
Abstract
Background:
Publication of the 2015 American Thyroid Association (ATA) management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer was met with disagreement by the extended nuclear medicine community with regard to some of the recommendations related to the diagnostic and therapeutic use of radioiodine (131I). Because of these concerns, the European Association of Nuclear Medicine and the Society of Nuclear Medicine and Molecular Imaging declined to endorse the ATA guidelines. As a result of these differences in opinion, patients and clinicians risk receiving conflicting advice with regard to several key thyroid cancer management issues.
Summary:
To address some of the differences in opinion and controversies associated with the therapeutic uses of 131I in differentiated thyroid cancer constructively, the ATA, the European Association of Nuclear Medicine, the Society of Nuclear Medicine and Molecular Imaging, and the European Thyroid Association each sent senior leadership and subject-matter experts to a two-day interactive meeting. The goals of this first meeting were to (i) formalize the dialogue and activities between the four societies; (ii) discuss indications for 131I adjuvant treatment; (iii) define the optimal prescribed activity of 131I for adjuvant treatment; and (iv) clarify the definition and classification of 131I-refractory thyroid cancer.
Conclusion:
By fostering an open, productive, and evidence-based discussion, the Martinique meeting restored trust, confidence, and a sense of collegiality between individuals and organizations that are committed to optimal thyroid disease management. The result of this first meeting is a set of nine principles (The Martinique Principles) that (i) describe a commitment to proactive, purposeful, and inclusive interdisciplinary cooperation; (ii) define the goals of 131I therapy as remnant ablation, adjuvant treatment, or treatment of known disease; (iii) describe the importance of evaluating postoperative disease status and multiple other factors beyond clinicopathologic staging in 131I therapy decision making; (iv) recognize that the optimal administered activity of 131I adjuvant treatment cannot be definitely determined from the published literature; and (v) acknowledge that current definitions of 131I-refractory disease are suboptimal and do not represent definitive criteria to mandate whether 131I therapy should be recommended.
Introduction
When developing guidelines, it is to be expected that areas of controversy will arise, especially if there are proposals for concepts that may significantly impact clinical practice. Soon after release of the 2015 American Thyroid Association (ATA) management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer (DTC) (1), it became evident that strong differences of opinion existed involving some of the guideline recommendations. Specifically, nuclear medicine specialists voiced several concerns about some of the recommendations related to the diagnostic and therapeutic utilization of radioiodine (131I). There was enough disagreement with the content of the ATA guidelines that both the European Association of Nuclear Medicine (EANM) (2) and the Society of Nuclear Medicine and Molecular Imaging (SNMMI) declined to endorse the guidelines.
In the summer of 2016, Dr. Ciprian Draganescu, Head of Nuclear Medicine Department of the University Hospital of Martinique, with his colleague Dr. Patrick Bourguet, contacted various individuals of the ATA, EANM, SNMMI, and the European Thyroid Association (ETA) to explore hosting a meeting to discuss some of the aforementioned differences in opinion constructively. The four organizations worked together to define the format and scope of the meeting and to agree on the selection of an impartial meeting moderator. Four major topic areas for discussion at the first joint meeting were identified: (i) formalizing the dialogue and activities between the four societies, (ii) indications for 131I adjuvant treatment, (iii) defining the optimal prescribed activity of 131I for adjuvant treatment, and (iv) clarifying the definition and classification of 131I-refractory thyroid cancer.
The ATA, EANM, SNMMI, and ETA each sent senior leadership (including the Presidents of the EANM and SNMMI, the President Elect of the ETA, the Secretary/Chief Operating Officer of the ATA) and subject-matter experts to a two-day interactive meeting in Martinique (January 13–14, 2018). Eight countries were represented, including Belgium, Denmark, France, Germany, the United Kingdom, Switzerland, The Netherlands, and the United States. Dr. Laszlo Hegedüs, President-Elect of the ETA, was unanimously selected by the four organizations to be the meeting moderator. The local organizing committee provided funding for onsite meeting expenses, while the four organizations supported travel expenses for their representatives.
After much consideration, debate, and collegial exchange of concepts, the conference participants agreed on a set of nine principles (Fig. 1). These principles, along with this article, describe the group's deliberations and suggestions for future research.
