
Abstract
Background:
Current guidelines allow lobectomy as treatment for 1–4 cm papillary thyroid carcinomas (PTCs), as previous studies reported no clear survival advantages for total thyroidectomy (TT). However, data on recurrence based on surgical extent are limited.
Methods:
This study enrolled 2345 patients with 1–4 cm PTC. Those with lateral cervical lymph node metastasis or initial distant metastasis were excluded. Disease-free survival (DFS) was compared after 1:1 propensity score matching by age, sex, tumor size, extrathyroidal extension, multifocality, and cervical lymph node metastasis.
Results:
Lobectomy was performed in 383 (16.3%) and TT in 1962 (83.7%) patients. In the matched-pair analysis (381 patients in each group), no significant difference in DFS was observed during the median follow-up of 9.8 years (hazard ratio [HR] = 1.35 [confidence interval (CI) 0.40–1.36], p = 0.33). When stratified by tumor size, DFS did not differ between the group with 1–2 cm tumors and that with 2–4 cm tumors (HR = 1.57 [CI 0.75–3.25], p = 0.228; HR = 0.93 [CI 0.30–2.89], p = 0.902, respectively). Multivariate analysis showed that the surgical extent did not play an independent role in structural persistent/recurrent disease development (HR = 1.43 [CI 0.72–2.83], p = 0.306).
Conclusion:
Patients with 1–4 cm PTCs who underwent lobectomy exhibited DFS rates similar to those who underwent TT after controlling for major prognostic factors. This supports the feasibility of lobectomy as initial surgical approach for these patients and emphasizes that tumor size should not be an absolute indication for TT.
Introduction
C
No convincing prospective controlled trials have compared the disease-free survival (DFS) rates based on the surgical extent of patients with 1–4 cm DTCs. The 2015 ATA guidelines stated that the lowest recurrence rates were more likely associated with TT rather than with lobectomy. However, the studies supporting this finding included low-risk patients based on age, tumor grade, extent, and size (AGES), or age, metastasis, extent, and size (AMES) scoring systems (10,11), and therefore consisted of patients who would not be considered as low risk based on current standards. To fill this research gap, this study examined patients with tumor size ≥1 cm and <4 cm in order to identify any differences in DFS between patients who underwent lobectomy and those who underwent TT. By conducting a matched-pair analysis of major clinicopathologic factors, the aim was to determine whether the extent of surgery is associated with recurrence.
Methods
Study design and patients
This retrospective cohort study was conducted at a single tertiary institution, the Asan Medical Center in Korea, from 1998 to 2007. A total of 2345 patients with papillary thyroid carcinoma (PTC) with a tumor size of ≥1 cm but <4 cm were included. Patients who had lateral cervical lymph node (LN) metastasis (N1b) or distant metastasis (M1) at the time of initial treatment were excluded from this study. Of the 2345 patients, 383 (16.3%) underwent lobectomy, while the remaining 1962 (83.7%) underwent TT. The Institutional Review Board of Asan Medical Center approved the data collection and subsequent analyses.
Propensity score matching process
Using the propensity score matching method, patients who underwent lobectomy and TT were matched by age, sex, tumor size, ETE, multifocality, and cervical LN metastasis in a 1:1 ratio. Patients with similar propensity scores (those having the same probability of being assigned to the lobectomy group based on the aforementioned six covariates) were matched between the two groups, making the distribution of observed baseline covariates appear similar. Two patients in the lobectomy group were excluded after matching, as they had no matching propensity score with the patients in the TT group. In this manner, 381 patients were assigned to each group.
Surgical strategy
During the study period, the earlier ATA guidelines for DTC were adopted (12,13). Patients who refused TT were given sufficient information about the potential risks and benefits of thyroid lobectomy versus TT as well as follow-up examinations. At the Asan Medical Center, routine ipsilateral central compartment node dissection (CCND) was preferred, even in patients without clinically apparent LN metastases on preoperative staging. Bilateral CCND was performed if suspicious LN enlargement in the contralateral central compartment was observed on preoperative staging or during the operation and as treatment for bilateral cancer.
Management of follow-up after surgery
To maintain consistent follow-up for all patients, the following protocol was shared at the Asan Medical Center, as previously reported (14). Regardless of their surgical extent, all patients were regularly followed with physical examinations, thyroid function tests, serum thyroglobulin (Tg), and anti-Tg antibody measurements every 6–12 months for at least two years after surgery. Neck ultrasonography was performed within the first 6–12 months after the initial surgery and was routinely repeated at 12- to 24-month intervals. If indeterminate or suspicious thyroid nodules or LNs were found, fine-needle aspiration cytology (FNAC) was used for evaluation. Additional diagnostic imaging was performed to detect recurrence or distant metastasis in some patients, such as neck or chest computed tomography, magnetic resonance imaging, or whole-body fluorodeoxyglucose positron emission tomography.
