
Abstract
Background:
The incidence of thyroid cancer has rapidly increased, and ecological evidence suggests this is due in some part to over-diagnosis. Understanding pathways to diagnosis could help determine whether unnecessary diagnosis can be avoided.
Methods:
A population-based sample (n = 1007) of thyroid cancer patients diagnosed between July 2013 and August 2016 was recruited from Queensland, Australia (response rate 67%). Information from structured telephone interviews was used to describe diagnostic pathways for thyroid cancer, to investigate factors associated with diagnostic pathways, and to assess the most prevalent modes of diagnoses by which the lowest-risk, potentially over-diagnosed thyroid cancers (intrathyroidal microcarcinomas) are detected.
Results:
Only 38% of participants presented with symptoms potentially related to thyroid cancer. Older age at diagnosis was associated with a lower prevalence of symptomatic diagnosis (prevalence ratio [PR] = 0.46 [confidence interval (CI) 0.31–0.68] for 70–79 vs. <30 years), as was frequent medical contact, while living in rural/regional areas was associated with a higher prevalence of symptomatic diagnosis (PR = 1.17 [CI 1.00–1.37] for rural/regional areas vs. major cities). Symptomatic diagnosis also occurred more for those whose tumors had adverse histopathological features (larger size, lymph node involvement, lymphovascular invasion). The likelihood of diagnosis of intrathyroidal microcarcinomas was greatest for those having surgical resection or monitoring for benign thyroid disease (PR = 3.87 [CI 2.81–5.32] and PR = 2.21 [CI 1.53–3.18], respectively).
Conclusions:
A minority of newly detected thyroid cancer cases were diagnosed because of symptoms. Access to medical care and factors related to cancer aggressiveness were associated with how diagnoses occurred. The likelihood of diagnosing the lowest-risk thyroid cancers was higher in situations related to management of other thyroid conditions. Adherence to thyroid management guidelines could reduce some thyroid cancer over-diagnosis, but ultimately better diagnostic tools are needed to differentiate between indolent cancers and those of clinical significance.
Introduction
The incidence of thyroid cancer has increased in many regions of the world over the past two to three decades (1 –6). Evidence suggests that this increase has been driven at least in part by greater ascertainment of asymptomatic tumors, which if undetected may have never caused symptoms or harm (7,8). It has been suggested that this increased ascertainment, also termed “over-diagnosis,” could be driven by incidental diagnosis resulting from increasing use of diagnostic imaging and more intensive scrutiny of histopathology specimens after thyroidectomy for benign conditions (9).
Although many reports have attributed the observed rise in incidence to increased detection of indolent subclinical lesions, few have investigated the situations in which people come to be diagnosed with thyroid cancer. Most studies that have investigated pathways to diagnosis of thyroid cancer were based on data from single-center tertiary-level institutes (10 –14) where patients may not be representative of all patients with thyroid cancer. The proportions of patients diagnosed with thyroid cancer without having experienced any relevant symptoms ranged from 10% (10) to 57% (11) in these studies. Population-based research from Australia (n = 452) (15) and the United States (n = 213) (16) found that 60–72% of thyroid cancer diagnoses occurred in patients without symptoms potentially related to thyroid cancer. Neither study addressed the circumstances in which very low-risk thyroid cancers (intrathyroidal microcarcinomas—those with the greatest potential to have been over-diagnosed) were detected.
Understanding more precisely the ways in which people come to be diagnosed and characteristics associated with different diagnostic pathways could help to determine whether unnecessary diagnosis can be avoided. Thus, a study was undertaken in Queensland, Australia, where the rise in diagnosis of thyroid cancer has been documented (6). Use of the state population-based cancer registry meant virtually complete ascertainment of thyroid cancer cases, and despite a universal health-care system, the state's large size and relatively high proportion of rural/regional residents means that access to health services varies considerably across the population. Information was used from a large sample of people newly diagnosed with thyroid cancer to describe their pathways to diagnosis and to investigate the socio-demographic and clinical factors associated with different modes of diagnosis. The study also examined how patients with the lowest-risk thyroid cancers came to be diagnosed in order to determine if such diagnoses could be minimized.
Methods
Study design and data collection
The Queensland Thyroid Cancer Study is a population-based case-control study established to investigate the pathways to diagnosis and the etiology of thyroid cancer. This analysis includes only the case participants. Eligible cases were residents of the Australian state of Queensland, aged 18–79 years, with thyroid cancer (excluding medullary cancers and lymphoma) newly diagnosed between July 2013 and August 2016.
