
Abstract
Background:
Overt thyroid diseases have been identified as risk factors for female infertility. However, it remains largely unclear whether subclinical hypothyroidism (SCH), a very common thyroid disorder, is associated with female infertility. This study aimed to investigate the potential association between SCH and the ovarian reserve in women seeking infertility treatment.
Methods:
This retrospective study included 2568 women with normal thyroid function (n = 2279) or SCH (n = 289) who visited our clinic for infertility treatment. Ovarian reserve markers, including follicle-stimulating hormone (FSH) concentrations on days 2–4, the antral follicle count (AFC), and anti-Müllerian hormone (AMH) concentration, were compared between euthyroid women and those with SCH. Multiple linear and Poisson regression analyses were used to estimate the associations of SCH with ovarian reserve markers. These analyses were repeated separately in women aged <35 (n = 1349) and ≥35 years (n = 1219).
Results:
In the total study population, women with SCH had significantly lower AMH concentrations (median: 2.05 vs. 2.51 ng/mL, p = 0.015) and AFCs (median: 10.0 vs. 11.0, p = 0.013), compared with euthyroid women. In linear and Poisson regression analyses, SCH was significantly associated with a higher basal FSH concentration (mean difference = 1.13 mIU/mL [95% confidence interval (CI) 0.97 to 1.29 mIU/mL], p < 0.001), lower AMH concentration (mean difference = −0.27 ng/mL [CI −0.43 to −0.12 ng/mL], p = 0.001), and lower AFC (mean difference = −0.7 [CI −1.3 to −0.2], p = 0.005). In women aged ≥35 years, SCH was significantly associated with FSH (mean difference = 1.74 mIU/mL, p < 0.001) and AMH concentrations (mean difference = −0.40 mg/mL, p < 0.001) and AFC (mean difference = −0.8, p < 0.001). In women <35 years old, SCH was significantly associated with a higher FSH concentration (mean difference = 0.30 mIU/mL, p < 0.001), but not with AMH or AFC concentrations (p = 0.84 and 0.06, respectively). Thyroperoxidase antibody (TPOAb) positivity was not associated with measures of ovarian reserve.
Conclusions:
The data suggest that SCH is associated with decreased ovarian reserve during later reproductive age. TPOAb positivity was not associated with ovarian reserve. Future research is necessary to investigate the underlying molecular mechanisms regulating the diminished ovarian reserve in women with SCH and to evaluate whether levothyroxine supplementation may improve the ovarian function of women with SCH.
Introduction
Subclinical hypothyroidism (SCH) is defined as an elevated serum thyrotropin (TSH) with a normal serum free thyroxine (fT4) level. This condition affects 3–8% of women of childbearing age (1,2). When diagnosed before conception, SCH has been associated with a higher miscarriage rate, lower live birth rate (3), lower gestational age at delivery, and lower birth weight (4). During pregnancy, SCH was shown to be associated with increased risks of miscarriage and preterm birth (5). Several recent meta-analyses have further confirmed the above findings (2,6).
Both the quality of the embryo and the subsequent clinical outcomes are known to be influenced by both the woman and her male partner. In other words, the potential effect of sperm quality is very difficult to exclude. Therefore, an evaluation of ovarian function and oocyte quality would be expected to reflect more directly the effect of thyroid dysfunction on female reproduction. To date, few studies have reported the association between the TSH concentration and ovarian reserve. The studies that did address this relationship all involved small numbers of patients, and their conclusions remain controversial. In 2011, Michalakis et al. reported a statistically significant association between the incidence of diminished ovarian reserve and increasing TSH concentrations. Specifically, 18% of patients with high TSH (>4.0 μIU/mL) were diagnosed with diminished ovarian reserve (7). Furthermore, Kuroda et al. reported an inverse correlation of the anti-Müllerian hormone (AMH) concentration with the TSH concentration in infertile Japanese women of reproductive age (8). However, this finding was contradicted by another study of euthyroid infertility patients, which found that women with a TSH level of <3.0 μIU/mL had significantly better functional ovarian reserve (i.e., higher AMH) than those with a TSH level of ≥3.0 μIU/mL, after adjusting for autoimmune thyroid disease and age (9). Still other studies failed to establish any association between TSH and ovarian reserve markers. In 2017, Chen et al. reported no significant differences in TSH levels between patients with low, normal, and high ovarian reserves in a cohort of 1044 women (10). A very recent study by Korevaar et al. of 436 women seeking infertility treatment failed to demonstrate significant correlations of the TSH concentration with the antral follicle count (AFC) and day 3 follicle-stimulating hormone (FSH) concentration (11).
