at 100.
Ethical approval was obtained from the Ethics Review Committee of the ETH Zurich (Zurich, Switzerland), and the corresponding local institution in each host country. Data were collected between 2015 and 2017.
Methods
Following inclusion, a questionnaire was administered in the local language to each parent or guardian to assess weaning practices, exposure of the weaning infant to iodine from iodized salt, fortified complementary foods and native iodine-containing foods, and household use of iodized salt. Anthropometric assessment was conducted in duplicate using standard methods (28). Body weight was measured to the nearest 0.1 kg using a Seca baby scale (Seca 384; Seca, Hamburg, Germany) and length to the nearest 0.1 cm using a UNICEF length board (UNICEF Supply Division) or Seca foldable height board. These measurements were not taken in P.R. China or Croatia. Weight-for-length (WLZ), weight-for-age (WAZ), and length-for-age (HAZ) Z-scores were calculated based on the WHO age- and sex-specific Child Growth Standards (29) using Anthro software v3.2.2 (World Health Organization, Geneva, Switzerland). Three infants from The Gambia and two from Kenya with a WLZ <−3 or mid upper arm circumference (MUAC) <115 mm were excluded n = 3 (30), and they were referred for medical assistance per study protocol. Otherwise, median Z-scores were greater than the WHO cutoff of <−2 to indicate low WAZ or HAZ (29).
Spot urine samples were collected to determine population iodine status by UIC. Samples were collected at any time of the day except the first morning void into a clean plastic cup or, for infants using nappies, using a pad collection system (Sterisets Newcastle Urine Collection Pack; Sterisets International B.V., Oss, The Netherlands) (31). Samples were aliquoted into three 2.0 mL Eppendorf tubes (Eppendorf, Hamburg, Germany), and stored at −20°C until analysis. On the same day, trained laboratory technicians or nurses collected finger or heel-prick dried blood spot (DBS) samples onto filter paper collection cards (IDBS-226; Perkin Elmer, Norwalk, CT), which were dried at room temperature, sealed in plastic bags with a desiccant, and stored frozen at −20°C until analysis. Blood spots contained 50 μL of whole blood. DBS-Tg, DBS-thyrotropin (TSH), and DBS-total thyroxine (TT4), used to assess thyroid function and prevalence of dysfunction, were measured.
Laboratory analyses
All sample collection materials were tested for iodine contamination (31). All analytical procedures were validated using external control samples and certified standard reference materials where available.
UIC
UIC were measured in the corresponding country or at the Laboratory of Human Nutrition of the ETH Zurich using a modified version of the Sandell–Kolthoff method (32). Each participating laboratory participates in and successfully fulfills the quarterly external validation requirements of the Program to Ensure the Quality of Urinary Iodine Procedures (U.S. Centers for Disease Control and Prevention, Atlanta, GA). The inter-assay variation determined at the Laboratory of Human Nutrition, ETH Zurich, was 4.6% at 67 ± 3 μg/L for lower urine control samples and 3.2% at 205 ± 7 μg/L for higher urine control samples.
DBS samples
DBS-Tg was measured at the Human Nutrition Laboratory of the ETH Zurich using a DBS-Tg enzyme-linked immunosorbent assay, as previously described (33). Serum control samples (Liquicheck Tumor Marker Control, LOT.23911, 23912, 23913; Bio-Rad, Hercules, CA) were used as standards for the DBS Tg assays. In-house DBS samples were used for quality control. The intra-assay variation was 18.3% at 25.8 ± 4.7 μg/L (n = 96), 11.8% at 51.7 ± 6.2 μg/L (n = 96), and 12.7% at 72.0 ± 9.1 μg/L (n = 31). At the time of writing, no current reference range has been defined for DBS-Tg in weaning infants.