Cases were ascertained through two sources: the Royal Brisbane and Women's Hospital (RBWH) and the Queensland Cancer Registry (QCR). Post-surgical thyroid cancer care is centralized in Queensland because the RBWH thyroid cancer clinic is the only institution in the state providing radioactive iodine (RAI) treatment. Thus, all patients diagnosed in Queensland who might require RAI attend the clinic, irrespective of where they live or whether they are public patients or privately insured. As a result, a substantial proportion of people diagnosed with thyroid cancer in Queensland are reviewed by the clinic either in person or by telephone. Potential participants were approached at their clinic appointment and invited to participate in the study. The study documents were mailed to those who agreed. To ensure that recruitment was as population based and complete as possible, eligible patients who were either not approached at their clinic appointment or not reviewed there (because they did not require RAI) were invited to participate via the population-based QCR using the registry's standard procedures. Cancer registration is a legal requirement in Australia, so the ascertainment of people diagnosed with thyroid cancer in Queensland during the study period was essentially complete. A QCR staff member first contacted each patient's doctor to obtain permission to approach patients, and once permission was obtained, a study information sheet, consent form, and reply-paid envelope were sent to the patients.
The study was approved by the Human Research Ethics Committee (HREC) of the QIMR Berghofer Medical Research Institute, as well as the HREC of the RBWH.
Of the 703 potential participants approached at the RBWH, 5% (n = 34) were ineligible on the basis of diagnosis date, age, inability to complete the questionnaire in English, or tumor type. Of the remaining 669, 89% (n = 595) met the study requirements. An additional 865 patients were identified through the QCR, and treating doctors gave consent for 766 (89%) to be approached about the study. Of these, 451 eligible patients agreed to take part, although 33 did not meet the study requirements, leaving 418 who were included. Overall, 1013 people with thyroid cancer participated in the study (American Association for Public Opinion Research response rate of 67%), and 1007 took part in the diagnostic pathways interview (see Supplementary Fig. S1).
How participants came to be diagnosed with thyroid cancer was ascertained using a structured telephone interview covering symptoms they may have had, medical practitioners consulted through the diagnostic process, and types of tests undertaken. Based on the interview data, each participant's mode of diagnosis was classified into two broad groups. First, a group classified as “symptomatic/patient initiated” were those who presented with symptoms potentially related to the thyroid (e.g., lump, voice change, swallowing problem, breathing difficulties, neck discomfort, and enlarged lymph nodes). Some of these symptoms may not have been related to thyroid cancer itself, but caused the patient to seek medical attention and then have the imaging or surgery that ultimately led to their thyroid cancer diagnosis. Second, a “medically initiated” group were those who were diagnosed as a consequence of consulting a medical practitioner for other reasons. These medically initiated circumstances were grouped as: (i) the doctor seeing or feeling a neck lump/mass while reviewing the patient for unrelated reasons; (ii) monitoring of known thyroid nodules or concern regarding a family history of thyroid cancer; (iii) work-up or follow-up for a diagnosis of benign autoimmune thyroid disease; (iv) surgical treatment for benign thyroid disease; and (v) unrelated imaging resulting in detection of a thyroid abnormality.
Socio-demographic information was recorded using a self-completed health and life-style questionnaire. The study classified participants' area of residence using their postcode and the Australian Statistical Geography Standard (ASGS) remoteness structure (17) into two categories: (i) those who lived in major cities and (ii) those who did not. Participants' permission was obtained to access relevant clinical records (histopathology, staging, and treatments), as well as information from the Medicare Benefits Schedule (MBS). All Australian permanent residents are eligible to receive subsidized health-care services (medical consultations, pathology testing, and medical imaging) through the MBS. MBS data were used to calculate the number of consultations (from both general practitioners and specialists) and imaging services that participants had received in the preceding 4.5 years. Tumor characteristics were extracted from the histopathology reports. The results of immunohistochemistry staining for the BRAFV600E mutation, undertaken using the BenchMark ULTRA platform (Ventana Medical Systems, Inc., Tucson, AZ), were available for most participants (n = 848; 84%). The scoring of these slides as positive or negative was performed by specialist endocrine pathologists.
