
Abstract
Introduction:
The lack of papillary structures and faint and/or unclear core features of follicular variant of papillary thyroid carcinoma (FV-PTC) may hamper the definitive fine needle aspiration biopsy -based diagnosis. Recently, the nomenclature of noninvasive encapsulated FV-PTC was revised to “noninvasive follicular thyroid neoplasms with papillary-like nuclear features” (NIFTP). However, it remains inconclusive whether or not the peptide patterns differ between NIFTP and encapsulated FV-PTC. The main objectives of this study were to investigate the viability of matrix-assisted laser desorption/ionization mass spectrometry imaging (MALDI MSI) in the pathological assessment of NIFTP and to evaluate the discriminatory power of MALDI MSI for the classification of classical variant of PTC (CV-PTC), NIFTP, and encapsulated FV-PTC.
Methods:
MALDI MSI was employed to investigate the changes in peptide profiles from 21 formalin-fixed paraffin-embedded (FFPE) tissue samples (n = 7 from each group of CV-PTC, NIFTP, and FV-PTC). Six out of seven FV-PTC FFPE tissue samples were encapsulated FV-PTC; only one was infiltrative FV-PTC. Liquid chromatography–tandem mass spectrometry was used for the identification of the peptide signals detected in MALDI MSI.
Results:
Using receiver operating characteristics analysis, 10 peptide signals distinguished NIFTP from normal thyroid parenchyma (area under the curve [AUC] >0.80). To evaluate the discriminatory power of MALDI MSI, statistically significant peptide signals (n = 88) within three groups were used for hierarchical clustering. The method had high discriminatory power for distinguishing CV-PTC from NIFTP and FV-PTC (encapsulated and infiltrative). The majority of the NIFTP and encapsulated FV-PTC were clustered together, indicating that NIFTP could not be distinguished from encapsulated FV-PTC. However, infiltrative FV-PTC FFPE tissue samples had the furthest distance from all the NIFTP cases. High signal intensities of S100-A6, vimentin, and cytoplasmic actin 1 were detected in FV-PTC, prelamin A/C in CV-PTC, and 60S ribosomal protein L6 and L8 in NIFTP tissues.
Conclusions:
MALDI MSI, a powerful tool combining histological and mass spectrometric data, enabled the differentiation of NIFTP from normal thyroid parenchyma. Although NIFTP is a recent definition that replaces noninvasive encapsulated FV-PTC, the peptide profiles of NIFTP and encapsulated FV-PTC were found to be similar.
Introduction
Papillary thyroid carcinoma (PTC) arises from follicular cells of the thyroid gland and has many histopathological variants, of which the classical variant of PTC (CV-PTC) is the most common (1). The papillary structures and cells with large nuclei and eosinophilic cytoplasm are definitive features of CV-PTC. In another PTC variant, namely follicular variant of PTC (FV-PTC), the papillary structures are absent, and the tumor forms follicles. Still, FV-PTC has nuclear changes that are reminiscent of PTC. However, the lack of papillary structures, faint and/or unclear core features may hamper the definitive diagnosis of FV-PTC and lead to subjective diagnoses in surgical pathology. Recently, the nomenclature for noninvasive encapsulated FV-PTC was revised and termed as “noninvasive follicular thyroid neoplasms with papillary-like nuclear features” (NIFTP) (2). The nomenclature was revised due to the indolent behavior of these lesions and to classify them as indolent neoplasms rather than a carcinoma.
The primary noninvasive diagnostic method of thyroid nodules is fine needle aspiration biopsy (FNAB) and the method is used to distinguish benign, malignant, and suspicious lesions. FNAB is especially useful for the diagnosis of PTC, which relies on five major diagnostic criteria: namely (i) enlarged, oval, and “irregular nucleus”; (ii) eccentric and often multiple micronucleoli; (iii) fine pale chromatin; (iv) longitudinal nuclear grooves; and (v) intranuclear pseudo- or cytoplasmic inclusions (3). Along with FNAB, clinical assessment and ultrasonography are considered to evaluate thyroid lesions.
FNAB, a gold standard screening method, is very rarely associated with complications, and the cytology results often allow to characterize the lesions and can avoid unnecessary surgical resections. Genetic and immunohistochemical markers can further improve the diagnostic accuracy of FNAB cytology. For example, mutations in the mitogen-activated protein kinase pathway are frequently altered in PTC. Specifically, the B-type Raf kinase (BRAF)V600E mutation is commonly found in CV-PTC, but it is rare in FV-PTC. This mutation is required for tumor progression and found to be associated with aggressive clinicopathological features of CV-PTC (4,5). Analysis for the presence of the BRAFV600E mutation in large thyroid carcinoma data sets revealed that the prevalence of BRAFV600E mutation is high in CV-PTC and tall cell variants of PTC (6,7). In addition, the presence of a BRAFV600E mutation predicts a malignant lesion in nodules with an indeterminate cytology (8). However, because of the low prevalence in nodules with an indeterminate cytology, other more sensitive methods are needed (9 –11).
Similarly, the results of proposed other genetic or immunohistochemical markers (alone or in combination) are greatly improved but still need further validation (12 –15). Therefore, the discovery of new potential markers remains an exciting area in thyroid pathology, particularly markers that allow to characterize indeterminate cytologies or that could discriminate lesions such as NIFTP from encapsulated and/or infiltrative FV-PTC.