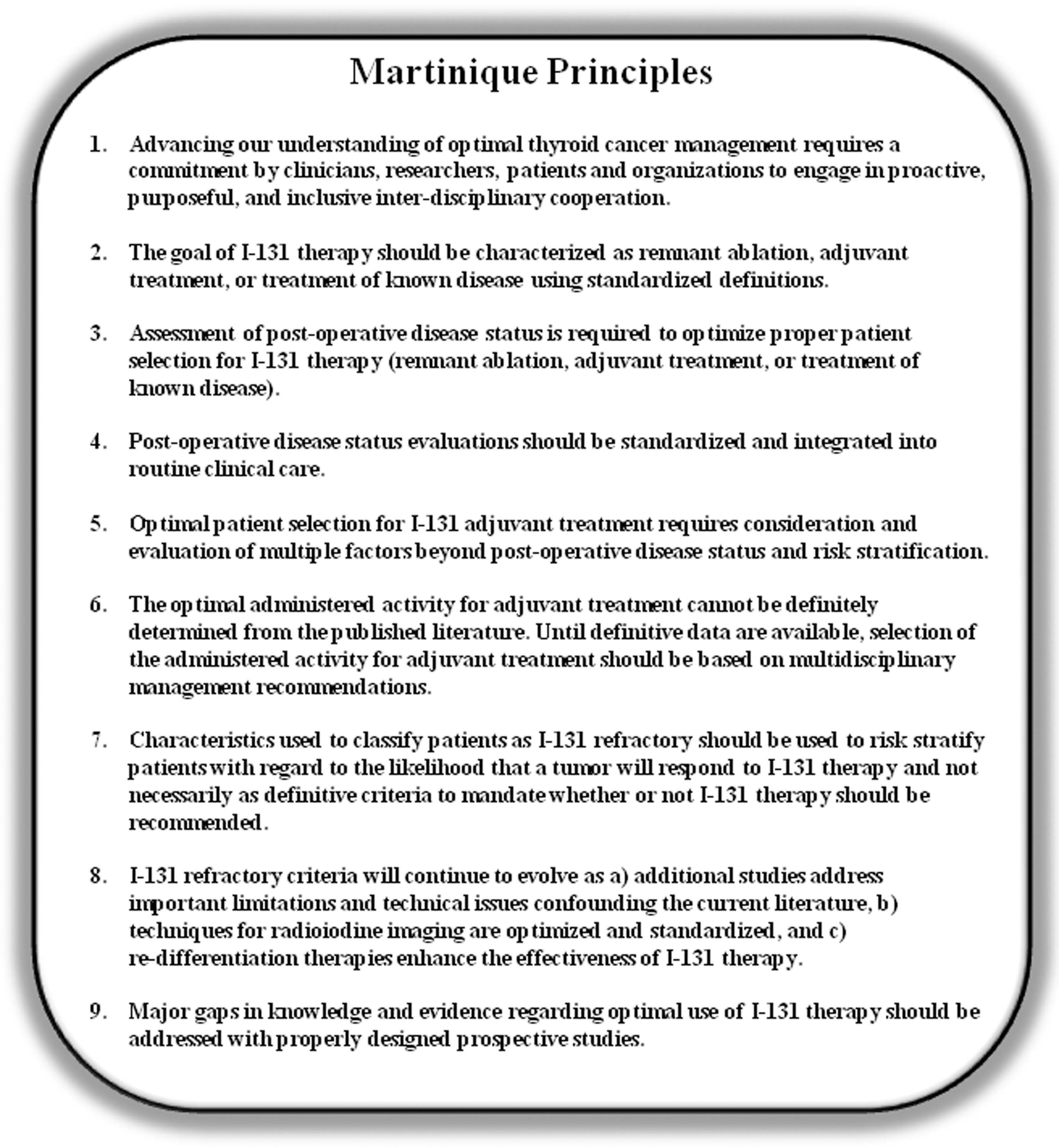
Nine principles that summarize the major points of discussion during the first Martinique meeting in January 2018.
After the Martinique meeting, constructive interactions among the societies continue, which include making plans for future meetings, identifying specific ways that the societies could most productively interact on topics of mutual interest, and exploring the best way to foster meaningful involvement of patients and patient organizations.
Acceptance of precise and well-defined terminology to describe the goals of the first administered activity of 131I after thyroidectomy for DTC will improve care by facilitating communication, discussion, and interpretation of the literature. As a prominent example, the non-descript colloquial use of the word “ablation” to describe all therapeutic goals of 131I after total thyroidectomy has thus far hindered a constructive scientific dialogue.
It has generally been recognized that the first administered activity of 131I after thyroidectomy can be used in attempts to destroy (i) residual presumably benign thyroid tissue, (ii) suspected but not identified remaining disease, and/or (iii) known residual or recurrent disease (1,3). Yet, a precise nomenclature to describe these three important goals has not been widely accepted. We propose adoption of a nomenclature that uses “131I therapy” as the broad term that encompasses the three primary goals associated with an administered activity of 131I: (i) remnant ablation, (ii) adjuvant treatment, or (iii) treatment of known disease (Fig. 2) (4). While listed as separate therapeutic goals, it is recognized that 131I used for remnant ablation may have a tumoricidal effect and that 131I used for adjuvant treatment may also destroy normal remnant thyroid.