DBS-TSH and DBS-TT4 concentrations were measured at the University Children's Hospital Zurich (Swiss Newborn Screening Laboratory and Children's Research Center, Zurich, Switzerland) using an automated time-resolved fluoroimmunoassay method and a Genetic Screening Processor (GSP) machine (2021-0010; PerkinElmer, Turku, Finland) and related GSP Neonatal TSH/T4 kits (PerkinElmer, Turku, Finland). Kit-specific controls were used for the analysis, with an intra-assay variability for TSH of 9.1% at 0.92 ± 0.08 mIU/L (n = 26) and 6.8% at 10.20 ± 0.69 mIU/L (n = 30) and for TT4 of 7.4% at 49.5 ± 3.6 nmol/L (n = 28), 14.0% at 106.2 ± 14.9 nmol/L (n = 28) and 6.0% at 221.1 ± 13.3 nmol/L (n = 28). We applied kit-specific reference ranges to the data: DBS-TSH 0.4–4.0 mIU/L and DBS-TT4 65–165 nmol/L. Data were recorded as being under or over these thresholds, and used to estimate prevalence of thyroid dysfunction in the study populations, defined as: subclinical hypothyroidism—elevated DBS-TSH, normal DBS-TT4; overt hypothyroidism—elevated DBS-TSH, low DBS-TT4, or DBS-TSH >10 mIU/L, normal tT4; subclinical hyperthyroidism—low DBS-TSH (0.1–0.4 mIU/L), normal DBS-TT4; subclinical hyperthyroidism with suppressed TSH—low DBS-TSH (<0.1 mIU/L), normal DBS-TT4; borderline overt hyperthyroidism—TSH 0.4 mIU/L, normal DBS-TT4; overt hyperthyroidism—low DBS-TSH (0.1–0.4 mIU/L), elevated DBS-TT4; and overt hyperthyroidism with suppressed TSH—low DBS-TSH (<0.1 mIU/L), elevated DBS-TT4.
Statistical analyses
Statistical analyses were performed using Microsoft Excel 2011 (Microsoft Corp., Redmond, WA) and IBM SPSS Statistics for Windows v23 (IBM Corp., Armonk, NY). UIC was the primary outcome parameter, and DBS-Tg, -TSH, and -TT4 and prevalence of thyroid function disorders were secondary outcomes. Further outcomes included information gathered from questionnaires.
Data normality was assessed using Kolmogorov–Smirnov and Shapiro–Wilk tests, a skewness of <1, and visually using Q-Q and P-P plots; non-normal data were log-transformed. For variables with outcomes <1 (DBS-Tg and DBS-TSH), 1 was added to all values before transformation. DBS-Tg values <0.91 μg/L, the limit of detection of the assay (33), were suppressed. No other outliers were removed. All normally distributed data are described as the mean ± standard deviation (SD), and skewed data as median (interquartile range [IQR]), unless otherwise described. Skewed data were bootstrapped to obtain robust confidence intervals.
The daily iodine intake was estimated using UIC, assuming an average urine volume of 0.5 L (21) and an iodine excretion rate of 87% of total daily iodine intake per child (19). Group differences were assessed using one-way analysis of variance for normally distributed data with Games–Howell post hoc tests for groups with unequal sizes or, for skewed data, the Kruskal–Wallis test with pairwise post hoc analysis. Continuous variables were correlated using Pearson's correlation coefficient (r) for normal or log-transformed normal data, or Kendall's tau-b (τb) for correlations involving skewed data. Group differences for prevalence were compared using the chi-square test, followed by the z-test to check for significant differences between individual values (Bonferroni correction). The association between DBS-Tg and UIC per study site is illustrated by a second-order polynomial trend line added to show best fit, and by a Loess smoothed line (with 75% of points to fit) for these variables plotted as continuous data. Significance was set at p < 0.05.
Results
A total 1543 eligible infants were recruited (M age = 12.2 ± 4.6 months). The general characteristics of infants per country are given in Table 1.
Subject Characteristics per Study Site
Data are median (IQR) or mean ± SD or % of n. Significance was set at p < 0.05.
Data were compared by 1Kruskall–Wallis test with pairwise post-hoc comparisons; 2one-way analysis of variance with Games–Howell post-hoc tests; 3Pearson's chi-square test with Bonferroni post-hoc tests.
Outcomes with the same superscript letters are not significantly different (p > 0.05). p corresponds to the overall significance for that outcome. Daily iodine intake is estimated using UIC, a urine volume of 0.5 L (21), and an iodine excretion rate of 87% (19).
UIC, urinary iodine concentration; WLZ, weight-for-length; HAZ, length-for-age; WAZ, weight-for-age; n, total sample size per measurement; NA, data were not taken in this country or not applicable; n.s., not significant.