Proteomics represents a powerful approach for the understanding of complex biological systems. In brief, proteomics enables identification and quantification of a large number of proteins in biological compartments. Such approaches have already enlightened some molecular pathways and specific target molecules involved in thyroid pathology (16,17). To the best of our knowledge, the specific proteomic profiles of histopathological variants of PTC and NIFTP have not been examined. Matrix-assisted laser desorption/ionization mass spectrometry imaging (MALDI MSI) is a proteomic technique offering several advantages over conventional approaches. MALDI MSI provides information on the spatial distribution of peptides and/or proteins in tissue sections (18). The method itself requires no homogenization before sample preparation and, thus, combines mass spectrometric data with histological features.
In this study, we have evaluated the use of MALDI MSI for further characterization of CV-PTC, NIFTP, and encapsulated FV-PTC. Formalin-fixed paraffin-embedded (FFPE) tissue sections from these three groups were analyzed to assess the discriminatory power of MALDI MSI, specifically focusing on the distinction of NIFTP from encapsulated FV-PTC using peptide profiles.
Materials and Methods
Materials
All chemicals used in this study were from Sigma-Aldrich (St. Louis, MO) and high performance liquid chromatography (HPLC) grade, except peptide calibration standard, conductive indium-tin-oxide (ITO)-coated microscope slides, and α-cyano-4-hydroxycinnamic acid (α-CHCA), all from Bruker Daltonics (Bremen, Germany), and trypsin gold, from Promega (Madison, WI).
Clinical material
Postoperative PTC tissues collected during thyroidectomy were used in this study. Thyroidectomy was performed between 2014 and 2017 at Acıbadem Maslak Hospital Istanbul, Turkey. Initially, 30 tissue samples were fixed in formalin after surgical procedures and embedded in paraffin. Those tissue samples were processed as routine pathology cases; a representative hematoxylin and eosin (H&E)-stained tissue section was evaluated by pathologists. Lesions other than thyroid cancer have not been evaluated, and medullary thyroid cancer, anaplastic thyroid cancer, and follicular thyroid cancer specimens were excluded from the study. Pathological confirmation of the aforementioned tissue types was based on the World Health Organization (WHO) Classification of Tumors of Endocrine Organs (19) and consensus diagnostic criteria for NIFTP (2). Two independent pathologists (F.T. and U.I.) confirmed the diagnosis.
Of the 30 FFPE tissue samples, 7 were diagnosed as NIFTP, 6 were diagnosed as encapsulated FV-PTC, and only 1 tissue sample was diagnosed as infiltrative FV-PTC, while the remainder of the samples consisted of CV-PTC (n = 16). For CV-PTC samples, BRAFV600E mutation analyses were performed and samples negative for the BRAFV600E mutation were selected (n = 7). The detailed clinical description for the FFPE tissue samples is given in Table 1. The study was approved by the Ethics Committee of the Acibadem University (ATADEK-2014-621). Informed consent was obtained from all subjects.
Description of the Tissue Samples (n = 21)
CV-PTC, classical variant of papillary thyroid carcinoma; FV-PTC, follicular variant of papillary thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasms with papillary-like nuclear features.
BRAFV600E mutation analysis
H&E-stained tissue specimens were assessed beforehand and areas containing tumor cores were selected. Four 5-μm-thick samples were sectioned from the selected tumor cores. DNA was extracted using the AmoyDx FFPE DNA Kit (Amoy Diagnostics Co., Ltd, China) according to the manufacturer's protocol and quantified using a NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific). The DNA concentration of samples to be amplified was >2 ng/mL. BRAFV600E mutation analysis was carried out using the CFX Connect Real-Time PCR Detection System (BioRad) and the AmoyDx BRAF V600 Mutations Detection Kit (Amoy Diagnostics Co., Ltd). Polymerase chain reaction conditions were performed with an initial denaturation at 95°C for 5 minutes, denaturation at 95°C for 25 seconds, annealing at 64°C for 20 seconds, and extension at 72°C for 20 seconds for 45 cycles. The results of BRAFV600E mutation test were interpreted according to the manufacturer's instructions.
MALDI MSI experiments and data analysis
The thyroid tissue samples were sectioned at 3 μm onto conductive ITO glass slides and prepared for measurement as outlined before (18). In brief, tissue sections were washed by immersion in xylene (100%), ethanol (100%, 70%, and 30%), and distilled water. Antigen retrieval was employed by heating the slides in 10 mM citrate buffer (pH 6) at 95°C. Trypsin was resuspended in 25 mM ammonium bicarbonate buffer at a concentration of 25 ng/μL and sprayed on the tissue using the SunCollect automatic sprayer (SunChrom, Friedrichsdorf, Germany). After trypsin application, slides were incubated in a temperature- and humidity-controlled environment at 50°C for 2 hours using SunDigest Incubation Chamber (SunChrom). A solution of α-CHCA matrix was prepared at a concentration of 7 mg/mL in 1:1 acetonitrile–water/0.1% trifluoroacetic acid/10 mM ammonium phosphate monobasic and was applied to the tissue surface by SunCollect automatic sprayer.