To assess the situations in which the lowest-risk cancers were diagnosed, case participants were classified into two groups: those with the lowest-risk cancers (i.e., <10 mm in size, with no other concerning features—no lymph node involvement, no extrathyroidal extension or lymphovascular invasion, no distant metastases) and those with potentially higher-risk cancers (i.e., all other cases).
Statistical analysis
Simple proportions were used to describe the mode of diagnosis for the case sample. The distribution of participants' personal and tumor characteristics between the symptomatic and medically initiated diagnosis groups was compared to examine their associations with the diagnostic pathways. As a cross-sectional study design was used with a relatively common outcome (prevalence >10%), prevalence ratios (PR) were used as the measure of association, as in this setting it produces less biased estimates than odds ratios (18 –20). Hence, log-binomial regression models were used with the binary outcome of symptomatic versus medically initiated diagnosis to estimate the adjusted PR and confidence intervals (CI) for the associations between participant and tumor characteristics and their diagnostic pathways. Directed acyclic graphs were used to guide the selection of confounders to control for in the regression model (with separate sets of confounders selected to adjust for each characteristic). The same approach was used to identify the diagnostic scenarios whereby the clinically lowest-risk thyroid cancer cases were most likely to have been detected. Estimates presented in the tables are adjusted only for potential confounders.
Results
The majority (72%) of the included 1007 participants were female. The median age at diagnosis was 51 years (interquartile range [IQR] 41–61 years) for women and 56 years (IQR 47–67 years) for men. Most participants (88%) had papillary thyroid cancer. The median tumor size in women and men was 15 mm (IQR 8–28 mm) and 18 mm (IQR 9–35 mm), respectively. Participants and nonparticipants had similar distributions of sex and cancer subtype. However, those who took part in the study were slightly older (median 52 vs. 48 years) and had larger tumors (median 16 vs. 10 mm) than the nonparticipants.
Figure 1 shows the mode of diagnosis for the included participants. Overall, 38% (n = 381) of participants reported that they had abnormalities or discomfort related to their neck/throat, which led them to be diagnosed with thyroid cancer, and these people were classified as having had a symptomatic diagnosis. The majority (74% of 381) of these described having a neck lump as the main reason for initially consulting a doctor, and 15% presented initially with throat and neck discomfort and swallowing difficulties. The remaining 11% reported that cough, voice change, breathing difficulties, or symptoms of metastatic disease led to their diagnosis. Among the 626 (62%) participants who did not have symptoms (classified as having a medically initiated diagnosis), 89 (14%) had a neck lump noticed by their doctor; 79 (13%) were having a previously diagnosed thyroid nodule monitored or had a family history of thyroid cancer (n = 8); 80 (13%) were diagnosed through thyroid ultrasound performed as an investigation of hyper- or hypothyroidism; 139 (22%) were diagnosed incidentally via histopathology assessment after surgical resection of their thyroid for benign thyroid disease; and 239 (38%) had their thyroid cancer discovered through an imaging procedure (e.g., carotid artery ultrasound, computed tomography scan of head or neck, or positron emission tomography scan) performed for unrelated health problems.