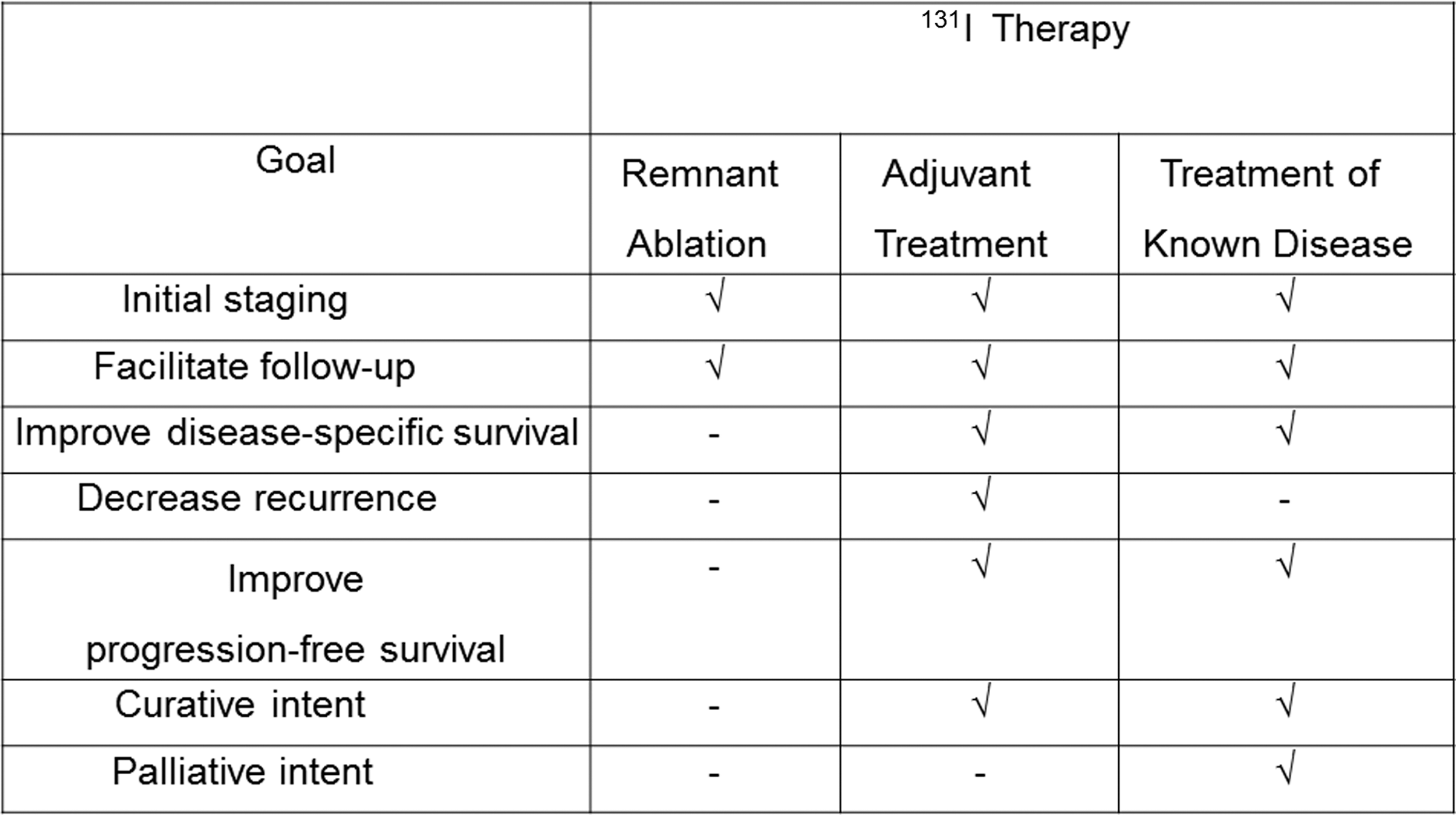
Terminology that should be used to communicate the goals of 131I therapy.
Remnant ablation refers to the use of 131I to destroy postoperatively residual presumably benign thyroid tissue to facilitate initial staging and follow-up studies (such as serum thyroglobulin [Tg] and radioactive iodine imaging).
Adjuvant treatment is an “additional cancer treatment given after the primary treatment to lower the risk that the cancer will come back” (5). Within the context of the therapeutic use of 131I for thyroid cancer, adjuvant 131I treatment can thus be defined as 131I administered in an effort to destroy subclinical tumor deposits that may or may not be present after surgical resection of all known primary tumor tissue and metastatic foci.
The goals of adjuvant treatment are to improve disease-specific survival, decrease recurrence rates, as well as to improve progression-free survival. It is important to remember that since adjuvant treatment is given for a risk rather than for known disease, it is accepted that some patients who receive adjuvant treatment might already have been treated sufficiently by their primary surgery. Therefore, selection for adjuvant treatment involves both an assessment of risk of DTC recurrence/persistence and risk of dying of DTC, as well as the prediction of the likelihood that 131I treatment may have a meaningful impact on an individual patient's course of disease.
Treatment of known biochemical or structural disease refers to the goal of destroying persistent or recurrent DTC foci with 131I in order to improve progression-free, disease-specific, and overall survival. It can be given with either curative or palliative intent.
Even though most guidelines make recommendations with regard to the postoperative use of 131I based primarily on staging systems that predict risk of recurrence or disease-specific mortality, the actual goal of 131I therapy can only be determined once the postoperative disease status has been assessed (1). Regardless of initial risk stratification, patients with biochemical, structural, or functional evidence of persistent disease can only be candidates for “treatment of known disease.” Patients demonstrating no histological, biochemical, or imaging evidence of persistent disease after appropriate initial surgery may be candidates for observation, remnant ablation, or adjuvant treatment.