UIC, estimated iodine intake, and weaning practices
Infants with a range of different iodine intakes were recruited in this study. Median UIC ranged from 48 μg/L (IQR 31–79 μg/L) in Morocco to 552 μg/L (IQR 272–987 μg/L) in Kenya (p < 0.001; Table 1). The corresponding estimated iodine intakes ranged from 21 μg/day (IQR 14–34 μg/day) to 233 μg/day (IQR 145–494 μg/day), assuming an iodine excretion rate of 87% (19) and urine volume of 0.5 L (21). UIC correlated negatively with infant age in P.R. China (τb = −0.148, p < 0.001) but not elsewhere.
The main source of dietary iodine was likely breast milk. In countries with data, most infants were breast-fed more than six times a day (Table 1). However, UIC was not associated with breast-feeding or complementary food intake. In Kenya and Tanzania, 94% and 74% of infants, respectively, received a cereal-based porridge (maize, wheat, cassava). In Morocco, 36% of infants received Smida (semolina bread) and 33% fruit- and/or vegetable-based foods (data from Morocco, Tanzania, and Kenya only) as first weaning foods. In Morocco and Kenya, 26% and 21% of infants received dairy foods (cow's or goat's milk, yoghurt or fromage frais [unripened cheese]) as first weaning foods. More than half of all families added salt to infant foods. Use was equally high for infants <12 months as for older infants, except in Croatia (Table 1). There were no differences in UIC between infants who were reported to consume food from the family table or not, or between households who reported use of iodized salt or not.
Thyroid function
Median DBS-Tg, DBS-TSH, and DBS-TT4 are presented in Table 2. DBS-Tg was highest at study sites with the lowest and highest median UIC (p < 0.001), respectively, indicating a U-shaped association (Table 2 and Fig. 1A and B). DBS-TSH and DBS-TT4 differed across study sites (p < 0.001) and correlated with UIC (τb = 0.15, p < 0.01; τb = 0.05, p < 0.05, respectively) in the overall sample. However, the associations lost significance when tested per study site. Similarly, DBS-TSH and DBS-TT4 were correlated with DBS-Tg (τb = 0.07, p = 0.001; τb = 0.09, p < 0.001, respectively) in the overall sample. Per study site, significant correlations were observed between DBS-TSH and DBS-Tg for the Philippines (τb = 0.20, p = 0.047) and Tanzania (τb = 0.17, p = 0.001), and DBS-TT4 and DBS-Tg for the Philippines (τb = 0.35, p < 0.001) and Kenya (τb = 0.08, p = 0.045).