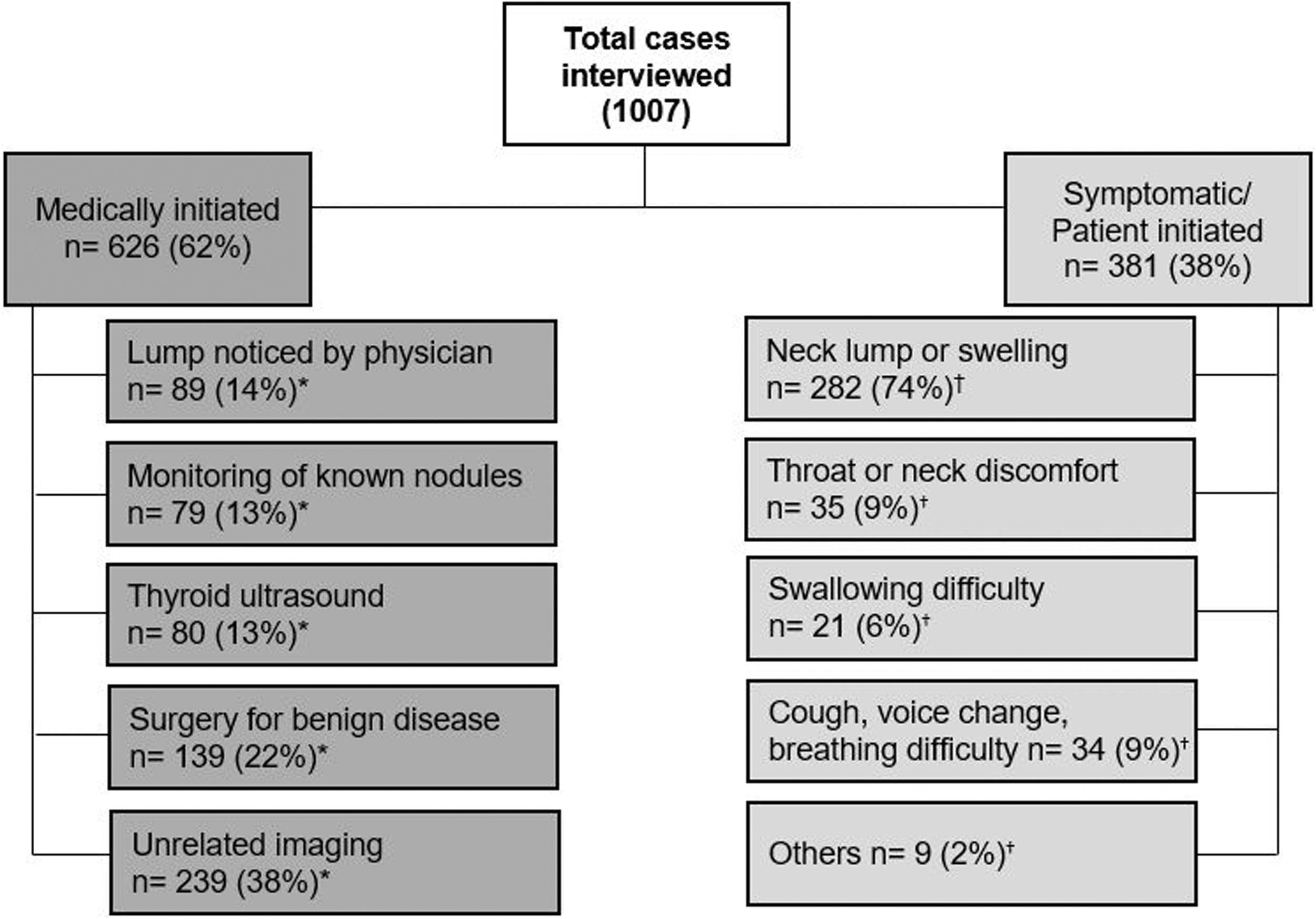
Mode of diagnosis of the study participants. *The percentage pertains to all those with a medically initiated diagnosis. †The percentage pertains to all those with a symptomatic/patient initiated diagnosis.
Table 1 shows the patient and tumor characteristics of those who presented with symptoms suggestive of thyroid cancer compared to those diagnosed through medically initiated pathways. The patient characteristics most strongly related to whether symptoms led to diagnosis were age and frequency of consultations with a doctor in the preceding 4.5 years. Beyond the age of 30 years, the likelihood of symptomatic diagnosis decreased by approximately 9% per decade, such that the proportion of those with symptomatic diagnosis was >50% lower among those in their 70s compared to those aged younger than 30 years (PR = 0.46 [CI 0.31–0.68]). The proportion being diagnosed because of symptoms was also almost 50% lower for those who consulted doctors on average more than eight times a year compared to those who visited doctors rarely (PR = 0.53 [CI 0.41–0.68] compared to fewer than two visits/year), even after consultations in the year prior to diagnosis were excluded. To assess how much of the association with age might be mediated by greater contact with medical practitioners, the model for age was adjusted by the participants' average frequency of consultation with medical practitioners. The association attenuated somewhat, particularly in the older (70–79 years) age group (PR = 0.57 [CI 0.38–0.85] compared to <30 years). When the average number of imaging procedures undertaken in the previous 4.5 years was also adjusted for, the association attenuated further (PR = 0.65 [CI 0.44–0.97] compared to <30 years). It was also found that living in rural or regional areas compared to major cities was associated with a slightly higher likelihood of symptomatic diagnosis (PR = 1.17 [CI 1.00–1.37]), but adjustment for the average frequency of consultation with medical practitioners did not change these estimates. Finally, a history of a benign thyroid condition was associated with a lower prevalence of symptomatic diagnosis.