Samples were analyzed on a MALDI-TOF/TOF instrument (RapiFlex MALDI Tissue Typer; Bruker Daltonics) in positive-ion reflectron mode over the m/z range of 700 to 2600. Mass spectrometry (MS) data were acquired using 300 laser shots per spot and MALDI MS images were acquired with 50 μm × 50 μm spatial resolution. The calibration of the mass spectrometer was performed using Peptide Calibration Standard II. The total spectra obtained were baseline subtracted. SciLS Lab 2016 software (Bruker Daltonics) and FlexImaging V5.0 (Bruker Daltonics) were used for data analysis and ion image generation. Total ion current normalization was performed for signal intensity normalization. In this study, we have applied receiver operating characteristics (ROC) analysis and principal component analysis (PCA) using SciLS Lab and Perseus Software. The consecutive tissue sections were stained with H&E and scanned with an automated slide scanner (Mirax Scan; Zeiss, Germany). A schematic MALDI MSI experiment workflow is shown in Figure 1.

Schematic MALDI MSI experiment workflow. MALDI MSI, matrix-assisted laser desorption/ionization mass spectrometry imaging. Color images are available online.
Liquid chromatography–tandem mass spectrometry analysis
A NIFTP FFPE tissue previously used for MALDI MSI was selected for liquid chromatography–tandem mass spectrometry (LC-MS/MS) analysis and prepared for measurement as outlined in our previous publication (20). Peptide signals obtained and identified using LC-MS/MS were correlated with the peptide signals present within the MALDI MSI data set (n = 21). Identifications were accepted only if identification matched a MALDI MSI peptide signal with <100 ppm error and MSI peptide signal detected in at least five out of seven tissues per group.
Results
Clinical descriptions of the subjects included in this study are presented in Table 1. The study included 19 females and 2 males, with an average age (±SD) at diagnosis of 43.67 (±11.5) years. The male subjects belonged to the CV-PTC and encapsulated FV-PTC groups. The samples in the FV-PTC group included six encapsulated FV-PTC and one infiltrative FV-PTC. No lymph node and/or distant metastases was detected in any of the cases at the time of diagnosis. NIFTP cases (n = 7) were independently reviewed by two experienced pathologists to confirm the diagnosis, which was based on the consensus diagnostic criteria for NIFTP (2,19).
Diagnostic detection of NIFTP by MALDI MSI of peptides
Seven FFPE NIFTP specimens were analyzed by MALDI MSI to assess the technical usefulness of MALDI MSI of peptides as a diagnostic tool in the study of NIFTP. In each NIFTP FFPE tissue, a reference “NIFTP area” was detected by the pathologist. In Figure 2, a representative NIFTP specimen is shown. Using this representative NIFTP specimen, average tryptic peptide profiles from the NIFTP area and its surrounding normal thyroid parenchyma were generated (Fig. 3A). The PCA scores of the NIFTP and normal thyroid parenchyma are shown in Figure 3B. Next, we performed ROC analysis to evaluate potential discriminating peptides between NIFTP and normal thyroid parenchyma. ROC analysis revealed 10 peptide signals (area under the curve [AUC] >0.80), which enable the discrimination of NIFTP lesions arising in the context of normal thyroid parenchyma (Table 2).
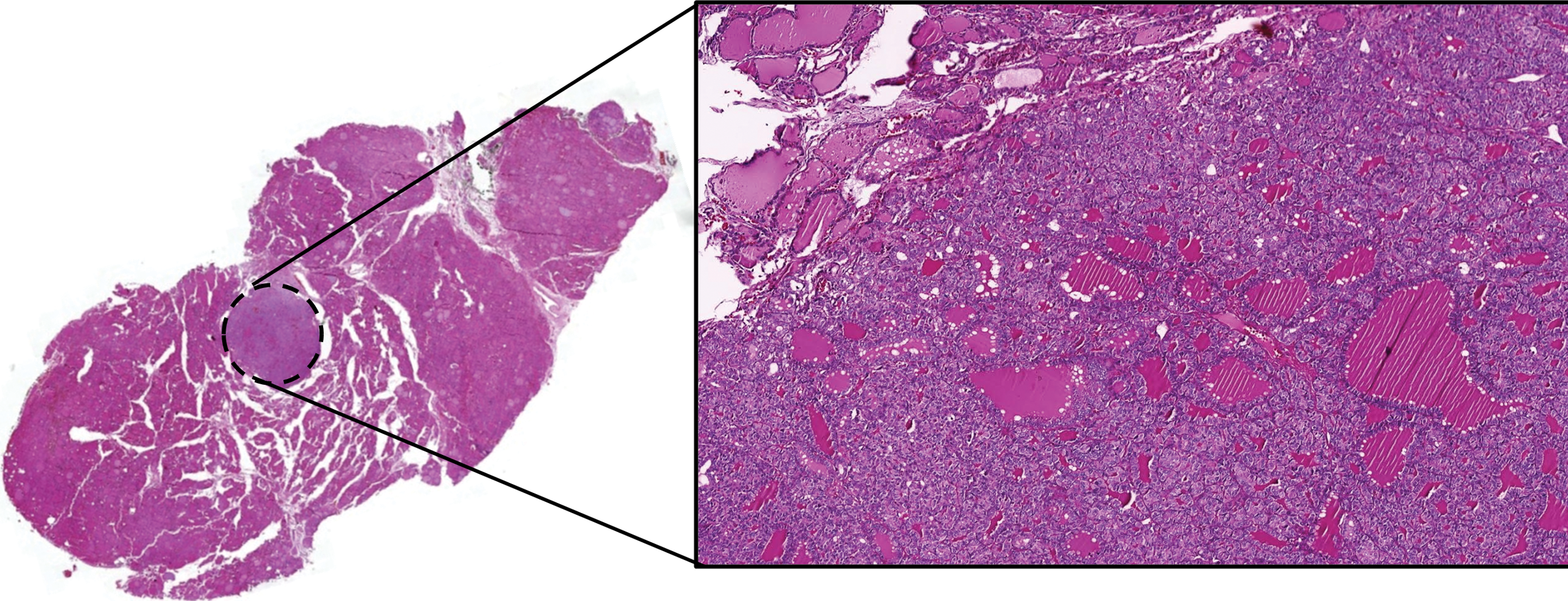
Representative H&E-stained NIFTP lesion. The lesion is encircled by black dash line. H&E, hematoxylin and eosin; NIFTP, noninvasive follicular thyroid neoplasms with papillary-like nuclear features. Color images are available online.