Primary outcome
The primary outcome of this study was structural persistent/recurrent disease, defined as the appearance of metastatic lesions after initial treatment confirmed by cytological or histopathological examination, and/or the appearance of distant metastatic lesions on imaging studies. DFS, the interval from initial surgery to the detection of structural persistent/recurrent disease, was compared between groups formed according to the surgical extent.
Subgroup analysis
A subgroup analysis was performed according to the size of primary tumors: subgroup 1, tumor size ≥1 cm to <2 cm, and subgroup 2, ≥2 cm to <4 cm. In subgroup 1, 326 patients in the lobectomy group and their matched 326 patients in the TT group were evaluated. In subgroup 2, 55 patients were included in the lobectomy and TT group as a matched pair.
Statistical analysis
R v3.4.0 and the R libraries survival, car, and Cairo were used for data analysis (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline clinicopathologic characteristics according to surgical extent
Table 1 summarizes the baseline clinicopathologic characteristics of the 2345 patients with PTC according to their surgical extent. Before propensity score matching, the patients in the lobectomy group presented with significantly younger age, lower female sex proportion, smaller primary tumor size, lower rate of ETE, less multifocality, and less cervical LN metastasis than the patients in the TT group. However, in the matched cohort, no significant differences were found in baseline clinicopathologic characteristics between the two groups.
Categorical variables are presented as numbers with percentages and were analyzed by Pearson's chi-square test. Continuous variables are presented as median with IQR or mean with SD and were analyzed by Mann–Whitney's U-test or Student's t-test.
Y, yes; LN, lymph node; RAI, radioactive iodine; IQR, interquartile range; SD, standard devation.
In the subgroup analyses, patients with a tumor size of 1–2 cm also showed significant differences in age, sex, size, ETE, multifocality, and LN metastasis according to the surgical extent (Table 2). Likewise, patients with a tumor size of 2–4 cm showed a similar tendency, except for age and sex, which did not differ between the lobectomy and TT group. After propensity score matching, results showed that the clinicopathologic factors were balanced between the matched pairs.
Categorical variables are presented as numbers with percentages and were analyzed by Pearson's chi-square test. Continuous variables are presented as median with IQR or mean with SD and were analyzed by Mann–Whitney's U-test or Student's t-test.
DFS according to surgical extent
In a median follow-up of 9.8 years (IQR 5.1–12.2), 24 (6.3%) patients in the lobectomy group and 18 (4.7%) in the matched TT group developed structural persistent/recurrent disease (p = 0.427; Table 3). While most patients in the TT group presented with structural persistent/recurrent disease in the lateral cervical LN (83.3%; n = 15), 12.5% (n = 3) of those in the lobectomy group had structural persistent/recurrent disease in lateral cervical LN, 45.8% (n = 11) in the contralateral lobe, and 29.2% (n = 7) in both areas.
Figure 1A depicts the DFS curves of the two groups, showing no significant differences in DFS (hazard ratio [HR] = 1.35 [confidence interval (CI) 0.40–1.36], p = 0.33). Figure 1B and C shows the DFS curve of subgroup 1 (tumor size 1–2 cm) and subgroup 2 (tumor size 2–4 cm), respectively. In both subgroup analyses, the DFS did not differ according to the surgical extent (subgroup 1: HR = 1.57 [CI 0.75–3.25], p = 0.228; subgroup 2: HR = 0.93 [CI 0.30–2.89], p = 0.902).