For DTC, the most common postoperative tools used to refine clinico-histological staging assessments include serum Tg measurement, neck ultrasonography (US), and diagnostic radioactive iodine scanning (1). Neck US is operator dependent, and although the sensitivity for detection of cervical nodal metastases is high, except in the central compartment prior to thyroidectomy, its specificity is suboptimal (6 –8). Tg measurements are performed using a multitude of assays providing different results, are influenced by concurrent thyrotropin (TSH) levels, and are prone to interference by Tg autoantibodies (9 –12). Furthermore, the precise Tg value, either basal or TSH stimulated, that should be used to distinguish adjuvant treatment from treatment of known disease has not been firmly established (1). Radioactive iodine scanning is performed with different iodine isotopes (123I, 124I, and 131I) and acquisition modalities (planar vs. single-photon emission computed tomography [SPECT] vs. SPECT/computed tomography [CT] vs. positron emission tomography/CT) with varying sensitivity and specificity (13,14). Despite these limitations, diagnostic radioactive iodine imaging has been shown to contribute to staging and risk stratification, especially by detection of unsuspected lymph node and distant metastases (15 –18).
From a clinical application perspective, it is important to emphasize that the vast majority of the available retrospective data pertain primarily to papillary thyroid cancer (and its variants). Therefore, generalizing these recommendations to other subtypes of DTC (such as follicular thyroid cancer, Hürthle cell thyroid cancer, or poorly differentiated thyroid cancer) may or may not be appropriate. Thus, while there is uniform agreement with regard to the importance of evaluating postoperative disease status, no one has established reliable, universally accepted, precise recommendations to guide the proper assessment of postoperative disease status. Until precise guidelines are developed and accepted, multidisciplinary teams should establish local standards to guide clinical management.
While most studies examining the potential benefit for 131I therapy in the postoperative disease setting did not define the disease status in a consistent manner, a number of retrospective studies comparing patients with and without 131I are nonetheless available in the literature. As summarized in a meta-analysis by Sawka et al. in 2008 (19) and confirmed in the literature of the past decade, the findings are inconsistent. Some authors report a benefit of giving 131I even to patients with non-metastasized microcarcinomas (20,21), whereas other groups find no benefit (19,22,23). There is a tendency for larger cohorts and longer follow-up durations to be loosely associated with improved outcomes following 131I therapy—but these findings are not consistent across the available reports (24 –27). Although all authors are studying the same disease and the same therapeutic modality, the variability of the findings indicate that large and important sources of heterogeneity exist in patient selection and therapeutic effectiveness.
In DTC, there most likely is not one “right” way of treating patients. While traditional factors such as postoperative risk assessment, the estimated likelihood that administration of 131I will significantly improve the clinical outcomes of interest (recurrence, disease-specific mortality), assessment of potential side effect profile, and patients preferences and values are critical to decision making, other important elements such as the availability and quality of US, radioactive iodine imaging, Tg assays, experienced thyroid surgeons, and preferences of the local disease management team are additional key elements that must be considered when deciding whether an individual patient could benefit from 131I adjuvant treatment (see Fig. 3). Most of these factors have likely not been adequately considered in the numerous published retrospective studies. In this respect, the ATA guidelines specifically note that “local factors such as the quality of pre-operative and postoperative US evaluations, availability and quality of Tg measurements, experience of operating surgeon, and clinical concerns of the local disease management team may also be considerations in postoperative 131I decision making” (1).