Association Between Patient and Tumor Characteristics and Mode of Thyroid Cancer Diagnosis (Symptomatic or Medically Initiated)
1002 observations (symptomatic: 379; medically initiated: 623) were used in calculating prevalence ratios. The estimates were adjusted for confounders only (not potential mediators) as per the following: bage; csex; dage, sex, and area of residence; eage, sex, and education; fage and sex; gage, sex, history of thyroid disease, and area of residence; hage, sex, and subtype; iage, sex, tumor size, and lymphovascular invasion; jage, sex, and tumor size; kfor the estimation of association between BRAF mutation and mode of diagnosis, 848 observations (with definitive BRAF information) were used.
PR, prevalence ratio; CI, confidence interval.
The prevalence of symptomatic diagnosis was greater for those whose tumors had adverse prognostic characteristics, including larger tumor size, lymph node involvement, extrathyroidal extension, and lymphovascular invasion (Table 1), but the associations with both extrathyroidal extension and lymphovascular invasion weakened considerably after adjustment for tumor size and lymph node involvement (PR = 0.94 [CI 0.78–1.15] and PR = 1.18 [CI 0.98–1.41], respectively).
The prevalence of symptomatic diagnosis was >30% greater for follicular versus papillary thyroid cancers (Table 1), although this association was attenuated after adjusting for tumor size (PR = 1.09 [CI 0.97–1.23]), indicating that most of the association with subtype was due to the larger size, on average, of follicular cancers.
BRAF information was available (presence or absence of BRAF mutation) for 848 cases (451 [53%] positive; Table 1). BRAF mutations were observed more commonly in papillary cancers, as well as those with extrathyroidal extension, lymphovascular invasion, lymph node involvement, and advanced cancer stage. Among participants with papillary thyroid cancer, having a BRAFV600E mutation was associated with a higher prevalence of symptomatic diagnosis (PR = 1.26 [CI 1.04–1.52]). While this association attenuated when adjusted for lymph node involvement (PR = 1.12 [CI 0.92–1.36]), adjusting for size did not substantially alter the association.
Of the 1004 participants with full histopathological information, 230 (23%) had tumors that were <10 mm in size with no extrathyroidal extension, lymph node metastasis, or lymphovascular invasion. These cancers are considered to have very low risk of recurrence or metastatic disease compared to those with higher-risk features (21). All but one of these lowest-risk cancers were papillary carcinomas; 50% were suspected to be thyroid carcinomas prior to surgery. Results comparing the mode of diagnosis of these lowest-risk papillary thyroid microcarcinoma cases in the cohort to all other cases are presented in Table 2. Compared to those presenting with symptoms, the likelihood of diagnosis of the lowest-risk papillary microcarcinomas was substantially higher among those who had surgery for benign disease (PR = 3.87 [CI 2.81–5.32]), those diagnosed as a result of imaging as part of the management of benign autoimmune thyroid disease or a thyroid nodule (PR = 2.21 [CI 1.53–3.18]), and those diagnosed through unrelated imaging (PR = 1.51 [CI 1.04–2.18]; Table 2). Of note, almost half (n = 101; 44%) of those with the lowest-risk tumors had a fine-needle aspiration (FNA) biopsy prior to surgery, although it was not possible to determine how many had FNA of the actual microcarcinoma or whether they had an indeterminate FNA of a larger lesion resulting in the thyroid surgery, which ultimately detected an incidental microcarcinoma.
Association Between Mode of Diagnosis and Prevalence of Diagnosis of the Lowest-Risk Thyroid Cancers
1003 observations were used to calculate the prevalence ratios.
These cancers are of papillary subtype, <10 mm in size, and have no extrathyroidal extension, lymph node metastasis, or lymphovascular invasion.
Adjusted for age and sex.