MALDI MSI of representative NIFTP lesion. (
Discriminatory Peptides Obtained from Receiver Operating Characteristic Analysis When Comparing Noninvasive Follicular Thyroid Neoplasms with Papillary-Like Nuclear Features Region with Normal Thyroid Parenchyma
AUC, area under the curve; LC-MS/MS, liquid chromatography tandem mass spectrometry; MALDI MSI, matrix-assisted laser desorption/ionization mass spectrometry imaging.
The identifications of these peptides are given in Table 3 and MS/MS spectra are shown in Supplementary Figures S1, S2, S3, S4, S5, S6, S7. Representative ion images and corresponding ROC curves of two peptides (m/z 894.40 and m/z 1190.64) are given in Figure 3C and D. Those two peptides—m/z 894.40 (m/z LC-MS/MS 894.430) and m/z 1190.64 (m/z LC-MS/MS 1190.638)—were identified as peroxiredoxin-1 and protein disulfide-isomerase A4, respectively (Table 3). These results show the capability of MALDI MSI of peptides to differentiate NIFTP lesions from normal thyroid parenchyma.
MS/MS Identifications of Peptides
PSM, peptide spectrum match; PEP, posterior error probability; MS/MS, tandem mass spectrometry.
Patterns of peptide profiles across PTC variants and NIFTP
CV-PTC and FV-PTC are known to be molecularly different; the main question of this study was whether it is possible to distinguish NIFTP from encapsulated FV-PTC (n = 6) and infiltrative FV-PTC using a proteomic approach (n = 1). Therefore, we sought to detect groups of peptides in the whole MALDI MSI data set. To accomplish this, we determined statistically significant peptide signals within three groups (n = 88) and clustered all samples with those significant peptides obtained from MALDI MSI. To determine peptides ubiquitously found in PTC variants and NIFTP lesions, we constructed common peptide profiles for all three tissue groups, each having seven FFPE samples. A peptide was considered as part of the common peptide profile if it was detected in at least five FFPE samples of every single tissue group.
The peptide signals (n = 88) used for classification were previously identified using LC-MS/MS and the identifications revealed that those peptides belonged to 31 different proteins (Fig. 4A). Identified proteins were further assessed for their functional categories on the basis of the Gene Ontology (GO) and PANTHER (Panther Classification System) databases. As shown in Figure 4B and C, a total of 31 proteins were grouped into several categories according to their classes and molecular functions. The major protein class consisted of nucleic acid binding proteins (48.6%), followed by cytoskeletal proteins (10.8%), hydrolases (8.1%), and enzyme modulator proteins (5.4%) (Fig. 4B). These proteins exhibit different molecular functions, of which the major functions are structural roles (40%), followed by nucleic acid binding properties (35%), and catalytic activities (17.5%) (Fig. 4C).

Thirty-one significantly different proteins between CV-PTC, FV-PTC, and NIFTP (p < 0.05). (
To evaluate the potential of using MALDI MSI to classify PTC variants (CV-PTC, encapsulated FV-PTC, and infiltrative FV-PTC) and NIFTP specimens, the identified 88 peptides of the aforementioned 31 proteins were used for hierarchical clustering analysis. The hierarchical clustering analysis revealed a clear separation between CV-PTC and other specimens (NIFTP and encapsulate/infiltrative FV-PTC). However, there was no clear distinction between NIFTP and encapsulated FV-PTC in hierarchical clustering and PCA (Fig. 5A, B). Interestingly, the only infiltrative FV-PTC case, which is denoted as FV-5 in Figure 5A, had the furthest distance from the NIFTP cases.