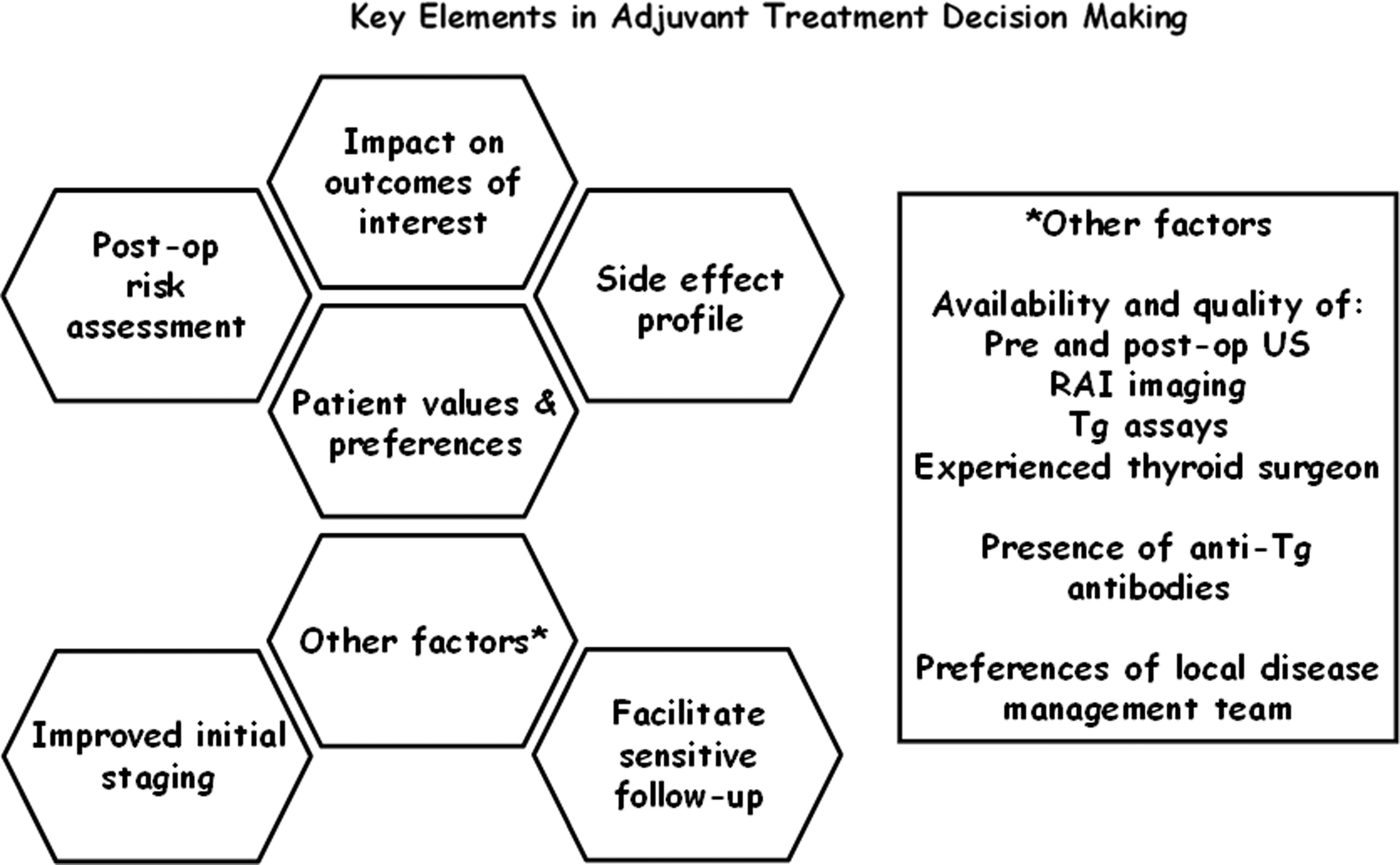
General groups of “key elements” that should be considered when evaluating a patient for possible adjuvant 131I therapy.
Furthermore, discussing, understanding, and integrating patient values and preferences into the shared decision-making process is important, especially when so little high-quality prospective evidence is available either for or against the postoperative use of 131I (28). In many patients, especially those receiving appropriate care up to the point of decision on 131I, both performing and not performing 131I therapy can be justified based on the available literature (1). Often, the final decision on whether to give 131I is influenced by patients' wishes, objections, hopes, and fears. Here, it is the obligation of the attending physician to give the most objective assessment possible and to discuss the pros and cons of 131I in relation to the individual patients' situation within a particular health-care environment.
Ideally, the administered activity selected for adjuvant 131I treatment needs to balance treatment efficacy with unwanted side effects. It is assumed that higher administered activities of 131I will on average lead to greater therapeutic efficacy by delivering higher absorbed doses to target lesions (29 –33). At the same time, the absorbed dose to non-target tissue such as the salivary glands will also be greater with increasing administered activities, thus potentially leading to a higher incidence of adverse effects such as a sialadenitis (34). This is particularly important when considering adjuvant treatment where some patients will by definition not have residual disease, whereas others may subsequently be proven to have distant metastatic disease on the post-therapy scan.
Assessing the role of adjuvant treatment by a review of the literature is difficult, as most studies have examined relatively small cohorts followed for suboptimal time periods. Furthermore, the low event rates in patients selected for adjuvant therapy can make it difficult to identify a clinical benefit (23). Retrospective studies that are underpowered to detect small event rates over long time periods may lead to the unjustified conclusion that 131I adjuvant treatment has no beneficial effect. Well-designed, prospective, randomized clinical trials that are powered to address these important clinical endpoints are required to determine for definite whether 131I adjuvant treatment has a beneficial effect in properly selected patients.
Although the candidates for adjuvant treatment differ from patients being treated for known residual disease, a look at the latter population may be instructive. Larger cohort retrospective studies with long-term clinical follow-up (>10 years) provide some evidence regarding the therapeutic 131I effectiveness for decreasing thyroid cancer mortality (25) and recurrence rates (24 –26). A meta-analysis of 31 patient-cohort studies regarding the effectiveness of 131I therapeutic administration demonstrated a statistically significant effect on improving clinical outcomes at 10 years, with a decreased risk for locoregional recurrence (relative risk = 0.31 [confidence interval (CI) 0.20–0.49]) and an absolute risk reduction of 3% [CI 1–4%] for distant metastatic disease (27). The beneficial effect of 131I adjuvant treatment in patients who truly have residual thyroid cancer that is unknown prior to 131I administration is most easily demonstrated in higher-risk patients (35,36) and may be related to higher administered activities (37). However, in lower-risk patients, three systematic reviews examining the results of multivariate adjusted analyses did not demonstrate a significant effect of 131I adjuvant treatment on disease-related mortality and showed conflicting results with regard to disease recurrence (19,22,23). In these lower-risk patients, the issue may not be the effectiveness or ineffectiveness of 131I in treating residual disease, but rather the relatively small number of lower-risk patients who truly have residual disease.