Discussion
In a population-based cohort of individuals with newly diagnosed thyroid cancer, it was found that 38% presented to a physician with symptoms or other concerns related to their neck or thyroid. The remaining 62% had a medically initiated diagnosis, comprising 14% diagnosed by a physician noticing or palpating a lump and 48% diagnosed either in the course of management of benign thyroid conditions or unrelated health conditions. The proportion diagnosed symptomatically varied according to participant and tumor characteristics, such that older age at diagnosis, more frequent medical consultations, and having a history of benign thyroid disease were associated with a lower prevalence of symptomatic diagnosis, while those who lived in rural or regional areas had a higher prevalence of symptomatic diagnosis. With respect to tumor characteristics, follicular cancers, larger tumors, and those with evidence of local spread had a greater likelihood of being diagnosed because of symptoms. It was also observed that almost a quarter of all participants had cancers—predominantly of the papillary type—that would be classified as lowest risk. The proportion of these potentially “over-diagnosed” papillary microcarcinomas was higher among those diagnosed through surgery for benign thyroid disease or during imaging for other thyroid conditions (nodules or autoimmune disease).
Many studies have attributed the increase in thyroid cancer incidence to a greater ascertainment of subclinical lesions on the basis of a relative increase in the proportion of small cancers diagnosed (22 –25), but there has been little published work describing the pathways to diagnosis of thyroid cancer in the general population. The finding that 38% of patients had symptoms or concerns potentially related to thyroid cancer at the time of diagnosis is consistent with the 40% reported in another population-based study from Australia (15). A study from the United States (16) reported a lower proportion (28%), but they excluded those who presented with symptomatic thyroid masses that they considered unrelated to the thyroid cancer (16). The diagnostic interviews conducted in this study did not allow a distinction to be made between masses that were caused solely by thyroid cancer and those caused by underlying benign conditions such as (nodular) goiter. Hence, some patients probably reported neck symptoms/concerns that were not caused by their thyroid cancer. The previous Australian and U.S. studies both reported lower proportions diagnosed through unrelated imaging (18% and 26%, respectively, compared to 38% reported here) (15,16). This difference may reflect other studies' lower participation rate (44%) (15), and/or a smaller number of cases (15,16), or increases in imaging over time (time periods: 2006–2008 and 2000–2012) (15,16), or, for the U.S. study, differences in health-care services between countries.
The results indicate that factors associated with access to medical care were significantly related to the likelihood of a symptomatic diagnosis. Thus, in keeping with what might be expected under a scenario of over-diagnosis, having very frequent interactions with medical practitioners over the approximately four years prior to diagnosis was associated with a lower prevalence of symptomatic diagnosis. The proportion diagnosed because of symptoms was also lower in older people, and this effect was found to be partially mediated by their greater frequency of medical consultations and greater frequency of various types of diagnostic imaging. Additionally, the prevalence of symptomatic diagnosis was higher among residents of rural and regional areas, who may have less access to a range of specialist health services than those who live in major cities.
Consistent with the literature (12,15), the current analyses also suggest that features related to cancer stage were significantly associated with how people came to be diagnosed. Thus, larger tumors and tumors with adverse pathological features such as lymph node involvement and extrathyroidal extension were more likely to be diagnosed because of symptoms than the smaller, lower-risk cancers. Follicular cancers were also more likely to present with symptoms, an effect that was due mostly to the larger tumors in this subtype. Cancers with BRAF mutations were also more likely to be diagnosed due to symptoms or patient concerns. This association was essentially driven by the fact that cancers with a BRAF mutation were more likely to have high-risk features such as lymph node involvement, which is in keeping with the literature (26 –28).
It was also found that the diagnostic situations associated with the highest prevalence of low-risk papillary microcarcinomas were when ultrasound was used as part of the diagnosis/management of hypo- or hyperthyroidism, or for monitoring of thyroid nodules, as a result of pathological assessment of thyroid glands after surgery for benign disease, and through unrelated imaging. These results imply that complete prevention of diagnosis of these lowest-risk cancers is probably not possible. However, there are some ways in which the frequency of diagnosis of these potentially over-diagnosed cancers may be minimized. For example, national endocrinology organizations (e.g., The Endocrine Society of Australia and the United States, and the Canadian Society of Endocrinology and Metabolism) recommend that thyroid ultrasound should not be routinely ordered in people with abnormal thyroid function unless they have a palpable thyroid abnormality (29 –31). In the present cohort, 80 (8%) people reported that they had a thyroid ultrasound because of abnormal thyroid function tests. While it is not possible to be sure that these people did not also have a palpable abnormality, it is likely that at least a small proportion of thyroid cancer diagnoses could be avoided if this recommendation was followed. The American Thyroid Association guidelines for managing thyroid nodules and differentiated thyroid cancer (21) also recommend that FNA should not be undertaken on nodules <1 cm. In this study, almost half of those with the lowest-risk cancers had a FNA prior to surgery. Data are not available on why these procedures were done, but ensuring that clinicians are aware of these recommendations may help reduce over-diagnosis of these mostly indolent cancers.