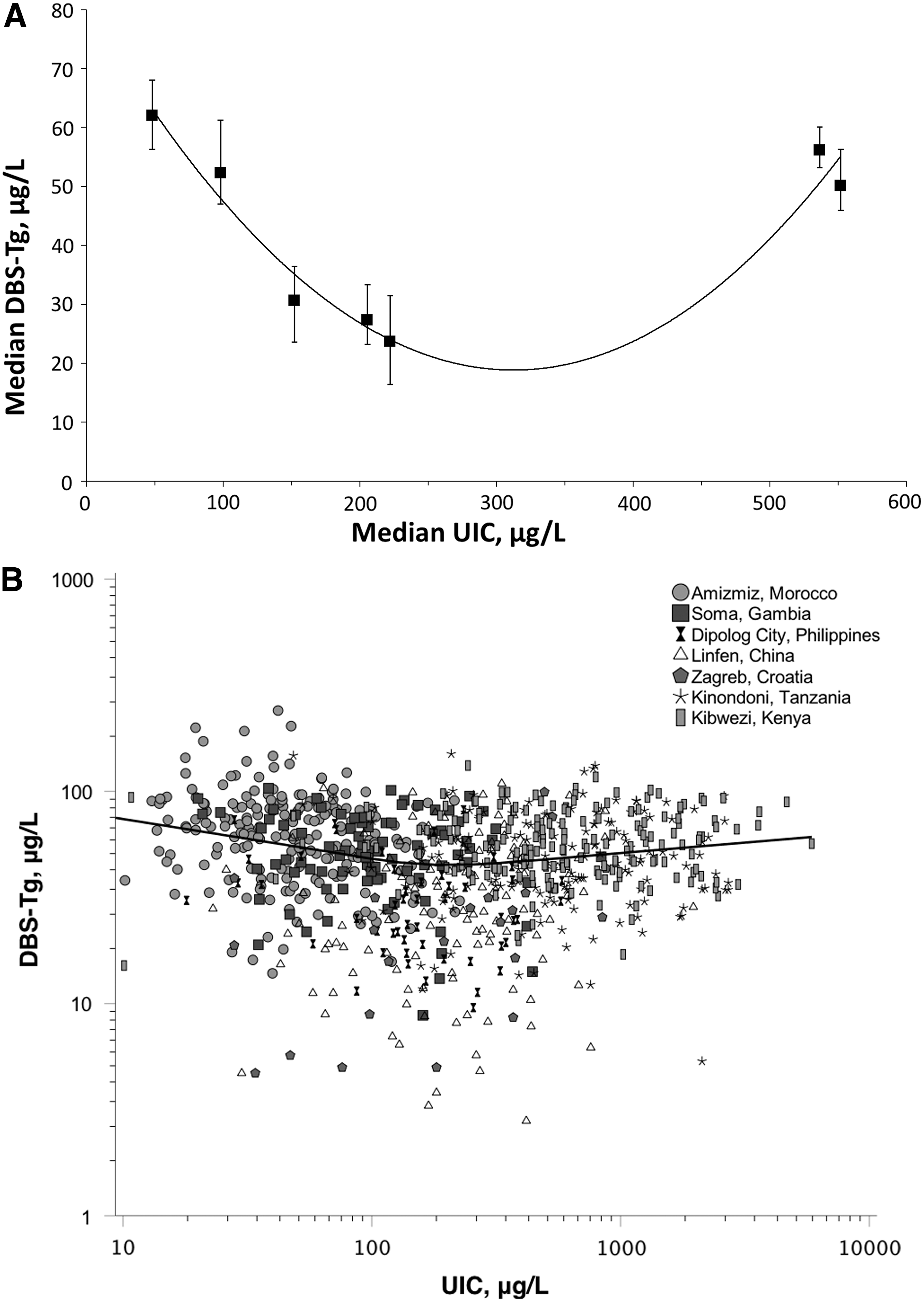
Association between urinary iodine concentration (UIC; μg/L) and thyroglobulin measured using dried blood spot testing (DBS-Tg; μg/L) (
Thyroid Function and Associated Disorders per Study Site
Data are median (IQR) or % of n. Significance was set at p < 0.05.
Data are compared by 1Kruskall–Wallis test with pairwise post-hoc comparisons; 2Pearson's chi-square test with Bonferroni post-hoc tests.
Subclinical and overt hyperthyroidism with TSH 0.1–0.3 mIU/L; no infant had a suppressed TSH <0.1 mIU/L.
Outcomes with the same superscript letters are not significantly different (p > 0.05). p corresponds to the overall significance for that outcome.
DBS, dried blood spot; Tg, thyroglobulin; TSH, thyrotropin; TT4, total thyroxine.
In the overall sample, DBS-Tg showed a negative correlation with infant age (τb = −0.05, p = 0.018), though a correlation at study site level was only seen in Morocco where the association was positive (τb = 0.10, p = 0.023). No association was observed in any of the other study sites. There were no differences in median DBS-Tg with breast-feeding, intake of solid foods, or reported household iodized salt use, except for Tanzania where DBS-Tg was higher in infants whose household reported using iodized salt (p = 0.005).
Prevalence of thyroid disorders was overall low, except for subclinical hyperthyroidism with a median DBS-TSH between 0.1 and 0.4 mIU/L, which was highest in Morocco (p < 0.05; Table 2). There were no infants with a suppressed TSH (<0.1 mIU/L).
Discussion
This is the first study to report iodine status and thyroid function in weaning infants aged 6–24 months across a broad spectrum of iodine intakes.
The same U-shaped association was observed between UIC and Tg concentrations as documented in other population groups (16 –18). However, in this age group compared to older children and adults, the optimal iodine intake range appears narrow. Median Tg was high (>50 μg/L) at estimated average habitual iodine intakes <50 μg/day and at intakes >230 μg/day, whereas in other population groups, the thyroid appears to maintain normal activity over a broader range of iodine intakes (16,17).