Generally, the ovarian reserve decreases gradually after 35 years of age (12,13). Correspondingly, older women of reproductive age are more likely to experience thyroid dysfunction, including SCH (14). These facts led to the hypothesis that a decreased ovarian reserve is associated with a higher incidence of mildly deficient thyroid function. Therefore, we investigated the association between SCH and ovarian reserve in a large population of women receiving treatment based on assisted reproductive technology (ART).
Methods
Study design and population
This retrospective study was conducted at the Reproductive Medical Center of the First Affiliated Hospital of Kunming Medical University between June 1, 2016, and November 30, 2018. New patients who were initially evaluated at our infertility clinic were offered screening examinations to determine whether further ART treatments were necessary. These examinations included transvaginal ultrasonography to determine the AFC, hysterosalpingography (if necessary), and blood sample collection on days 2–4 of the menstrual cycle to measure the serum levels of reproductive hormones, AMH, and markers of thyroid function. The demographic and clinical data of patients who underwent intrauterine insemination (IUI) with their male partner's sperm, in vitro fertilization and embryo transfer (IVF-ET), or intracytoplasmic sperm injection (ICSI) were recorded in a database.
The study inclusion criteria were as follows: (i) female patients aged ≤50 years; (ii) treatment with IUI or IVF/ICSI; and (iii) an euthyroid or SCH status. Women who were diagnosed with polycystic ovarian syndrome, endometriosis, or overt thyroid dysfunction, or who had a history of thyroid disease (treated or not), pelvic surgery, or ovarian tumor were excluded. Finally, 2568 women were included in the data analysis, including 2279 euthyroid women and 289 women with a diagnosis of SCH (Fig. 1). Overall, 1349 and 1219 of the women were aged <35 and ≥35 years, respectively. A total of 2243 patients underwent IVF/ICSI, while the remaining 325 patients underwent IUI.