The analysis also found that a high proportion of the lowest-risk cancers were diagnosed because of surgery for benign thyroid disease. Although it may not be possible to avoid these surgeries, it is likely that the number of lesions designated as cancer following these procedures will decrease due to the recent reclassification of the indolent “noninvasive form of encapsulated follicular variant of papillary thyroid cancers” as “noninvasive follicular thyroid neoplasm with papillary-like nuclear features” (32,33). The changed terminology, eliminating “cancer,” is likely to reduce psychological burden to the patients and clinical consequences such as total thyroidectomy and RAI treatment (33).
Post-diagnosis management is important to avoid unnecessary treatment of the lowest-risk cancers. For these cancers, active surveillance may be an acceptable alternative to immediate surgery (34 –38). Several studies involving patients with low-risk differentiated carcinomas have shown that tumor growth tends to be very slow, especially in older patients (those aged >60 years), and only a small number of tumors progressed to clinically significant disease during the follow-up period (range 1–17 years), all of which were readily treatable (34,36,37).
One limitation of this study is that a telephone interview was used to ask the participants about how they came to be diagnosed. Thus, recall error may have caused some cases to be misclassified. However, the interviews were conducted on average within five months of the date of diagnosis by an experienced research nurse using a structured interview form to ensure information was consistently collected. Hence, misclassification of the pathways to diagnosis is likely minimal. Furthermore, such misclassification is unlikely to be differential. Other methods of collecting diagnostic information such as medical chart review or using administrative claims data were considered. However, these methods also have limitations. Neither is designed for research purposes, so much of the information required to answer specific research questions may not have been adequately recorded. Claims data include no information on symptoms, while inaccuracies in documenting and abstracting information from medical records can also lead to error. Additionally, obtaining the information from primary-care records where most of these patients would have been originally diagnosed would not be practical. Another potential limitation is that almost 30% of eligible people did not participate. Those who took part were on average a little older and tended to have somewhat larger tumors compared to the eligible nonparticipants. They were also somewhat more likely to have been assessed for the need for RAI treatment at the RBWH. It is therefore likely that the sample included a higher proportion of patients with tumors with higher-risk features. Thus, had all eligible patients participated, the proportion with a medically initiated diagnosis may have been higher than reported, and the association between age and mode of diagnosis may have been somewhat attenuated.
In conclusion, the present findings suggest that the majority of people newly diagnosed with thyroid cancer did not present with symptoms suggestive of thyroid cancer. Access to medical care and factors related to cancer aggressiveness were associated with how people came to be diagnosed. The likelihood of diagnosing the lowest-risk papillary microcarcinomas was highest in circumstances related to management of benign thyroid disease, and much of this is probably unavoidable. Nevertheless, appropriate adherence to existing thyroid nodule management guidelines and pathological reclassification of indolent neoplasms could go some way to reducing thyroid cancer over-diagnosis. Ultimately, better diagnostic tools are needed, potentially including molecular markers, to differentiate between indolent/lowest-risk cancers and those of greater clinical significance. Until such technology is available, it is likely that diagnosis of indolent thyroid cancers will continue to contribute significantly to the incidence of thyroid cancer.
Footnotes
Acknowledgments
This study was supported by a grant from the National Health and Medical Research Council (NHMRC APP1047733) of Australia. S.J. and R.N. were supported by fellowships from the NHMRC (APPs 1061341 and 1060183, respectively). S.R. is supported by a scholarship from the QIMR Berghofer Medical Research Institute. We would like to acknowledge the work of Andrea McMurtrie, RN, and Emily Dickson, BA, for undertaking the data collection. We would also like to acknowledge the Royal Brisbane and Women's Hospital's assistance with participant recruitment and Sullivan Nicolaides Pathology for their assistance with the BRAF mutation data.
Author Disclosure Statement
All of the authors declare no support from any organization for the submitted work, no financial relationships with any organizations that might have an interest in the submitted work, and no other relationships or activities that could appear to have influenced the submitted work.
Supplementary Material
Supplementary Figure S1