The dietary iodine requirement for infants aged 6–24 months is poorly defined. The Institute of Medicine of the U.S. National Academy of Sciences recommends an adequate intake of 130 μg/day and an upper level of 200 μg/day (20). The WHO recommended nutrient intake stipulates 90 μg of iodine per day from birth until 59 months (2). Though this study was not designed to define the optimal iodine intake, the data presented suggest that the median UIC threshold of 100 μg/L defining adequate iodine nutrition in this group may be too low. The Tg concentration was markedly elevated in populations with an habitual iodine intake equivalent to this UIC. The results suggest that the median UIC range reflecting optimal iodine nutrition in young infants may be higher than for older children. Further studies are warranted to establish the dietary requirements and the optimal median UIC range in order to define adequate population iodine nutrition.
Tg is widely recognized to be an effective biomarker of iodine status (17,34 –36), and this study shows that this also applies to 6- to 24-month-old infants. In euthyroid populations with a sufficient iodine intake, median serum Tg is typically around 10 μg/L (37 –39). Yet, in the present iodine-sufficient infant populations, median Tg ranged from 24 to 30 μg/L. Circulating Tg levels are high in early infancy but fall over the first year of life, likely reaching concentrations typical of adults by about six months to two years of age (40,41). Though normative pediatric reference ranges for Tg are derived over wide age ranges and the actual age at which Tg stabilizes is uncertain, the results generally agree. In the overall sample, a weak negative correlation was observed between Tg and infant age. No age-specific reference range is available for the DBS-Tg assay used in this study. Thus, the prevalence of elevated Tg could not be calculated.
Tg, the protein scaffold for thyroid hormone synthesis, is intricately involved with thyroid cell function at all levels (42). Following iodination of tyrosine residues within Tg and hormone synthesis in the colloid, endocytosis of Tg back into the thyrocyte follows two pathways: either lysosomal proteolysis to release thyroid hormone, or transcytosis through the thyrocyte intact. This pathway is thought to involve the transporter protein megalin (43). The expression of both Tg and megalin are upregulated by TSH stimulation (35,43) and provide important intracellular regulation (42). Correlations were observed between Tg and TSH, and Tg and TT4, though they were generally weak.
In this study, a higher prevalence of hypothyroidism was expected at study sites with lower habitual median iodine intakes. Surprisingly, the data revealed a higher prevalence of subclinical hyperthyroidism in infants in Morocco, The Gambia, and The Philippines (p < 0.05). A high prevalence was also found in Croatia, but the sample size was small. Further, no infants with clinically important subclinical hyperthyroidism were found (i.e., with a suppressed TSH <0.1 mIU/L). Although the etiology of hyperthyroidism is diverse, clinical juvenile hyperthyroidism is rare and transitory, and usually associated with transfer of maternal autoimmunity (40,44,45). Graves' disease affecting neonates would therefore not be expected in the present age group, as maternal TSH receptor-stimulating antibodies are usually cleared by three months of age (40,46).
In countries where maternal iodine status is borderline deficient, studies indicate that weaning infants may be at risk of inadequate iodine intake (12,47,48). A national survey in mother–infant pairs (n = 507) in Switzerland where the median breast milk iodine concentration (BMIC) was low (50 μg/L) found mild deficiency in infants aged 6–24 months receiving breast milk and complementary foods (12). In-depth analysis of different dietary patterns showed that fortified infant formula milk plays a pivotal role in dietary iodine provision to infants in this setting. The BMIC observed in Swiss women is comparable to that measured in lactating women six months postpartum in The Gambia (39 μg/L; n = 186) (49), and nine months postpartum in Morocco (26 μg/L; n = 234) (50). More than 80% of weaning infants in Morocco and The Gambia in the present study were breast-fed six times a day or more. However, USI coverage and access to fortified complementary foods were low in these countries. In the Philippines, although the household coverage of iodized salt in Dipolog City was low, processed foods may be produced with iodized salt. This contrasts with Switzerland, where household coverage is high but use of iodized salt in processed foods is voluntary. In Burkina Faso, where breast-feeding rates are similar to those in Morocco and The Gambia (97% at 18 months) (51,52), the geometric mean UIC in 18-month-old infants was 310 μg/L (n = 80), likely attributed to mandatory USI and subsequent adequate BMIC (51). A recent multi-country study across sites with good coverage of adequately iodized salt (≥15 mg/kg) confirmed that USI, when well enforced, meets the needs of both 0- to 6-month-old and 7- to 24-month-old infants (4).