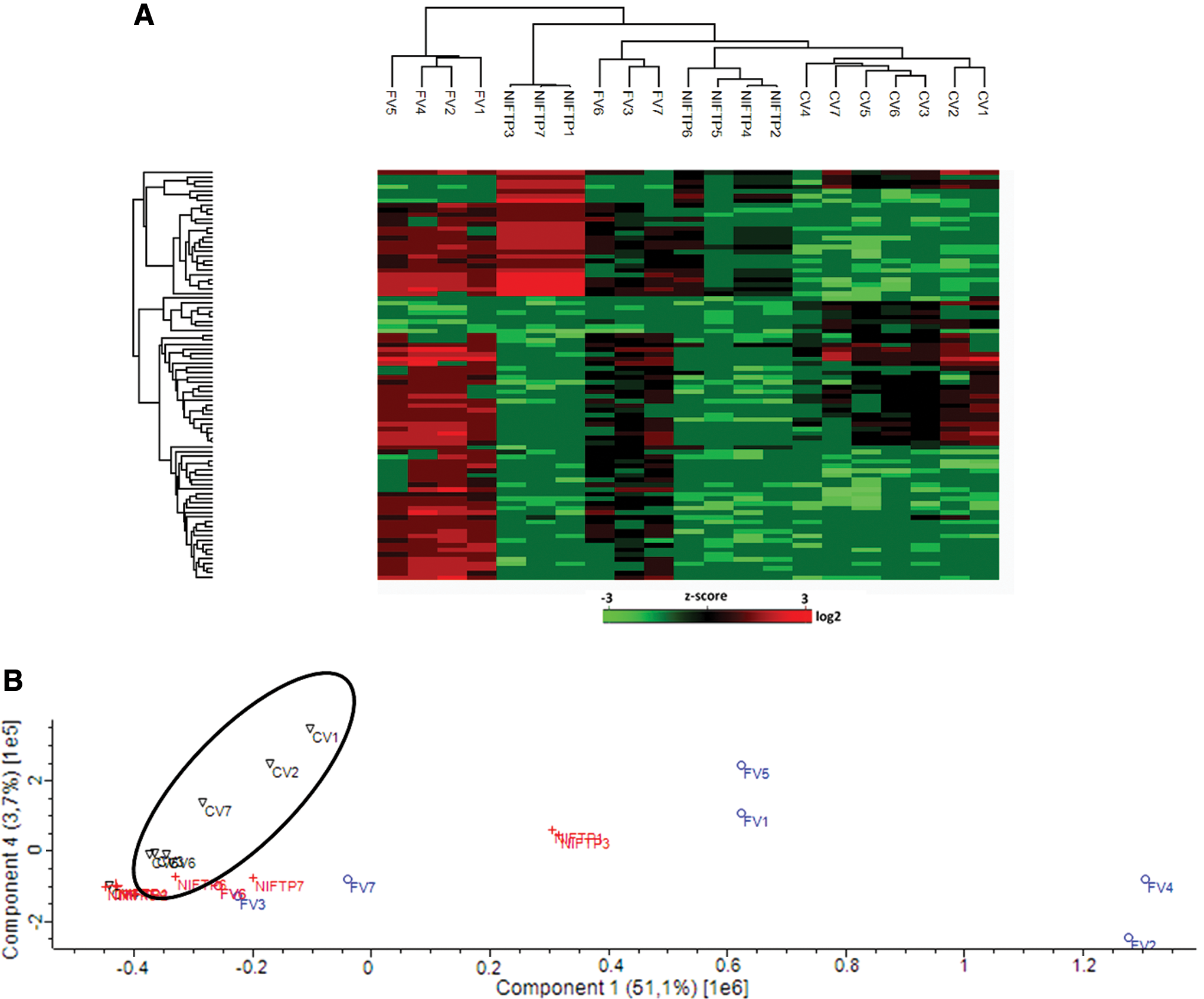
Discriminatory power of MALDI MSI. (
Detailed examination of encapsulated FV-PTC and NIFTP specimens on hierarchical clustering revealed that distribution of peptide signal intensities among the groups showed variations between each specimen. For example, representative peptide m/z 1377.75, which was identified as heterogeneous nuclear ribonucleoproteins A2/B1, showed relatively higher signal intensities in encapsulated FV-PTC and NIFTP than CV-PTC (p < 0.05). However, it was shown that the signal intensities for this specific peptide vary within the same group (Fig. 6A). Random selection of one FFPE specimen in each group with low signal intensity for this peptide represented almost similar ion images (Fig. 6B).