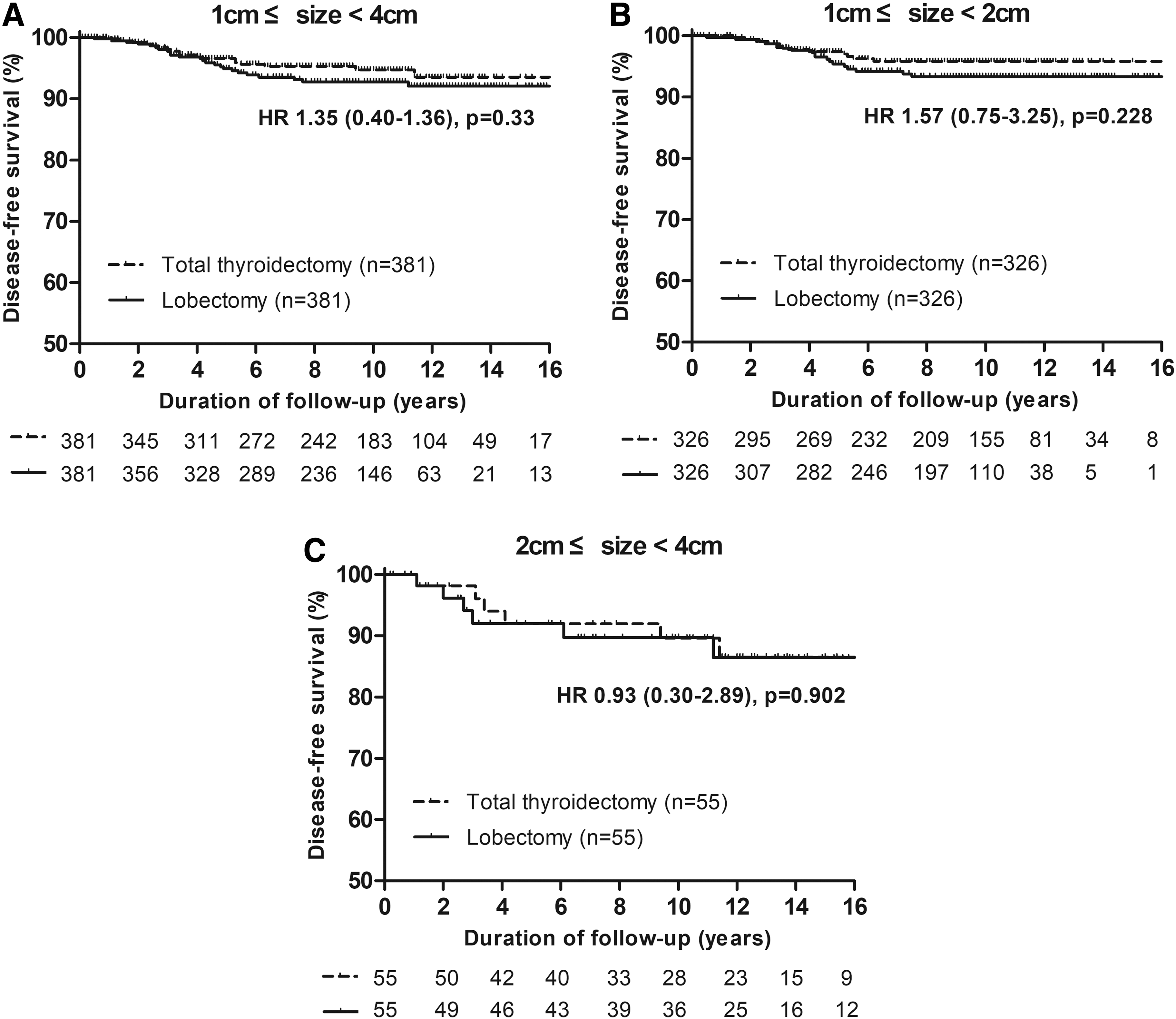
Disease-free survival curve of (
Impact of surgical extent on structural persistent/recurrent disease
Cox proportional hazard regression analysis of the variables associated with structural persistent/recurrent disease, including surgical extent, was performed (Table 4). In the univariate analysis, the tumor size, ETE, multifocality, and cervical LN metastasis significantly increased the risk of developing structural persistent/recurrent disease, whereas lobectomy did not (HR = 0.69 [CI 0.45–1.05], p = 0.86). Multivariate analysis also showed that lobectomy was not an independent risk factor for structural persistent/recurrent disease (HR = 1.33 [CI 0.84–2.10], p = 0.224). Moreover, a conditional Cox proportional hazard regression analysis performed in the matched cohort revealed that lobectomy was not associated with an increased risk of structural persistent/recurrent disease, even after stratification by matched pairs (HR = 1.43 [CI 0.72–2.83], p = 0.306).
HR, hazard ratio; CI, confidence interval.