Until the results of prospective multicenter studies centering on relevant outcomes of adjuvant postoperative 131I treatment, including disease-specific survival and disease-free survival as well as the incidence of side effects, are available, the activity to be prescribed for adjuvant treatment of DTC remains a question best answered on an individual basis in a multidisciplinary setting.
Several groups have proposed various definitions, classifications, and criteria to identify patients with 131I-refractory thyroid cancer (1,38 –45). However, instead of using any of the prior terms that have specific connotations, the term “clinical scenarios” will be used to describe and discuss five common findings that increase the likelihood that a patient has 131I-refractory thyroid cancer in the setting of persistent/recurrent biochemical or structural evidence of disease (Table 1).
Common Clinical Scenarios that Suggest a Patient May Have 131I-Refractory Thyroid Cancer
It is important to note that no current definition, classification, criterion, or clinical scenario is an absolute indicator that a patient has 131I-refractory DTC. Simply because a patient fits a particular clinical scenario does not mean that this patient's DTC should be absolutely defined or labeled as 131I refractory, but rather conveys the likelihood that a tumor will be refractory to additional 131I therapy. Each patient should be managed individually with a thorough understanding of the many factors that enter into the appraisal of the likelihood that a tumor will be refractory to 131I, as well as weighing the patient's specific clinical scenario and the risks and benefits of 131I therapy. It is not the specific objective of this section to present a consensus statement or to discuss all aspects for and against a particular clinical scenario indicating 131I-refractory disease. Rather, the specific objectives are to encourage the practicing physician to (i) be cautious in labeling a patient as 131I refractory, (ii) have a better understanding of the complexity of such a decision, and (iii) encourage further dialogue and research on this topic.
Clinical Scenario 1: No radioiodine uptake is present on a diagnostic radioiodine scan.
A negative diagnostic scan increases the likelihood that the patient's DTC is 131I refractory, but it is not an absolute criterion. Conversely, the presence of radioactive iodine uptake on a diagnostic radioactive iodine scan is not a certain marker of 131I responsiveness. There are many confounding factors. First, preparation, including avoidance of iodine excess and adequate TSH stimulation—details of which are a topic of discussion in itself—is important. Second, the technique of radioactive iodine scanning is critical and varies significantly between different centers (46). High-resolution imaging incorporating SPECT/CT provides much more functional and anatomic detail than planar imaging (Fig. 4) (15). A lack of optimization and standardization of radioactive iodine scans can lead to suboptimal imaging that may inappropriately classify a patient as having 131I-refractory disease. Although the phrase “appropriately performed radioactive iodine imaging” is often used as part of the definition of 131I-refractory disease, this really evades what is “appropriately performed radioactive iodine imaging” and whether one knows that the patient has undergone radioactive iodine imaging that maximizes identification of functioning DTC foci.