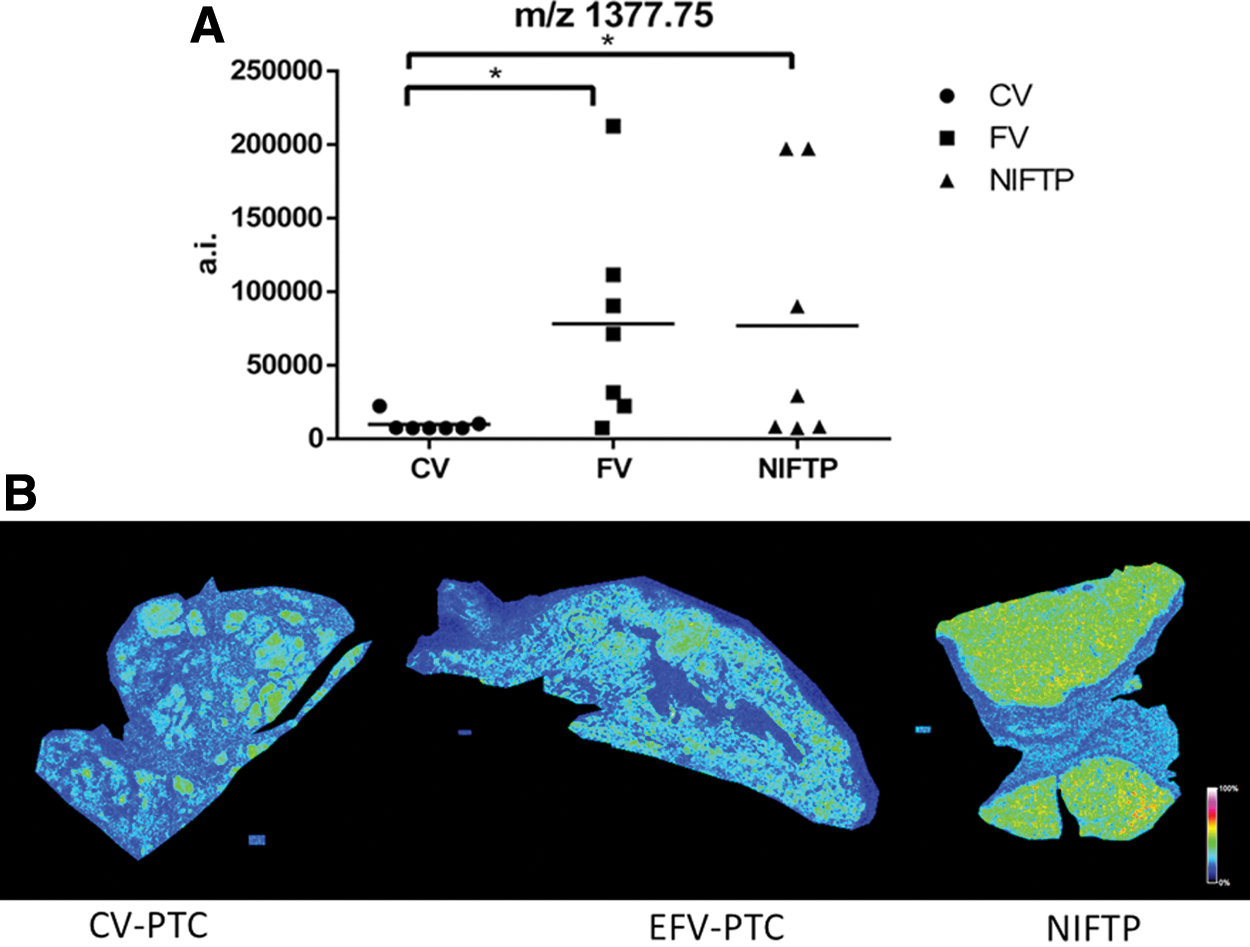
Representative peptide (m/z 1377.75) showing signal intensity variation within the same group. (
Peptide profile comparison of PTC variants and NIFTP
The tryptic peptide profiles obtained using MALDI MSI were further investigated to determine potential ions of differing intensities. ROC analysis revealed nine ions that were able to distinguish between PTC variants and NIFTP specimens (AUC >0.80). Of the nine ions, five ions were of higher intensity in encapsulated FV-PTC (m/z 915.48, 891.42, 1494.71, 1161.61, and 1177.61), whereas two ions were of higher intensity in CV-PTC (m/z 1729.92 and 1566.74) and two ions were of higher intensity in NIFTP (m/z 970.55 and 941.55) (Fig. 7). LC-MS/MS identifications of these discriminative ions are m/z 915.48 and m/z 891.42 as S100A-6, m/z 1494.71 as vimentin, m/z 1161.61 and m/z 1177.61 as actin-cytoplasmic I, m/z 1729.92 and m/z 1566.74 as prelamin-A/C, and m/z 970.55 and m/z 941.55 as 60S ribosomal protein L6 and L8, respectively (Table 3).