Discussion
The optimal surgical approach for DTC, either lobectomy or TT, has been a topic of discussion for some considerable time. TT has certain advantages over lobectomy because it enables radioactive iodine (RAI) ablation after surgery and facilitates the use of Tg as a sensitive tumor marker for remnant thyroid tissue or recurrence during follow-up. However, as RAI ablation has been deferred in low-risk patients due to questions regarding its efficacy (15,16) and possible complications (17,18), lobectomy was used, as it requires less hormone replacement (19,20) and has a lower risk of complications compared to TT, including postoperative bleeding, hypoparathyroidism, and nerve injury (14,21,22). No definite advantages of clinical outcomes in either lobectomy or TT had been shown until Bilimoria et al. reported a survival benefit (98.4% vs. 97.1%, p < 0.05) and lower recurrence rates (7.7% vs. 9.8%, p < 0.05) in patients undergoing TT compared to those who underwent lobectomy (23). Hence, the 2009 ATA guidelines recommended that for patients with ≥1 cm and <4 cm tumors, TT should be the first-line treatment option in the absence of contraindications (2). However, the cited study lacked data on ETE, multifocality, comorbidity, and completeness of surgical resection. When Adam et al. took these factors into account and performed an updated analysis based on the same data source (National Cancer Data Base), the survival benefit was lost (3).
With emerging studies supporting the absence of clear survival advantages in patients undergoing TT compared to those undergoing lobectomy (4
–6,24), the 2015 ATA guidelines made some changes to the surgical treatment of DTC, allowing the performance of lobectomy in patients with a tumor size of ≥1 cm and <4 cm without ETE or any evidence of LN metastasis (1). The current retrospective matched-pair analysis of patients with PTC ≥1 cm and <4 cm supports this recommendation, as TT did not improve the 10-year DFS rate of 92.8% for lobectomy and 94.7% for TT. Moreover, after further stratification of the data, the lack of an advantage was still found when the patients were subdivided into those with 1–2 cm tumors and those with 2–4 cm tumors. Furthermore, conditional multivariate regression showed that the surgical extent had no significant impact on the risk of developing structural persistent/recurrent disease. These results will have a significant contribution to the improvement of current surgical approaches for thyroid cancer, as data regarding the differences in recurrence according to the surgical extent are limited (25). However, the results of this study are based on a matched-pair analysis of six clinicopathologic factors and are applicable to patients with similar clinicopathologic factors as the study patients. The baseline characteristics of patients who were excluded from this study after the propensity score matching are summarized in Supplementary Table S1 (Supplementary Data are available online at
Interestingly, the structural persistent/recurrent disease in the TT group was mostly due to the development of N1b disease (83.3%), while in the lobectomy group, 10 patients (41.7%) had lateral cervical LN metastasis (Table 3). The structural persistent/recurrent disease in the lobectomy group was more common in the contralateral lobe (75%). Since all the study patients underwent preoperative neck ultrasound (US) and indeterminate or suspicious thyroid nodules in the contralateral lobes were evaluated by FNAC prior to surgery, the recurrent nodules are expected to have developed after the initial surgery. This pattern of recurrence in patients who underwent lobectomy was more frequent than LN recurrences was also reported in previous reports (14,26). Whether this is due to more easily detectable suspicious nodules in the remaining thyroid lobe than LNs in the lateral neck by neck US, or whether remnant lobe recurrences occur earlier than in the lateral neck needs to be further investigated.
The strength of the current approach stems from the propensity score matched analyses for six major risk factors to minimize selection bias when deciding on the extent of surgery. The median follow-up duration was 9.8 years, which was relatively long compared to that in other studies. Moreover, subgroup analyses of patients with tumors measuring 1–2 cm and 2–4 cm provide additional clear evidence for the feasibility of lobectomy in PTCs measuring 2–4 cm. However, the study also has potential limitations. The impact of RAI remnant ablation on the clinical outcomes of the majority of patients who underwent TT could not be evaluated. Moreover, unilateral or bilateral prophylactic CCND was performed in patients who underwent lobectomy and TT, and a resulting effect on clinical outcomes cannot be excluded. However, pathological cervical LN metastasis was included as one of the propensity score matching variables in order to control for the impact of LN metastasis between the two groups. Also, since CCND was performed routinely at the Asan Medical Center, the influence of CCND on certain clinical outcomes such as central neck recurrence rates could not be evaluated. Usually, CCND is not routinely performed, and therefore this should be addressed by additional studies in order to determine whether there are differences in central neck recurrence rate according to surgical extent. Moreover, although propensity score matching for major risk factors was performed to minimize the selection bias, the possibility of potential selection bias cannot be eliminated, as this study was a retrospective study. Further prospective studies are necessary to validate the findings.
In conclusion, patients with 1–4 cm PTC who underwent lobectomy exhibited DFS rates similar to those who underwent TT after controlling for major prognostic factors. The surgical extent did not play an independent role in the development of structural persistent/recurrent disease in these patients. Although TT has the advantage that RAI scanning and Tg monitoring become more sensitive, the results emphasize that tumor size should not be an absolute indication for TT.
Footnotes
Author Disclosure Statement
The authors declare no potential conflict of interest.