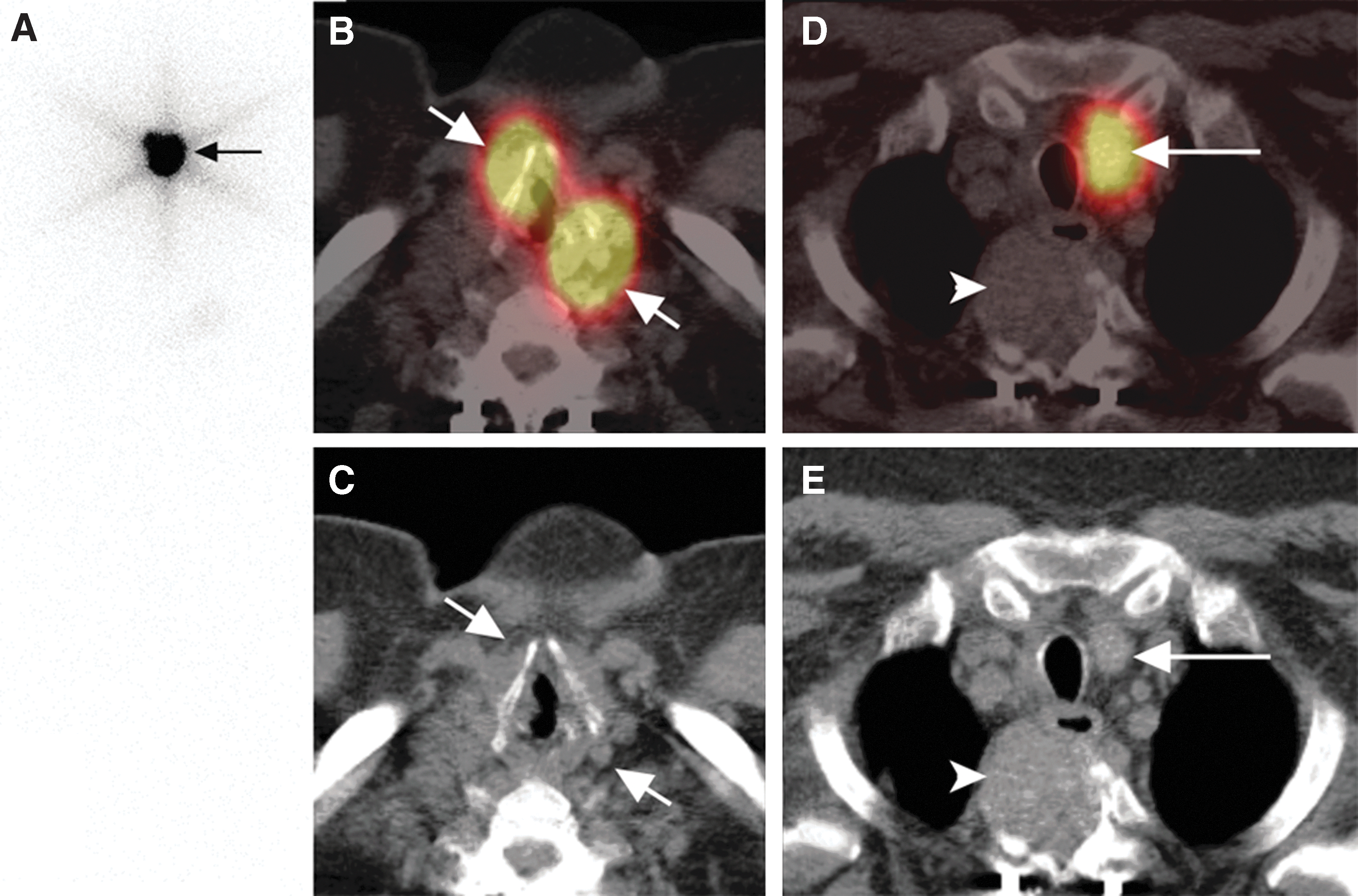
Pre-ablation 131I single-photon emission computed tomography (SPECT)/computed tomography (CT) imaging in a 65-year-old man with a multifocal 7 cm tall-cell variant papillary thyroid cancer, with capsular and vascular invasion, extrathyroidal extension, and positive surgical margins; 0/2 central neck nodes dissected; thyroglobulin was 1136 ng/mL (thyrotropin 4.5 mIU/L). Stage: as pT4A N0 M0, Stage 4A, classified as high risk. Planar anterior whole-body images (
Finally, it is well documented in the literature that a diagnostic radioactive iodine scan is frequently negative, but the post-131I therapy scan is positive for functioning 131I-avid metastases (47 –53). Although this scenario may be associated with an increased likelihood that the patient has 131I-refractory DTC, it does indicate that the tumor retains 131I avidity and may be 131I responsive.
Clinical Scenario 2: No radioiodine uptake is present on a radioiodine scan performed several days after 131I therapy.
This clinical scenario portends one of the highest likelihoods that the patient's DTC is 131I refractory and is one of the more reliable clinical scenarios. However, the practicing physicians must be aware of reports that post-131I therapy scans may miss as many as 7.5–12% of metastases of DTC that do indeed have radioactive iodine uptake if the scan had been performed at a different time point (54 –57). Thus, while this clinical scenario still conveys a very high likelihood of 131I-refractory disease, it is not definitive proof of 131I-refractory disease.
Clinical Scenario 3: Radioactive iodine uptake is only present in some but not other tumor foci.
Simply because one or more metastases are non-131I avid, the disease should not be categorized de facto as 131I refractory. It may be possible to apply local treatment to the site(s) of non-131I-avid lesions (e.g., surgery, radiotherapy, radiofrequency ablation, cryotherapy, embolization, etc.) and concurrently effectively treat the 131I-avid tumors with 131I therapy.
Clinical Scenario 4: DTC metastases progress despite 131I uptake.
The confounding factors that must be considered in this scenario include but are not limited to (i) the metric(s) for successful response to the last 131I therapy, (ii) the duration of that response, (iii) the metric(s) for progression after 131I therapy, (iv) the amount of prescribed activity of 131I administered, (v) the potential for administering a higher activity of 131I, and (vi) the assessment of side effects and the patient's risk-to-benefit tolerance. Slow or no progression for an acceptable period of time may be considered effective 131I therapy and an indication for additional 131I therapy rather than for a designation as 131I refractory. Of course, what is considered an “acceptable” duration of response is subjective and will likely vary based on the specific clinical situation. Nevertheless, simply documenting any degree of tumor growth at any time point after 131I therapy is not an adequate justification for classifying DTC as 131I refractory.