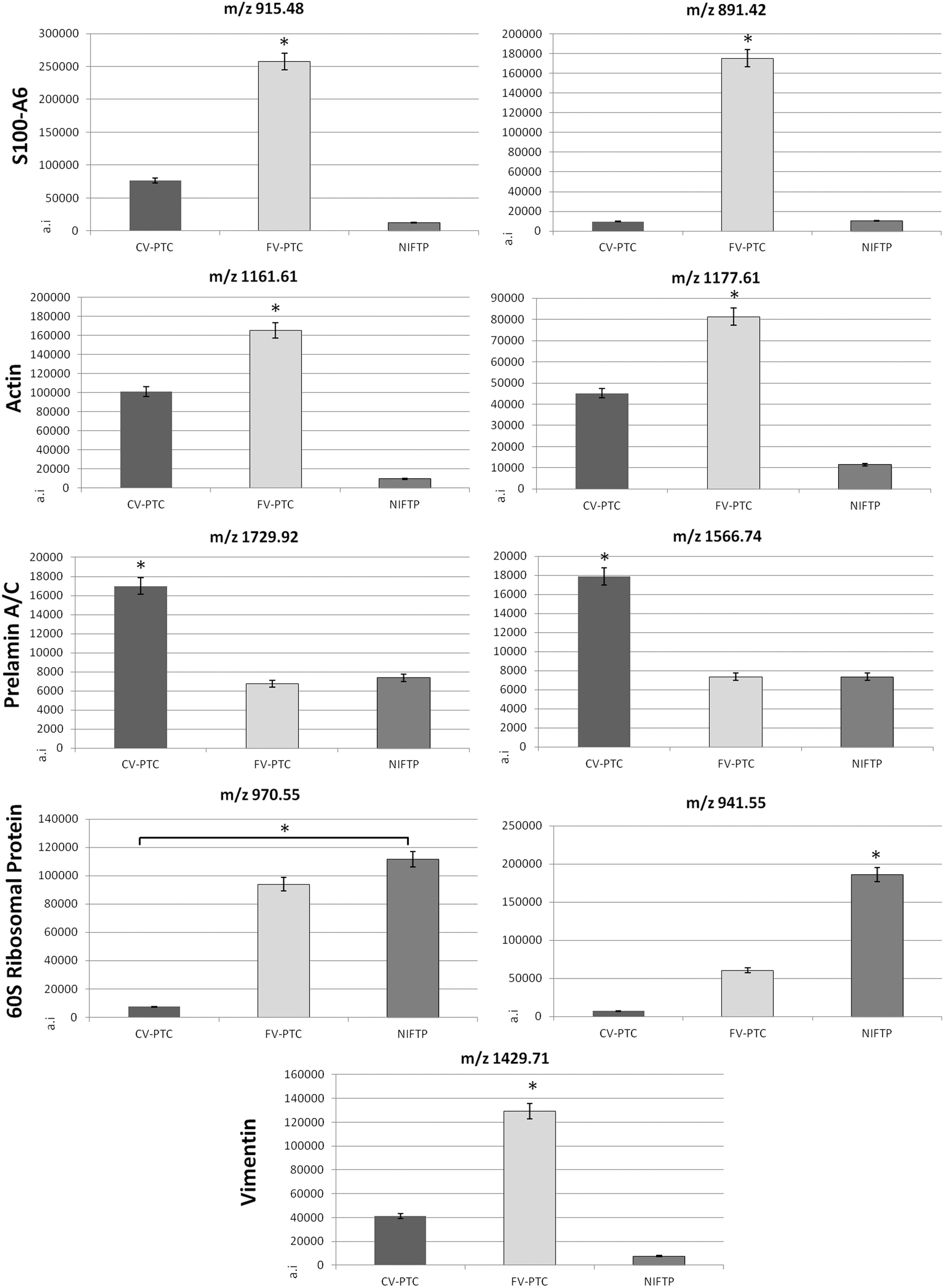
Mean ion intensities of the identified tryptic peptides that can discriminate PTC variants from NIFTP after ROC analysis. The asterisk denotes statistical significance at p < 0.05. Error bars represent SEM. PTC, papillary thyroid carcinoma; SEM, standard error of mean.
Discussion
MALDI MSI allows to bridge high-throughput “-omics” technologies and classical histology, and enables localization of peptides and proteins in several tissues, including thyroid cancer (18). MALDI MSI enables virtual microdissection by exporting spectra from the region of interests that are defined as “tumor” by pathologists based on the morphological architecture. Previous studies have highlighted the capability of MALDI MSI of peptides, proteins, and/or lipids on FFPE or fresh frozen thyroid tissue sections (21 –25). Although these studies are important for demonstrating the applicability of the method, there is currently no comprehensive proteomic study aimed at distinguishing peptide and/or proteome profiles of NIFTP, encapsulated FV-PTC, and infiltrative FV-PTC. To address this issue, we explored the feasibility of MALDI MSI in the pathological evaluation of NIFTP and encapsulated FV-PTC. In addition, we have added CV-PTC cases that were negative for the BRAFV600E mutation into the MALDI MSI data set. The CV-PTC cases were preferentially selected to have a compatible MALDI MSI data set, since FV-PTC and NIFTP cases harbor no BRAFV600E mutations.
Recently, “noninvasive encapsulated follicular variant of papillary thyroid carcinoma” was renamed as NIFTP based on an international multicenter consensus study demonstrating evidence for a low malignancy potential (2,19). In our study, NIFTP was clearly distinguished from the normal thyroid parenchyma using MALDI MSI. In addition, ROC analysis revealed 10 peptides with high discriminating power, thus indicating that MALDI MSI could be an alternative tool for the detection of specific markers for NIFTP lesions.
We evaluated statistically significant peptide signals (n = 88) within three groups that could be further used for hierarchical clustering analysis. LC-MS/MS identifications revealed that 31 proteins had differential signal intensities within CV-PTC, NIFTP, and encapsulated FV-PTC. From the viewpoint of protein classes, the top-ranked GO term consisted of nucleic acid binding proteins, followed by cytoskeletal, hydrolases, and enzyme modulator proteins. These findings are in agreement with our previous report, in which we used a mass spectrometry-based label-free quantification approach to investigate protein profiles of fresh frozen FV-PTC and CV-PTC tissues, and showed that almost 50% of the differentially increased proteins in CV-PTC had cytoskeletal, DNA, and receptor binding properties (26).