Less is known about the iodine intake and thyroid function of infants in areas with high iodine intake. In Kenya, the median BMIC was high (240 μg/L; n = 126) (25). Breast milk is the likely principal source of iodine intake for these infants, and the complementary weaning foods described are likely low in native iodine. Yet, mothers reported adding salt to infant foods, and it was recently described that elevated iodine intakes at the study sites in Kenya and Tanzania are likely due to a combination of over-iodized salt and iodine-concentrated ground water (25). Additional iodine intake by weaning infants in these settings, such as that included in micronutrient powders (53), may not be justified.
Strengths of this study include recruitment of infants with a wide range of habitual iodine intakes. However, the study was limited by the lack of a population with habitual intakes of around 200 μg/day (i.e., a UIC of 300–400 μg/L), though the data in both Figure 1B and elsewhere in the literature support the present findings. In Burkina Faso, 80 infants aged 18 months had a geometric mean UIC of 310 μg/L [CI 227–425 μg/L] and a geometric mean serum Tg of 26.1 μg/L [CI 23.3–29.0 μg/L] (51). A cross-sectional study in 568 Nepalese infants aged 6–24 months described a median UIC of 407 μg/L (IQR 312–491 μg/L) and a geometric mean serum Tg of 21.7 μg/L [CI 20.4–22.9 μg/L] (13). In the Saharawi refugee camps of Western Algeria, 289 infants with a median age of 31.4 months (IQR 25.3–35.1 months) had a median UIC of 458 μg/L (IQR 275–1026 μg/L) and median serum Tg of 38.4 μg/L (range 10.7–158.0 μg/L) (54). The study was also limited by small sample sizes in Croatia, The Gambia, and The Philippines due to strict inclusion criteria, though results agree with previous studies with larger sample sizes (4,25). Urinary creatinine concentration was not measured, and estimates of daily iodine intakes are based on UIC and an average urine volume of 0.5 L (21). Further, Tg antibodies were not measured, although autoimmunity in later infancy is likely rare, as previously described. Finally, for full interpretation, the data lack measurement of T3, which may increase at low iodine intakes.
Conclusions
The association between UIC and Tg concentration follows the same U-shaped association in 6- to 24-month-old weaning infants as in other population groups. However, the present data suggest the optimal intake range is narrower than in older children or adults. This study confirms that the utility of Tg as a biomarker of iodine intake is extended to 6- to 24-month-old weaning infants and children, though its use as a predictor of thyroid dysfunction remains to be assessed. The prevalence of thyroid disorders was low in the present study, and while weaning infants with low iodine intake were at an increased risk of subclinical hyperthyroidism, at higher intake, increased Tg concentrations may be part of a physiologic mechanism to adapt to low and high intake. It is suggested that if deficient or excessive intakes are recorded in population iodine surveys on school-age children, monitoring and surveillance is extended to this age group. Criteria to define optimal iodine nutrition in this age group are urgently needed.
Footnotes
Acknowledgments
We would like to sincerely thank the following persons for their implication in this study: Fatma Abdallah, Khadija Akhiayt, Kabiru Ceesay, Francesca Chepkirui, Susanne Dold, Annemarie Geutjes, Juma Peter Kaswahili, Michael Maganga, Eusebeia Mendoza, Mohammed Ngum, Ema Parian, Cherry Maramag, Aimad Meghrani, Soujaina Ourhou, Johsua Saltiban, Katja Schoenenberger, Seedy Singateh, Manasi Shrouti, Kevin Szillat, Juliawati Untoro, and entire field teams in The Gambia, Kenya, The Philippines, and Tanzania. We also wish to thank Dipolog City Health Office, the Direction Régionale du Ministère de la Santé Marrakech-Safi, Kibwezi Health Centre, the MRC Field Station Keneba, The Municipal Council of Kinondoni, Dar Es Salaam, Tanzania, and the Tanzania Food and Nutrition Centre.
Funding for this study was provided by the United Nations Children's Fund New York, the U.S. Agency for International Development, the Global Alliance for Improved Nutrition, the Croatian Science Foundation Grant, and the ETH Zurich.
Author Disclosure Statement
No competing financial interests exist.