Clinical Scenario 5: DTC metastases progress despite a cumulative
As the cumulative 131I activity and number of therapies increase, the likelihood of DTC becoming 131I refractory will increase (58,59). However, just because cumulative activity has exceeded 22.2 GBq (600 mCi), DTC should not by definition, classification, or criteria be labeled as 131I refractory. Factors such as response to previous therapies, duration of response, the individual and not cumulative activity administered for each previous 131I treatment, side effects, and the patient's view with regard to the risk-to-benefit ratio should influence the decision of whether to continue with further 131I administrations.
The arbitrary cut point of cumulative activity of 131I > 22.2 GBq has been used as one of the eligibility criteria to define 131I-refractory disease in prospective clinical trials evaluating outcomes in multitargeted kinase inhibitors. Thus, the 22.2 GBq scenario is well known to endocrinologists, oncologists, and nuclear medicine specialists and is therefore specifically addressed. The purpose of discussing the 22.2 GBq cutoff value is not to adopt or recommend this cutoff, but rather to underline the fact that this cutoff should not be interpreted and implemented as an absolute criterion for 131I-refractory disease.
Clinical scenarios characterizing a patient as likely to be 131I refractory will continue to evolve as (i) additional studies address important limitations and technical issues confounding the current literature, and (ii) techniques for radioactive iodine scanning are standardized and optimized. Furthermore, the continuous efforts in the development of re-differentiation therapies to enhance the effectiveness of 131I therapy may, if ultimately successful, require a re-evaluation of patients currently considered to be 131I refractory. In addition, the role of molecular testing in determining the risk of having 131I-refractory disease also requires additional study.
Unfortunately, the lack of high-quality studies addressing most of these critical management issues makes consensus by panels of experts difficult. There are still numerous open topics that require such studies to guide clinicians in DTC management. They range from the use of US, molecular markers, and imaging in the diagnostic process through the extent of surgery to various questions pertaining to appropriate use of 131I therapy and the role of personalized dosimetry. Ideally, such studies should be prospective, randomized, and controlled. Furthermore, they should evaluate patient-relevant outcome measures (i.e., quality of life, recurrence rate, and progression-free, disease-specific, and/or overall survival). It is only with high-quality studies that are properly designed and which control for known variables that the most important questions can be answered.
However, it is the comparatively indolent behavior and high survival rates of most DTCs that make prospective studies that address important oncological outcomes (e.g., disease-specific or overall survival) difficult if not impossible to perform. Based on previous literature, follow-up should be at least 10–15 years, with enrollment requirements that would be difficult to achieve (multiple hundreds per study arm).
The indolent course of DTC, the long follow-up, and the large patient numbers required in most trials will necessitate multicenter international efforts. The societies involved in the present effort have the expertise, access to potential study participants, and other resources required to address a large number of these important issues. It is also critical to gain input from patients by consulting with representative patient societies in all these initiatives.
Conclusions
It is perhaps surprising that more than 70 years after the first use of 131I for hyperthyroidism by Saul Hertz and Arthur Roberts at the Massachusetts General Hospital in 1941 (reviewed in Bonnema and Hegedüs) (60), there are still controversies regarding the therapeutic use of 131I for DTC. While the Martinique Principles provide a framework for many important management issues in DTC, ongoing discussions will be required to address many of the specifics that arise as one considers implementing these principles in clinical practice. These include critical issues such as the optimal method of preparation for 131I therapy (e.g., low-iodine diet, recombinant human TSH vs. thyroid hormone withdrawal), assessment of postoperative disease status, precise definition of “successful remnant ablation” and “successful response to the last 131I therapy,” recommendations regarding administered activity for remnant ablation, the role of diagnostic radioactive iodine scans prior to 131I therapy in the setting of remnant ablation, adjuvant treatment, and treatment of known disease, specific isotopes to be used for radioactive iodine scanning, potential utility of personalized dosimetry (both lesional dosimetry and whole-body or blood dosimetry studies), refinement of the clinical scenarios that describe 131I-refractory disease, establishing minimum criteria for “appropriately performed” radioactive iodine imaging, and integration of the side effect profile of 131I therapy into the decision-making process to optimize the risk–benefit ratio. Unfortunately, these critical issues could not be adequately evaluated, presented, and discussed within the time constraints of the initial joint meeting in Martinique.
International collaborations between different disciplines and the progress in technology offer the potential to address 131I therapy comprehensively and with a long-term, interdisciplinary, and patient-orientated perspective for the first time. By fostering an open, productive, evidenced-based discussion, the Martinique meeting restored trust, confidence, and a sense of collegiality between individuals and organizations that are committed to optimal management for patients with thyroid disease. While this initial meeting focused specifically on organizational interactions, proper use of 131I as adjuvant treatment, and the clinical scenarios of 131I-refractory disease, future meetings are expected to cover a wider range of topics relevant to both benign and malignant thyroid disease. With the benefit of these collaborations, it is hoped that future guidelines will benefit from the wealth of experience from the broad range of specialists treating thyroid disease.
Footnotes
Acknowledgments
The boards of directors of all four societies—the ATA, the EANM, the ETA, and the SNMMI—have endorsed this article. This work has not received any specific funding beyond the support of each society for travel expenses in the context of the meeting in Martinique.