We next examined the similarity of individual CV-PTC, NIFTP, and FV-PTC (n = 6 encapsulated FV-PTC, n = 1 infiltrative FV-PTC) peptide profiles using unsupervised hierarchical clustering. In general, CV-PTC FFPE tissues converged into the same or closely related clusters. However, there was no clear separation between NIFTP and encapsulated FV-PTC FFPE tissues. Rather the two cluster groups of NIFTP and encapsulated FV-PTC showed a similar distribution. The morphological resemblance and the frequent presence of RAS mutations in NIFTP and encapsulated FV-PTC (27 –29) are consistent with the proteomic similarity of these lesions obtained using MALDI MSI.
Our study is limited in that the MALDI MSI data set included only one infiltrative FV-PTC, thus limiting the possibility of making inferences about peptide and/or proteomic profile differences between infiltrative FV-PTC and encapsulated FV-PTC, or between infiltrative FV-PTC and NIFTP. However, in the hierarchical clustering analysis, the only infiltrative FV-PTC had the furthest distance from the NIFTP cases and was clustered almost separately from the encapsulated FV-PTC cases. This finding might be important in a clinical setting and needs further validation.
Pietrowska et al. investigated molecular profiles of thyroid cancer subtypes using MALDI MSI and successfully classified medullary thyroid cancer and anaplastic thyroid cancer (23). However, the authors could neither discriminate nor classify three types of differentiated thyroid carcinomas, including FV-PTC and CV-PTC. One possible explanation for this discrepancy is the different spatial resolution used in our study (50 μm) and in the study by Pietrowska et al. (100 μm) (23). Taken together, the analytical power of MALDI MSI can be especially important for the successful discrimination and classification of tissue samples with similar molecular profiles.
The MALDI MSI approach was previously applied to the cytological smears of fine-needle aspiration (FNA) thyroid specimens, medullary thyroid carcinoma tissues, and a subset of thyroid carcinoma tissues originating from different thyroid cells (22,23,25,30). In addition, in a preliminary report by Pagni et al., minimal spectral differences between FV-PTC and CV-PTC were shown (22). In our study, ROC analysis revealed nine peptide signals that were in part able to distinguish between PTC variants and NIFTP specimens.
Interestingly, the peptides of three proteins (S100-A6, vimentin, and cytoplasmic actin 1) were detected with increased signal intensities in FV-PTC tissues. S100-A6 is a member of the S100 family of Ca2+-binding proteins and is known to affect cellular proliferation and cancer development (31). The overexpression of S100-A6 in PTC is well documented (32,33) and it has been suggested that S100-A6 plays an important role in PTC development (34). Previously, Sodiadis et al. used surface-enhanced laser desorption/ionization mass spectrometry and showed that S100-A6 was overexpressed in PTC when compared with normal tissue (35). Similarly, in a mass spectrometry approach, the S100-A6 protein was detected as a common protein associated with the papillary histotype (36). In our study, we detected two different peptides of S100-A6 in FV-PTC with high intensities; however, to make a general conclusion regarding its higher expression in FV-PTC compared with CV-PTC, there is a need for validation studies in an independent data set.
Vimentin belongs to type III intermediate filament proteins and is expressed in a broad range of cell types (37). A positive staining using a vimentin antibody was detected in many PTCs (38). Therefore, although vimentin is expressed in a wide range of PTC cells, the data suggest that it is more abundant in less aggressive PTCs. A marked alteration of actin cytoskeleton proteins is commonly observed in PTC (26,36), and in this study, we detected high intensities of two peptides of cytoplasmic actin 1 in FV-PTC.
Moreover, we found an increased signal intensity of prelamin A/C in CV-PTC tissues and an increased intensity of 60S ribosomal protein L6 and L8 in NIFTP tissues. Galli et al. evaluated specific protein signatures for malignant and benign thyroid specimens using MALDI MSI and found upregulated signals of cytoplasmic actin 1 and prelamin A/C in neoplastic thyroid tissues (25). The tissue microarray used in this study included FV-PTC and CV-PTC specimens; however, there was no information regarding the specific proteomic signature of the PTC variants. Although we observed increased peptide intensities for 60S ribosomal proteins L6 and L8 in NIFTP tissues, it still needs validation and a further examination in a comprehensive proteomic study on how NIFTP proteome profiles differ from FV-PTC (encapsulated and infiltrative) and CV-PTC.
In conclusion, MALDI MSI can create molecular profiles of specific regions by virtual microdissection and may present a tool that can be used to identify new molecular markers of thyroid pathology. This proteomic analysis of CV-PTC, NIFTP, and encapsulated FV-PTC revealed specific peptide signatures that can, in part, distinguish different histopathological variants of PTC. Specifically, clusters of peptides showed high discriminatory power for distinguishing CV-PTC from NIFTP and FV-PTC. The data presented here show that the NIFTP peptide profile is not much different from the encapsulated FV-PTC profile. Although limited in the sample size, infiltrative FV-PTC seems to have a different proteomic profile than NIFTP and encapsulated FV-PTC since the only infiltrative FV-PTC was clustered separately from NIFTP cases. We believe these findings could be a starting point for further investigations aimed at analyzing the whole proteomes of PTC variants and NIFTP lesions.
Footnotes
Acknowledgments
This study was supported by TUBITAK (Scientific and Technological Research Council of Turkey) 1001 grant, 214S012, and International Cost Project BM 1403 Native Mass Spectrometry and Related Methods for Structural Biology, 110664. In addition, this study was funded, in part, by Istanbul Development Agency (ISTKA).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7