
Abstract

Immune checkpoint inhibition, targeting the programmed death protein 1 receptor/programmed cell death 1 ligand 1 (PD-1/PD-L1) axis has been successfully implemented in cancer therapy. The anti-PD-1 monoclonal antibody nivolumab is approved for the treatment of several solid tumors, such as malignant melanoma, non-small cell lung cancer, and urogenital malignancies (1,2).
Reduction of immune tolerance by nivolumab leads to immune-related side effects including autoimmune events in various organ systems. In this context, involvement of the thyroid leads to thyroiditis, which is clinically associated with mostly asymptomatic dysfunction. In some cases, however, hypo- or hyperthyroidism, requiring hormone replacement or treatment of hyperfunction can occur (3,4). While this immune-related adverse event is well recognized following the evaluation of clinical trials (1,2), little is known about the histologic appearance of nivolumab-induced thyroiditis, which may be due to the noninvasive diagnostics and predominantly conservative treatment of nivolumab-induced thyroiditis.
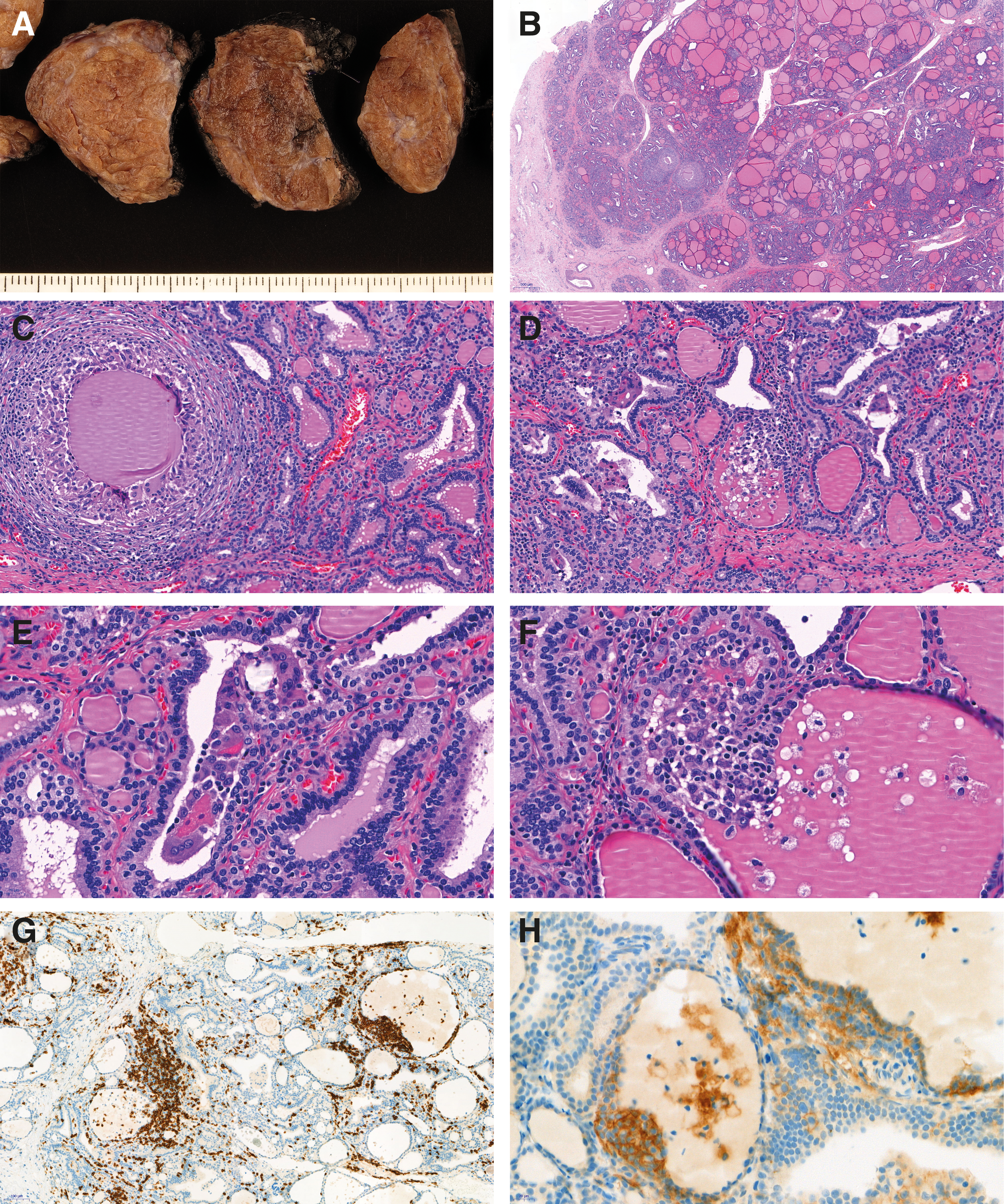
We report a case of a 44-year-old male who received biweekly nivolumab 3 mg/kg (200 mg) as a second line therapy of systemically metastasized non-small cell adenocarcinoma of the lung with good objective response. The patient developed TRAK-antibody-negative hyperthyroidism. Beta-blocker, glucocorticoid, and thyreostatic therapy was installed. Due to persisting hyperthyroidism and in order to enable resumption of the treatment with nivolumab, thyroidectomy was performed. Macroscopic evaluation of the thyroidectomy specimen revealed a slightly enlarged gland with accentuated lobulation (Fig. 1A). On histology, the thyroid showed chronic lymphocytic inflammation with formation of non-necrotizing colloid granulomas (Fig. 1B and C), and destruction of follicles with inflammatory infiltrates protruding into the lumen. Some scattered giant cells in areas of follicular destruction could be appreciated (Fig. 1D). In comparison with randomly selected cases of Graves' disease (n = 6), Hashimoto's thyroiditis (n = 5), and benign nodular goiter (n = 5), the inflammatory infiltrates in the autoimmune thyroid disorders were predominantly lympho-follicular, and formation of granulomas and destruction of follicles was seen only very rarely. These findings were nearly absent in nodular goiter. By immunohistochemistry, PD-L1 was expressed in epithelia and inflammatory cells in areas of follicular destruction of the thyroid after nivolumab treatment (Fig. 1E). Further characterization of the inflammatory infiltrate revealed a CD8+ predominant immune response in proximity to the granulomas (Fig. 1F), with only scattered FoxP3+ cells (not shown). This mixed PD-L1 positivity of epithelial cells and inflammatory cells and the predominance of CD8+ T cells within the inflammatory infiltrates were similar in the cases of Graves' disease or Hashimoto's thyroiditis and in contrast to examples of benign nodular goiter. Here, only very few CD8+ and PD-L1+ immune cells were detected, and only very few epithelial cells in close vicinity to PD-L1+ inflammatory cells showed PD-L1 positivity.
(
In summary, nivolumab-induced thyroiditis may histologically present as a granulomatous inflammation with active destruction of follicles, which is distinct from other types of autoimmune thyroiditis. Secondary overexpression of PD-L1 and predominance of the CD8+ T cell inflammatory infiltrates go well in line with an autoimmune reaction targeting follicular epithelial structures.