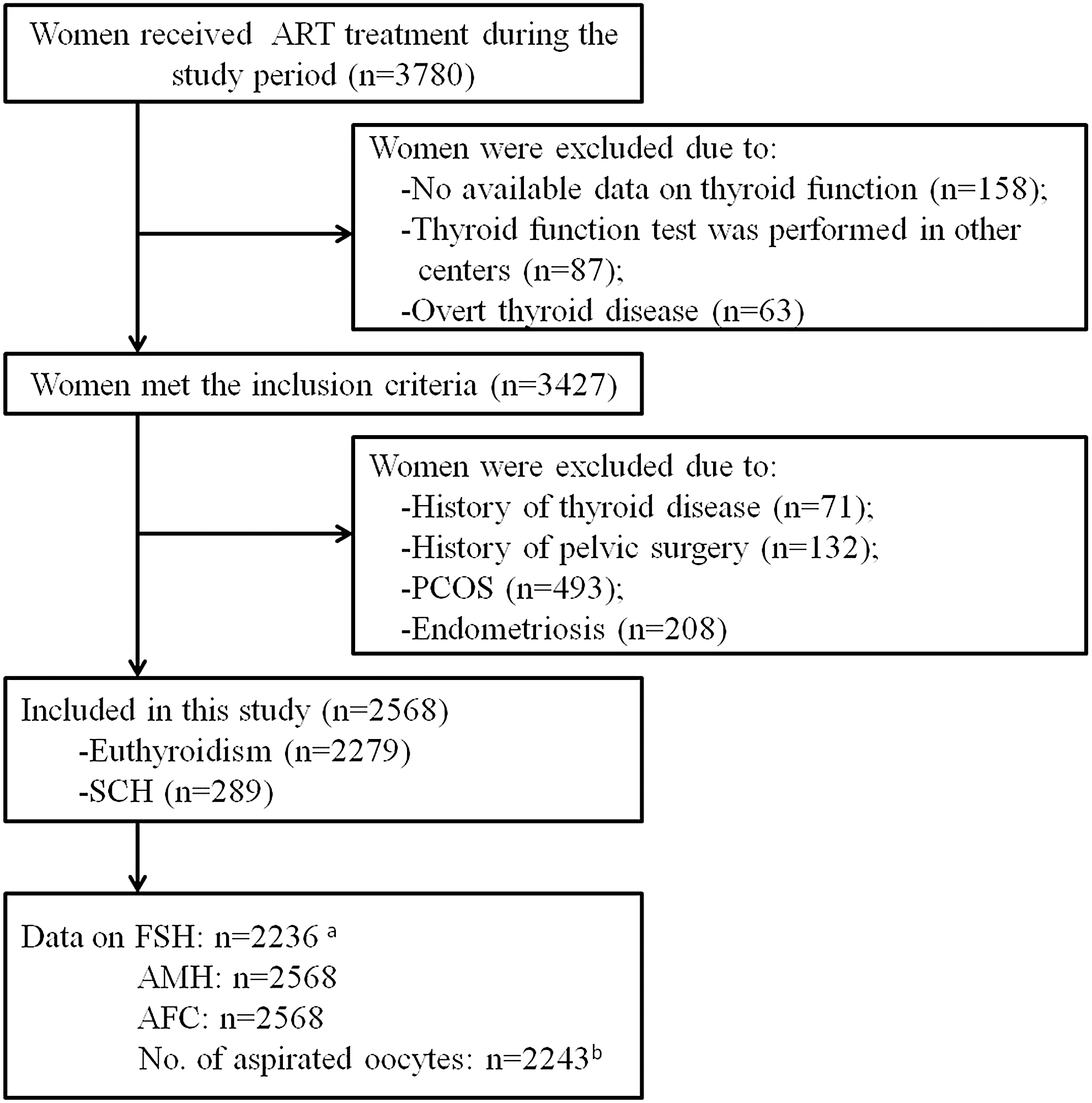
Flowchart of study population selection. aReproductive hormone measurements during days 2–4 of the menstrual cycle were performed in only 2236 women (1986 euthyroid women and 250 women with SCH). bTwo thousand two hundred forty-three participants received in vitro fertilization/intracytoplasmic sperm injection treatment. AFC, antral follicle count; AMH, anti-Müllerian hormone; FSH, follicle-stimulating hormone; PCOS, polycystic ovarian syndrome; SCH, subclinical hypothyroidism.
Measurement of AFC
The ovarian AFC levels were assessed on days 2–4 of an unstimulated menstrual cycle. The AFC was defined as the sum of the antral follicles (2–9 mm in diameter) in both ovaries in the early follicular phase. The follicles were measured via transvaginal ultrasound performed by two well trained reproductive endocrinologists, as described in a previous study (15).
Measurement of AMH
The serum AMH concentration was assayed using a commercially available ELISA kit (Kangrun Biotech, Guangzhou, China) and a plate reader (EXL808; BioTek Instruments), as described in an earlier study (16). The kit sensitivity was 0.06 ng/mL. The intra- and interassay coefficients of variation (CVs) were ≤15% and ≤10%, respectively.
Measurement of reproductive hormones
The serum levels of FSH, luteinizing hormone (LH), estradiol (E2), and progesterone were measured using electrochemiluminescence immunoassays on a Cobas E601 analyzer (Roche, Mannheim, Germany), as described previously (17). The ranges of intra-assay CVs for the FSH, LH, E2, and progesterone assays were 1.3–2.8%, 0.6–1.2%, 1.1–6.7%, and 2.3–5.3%, respectively. The ranges of interassay CVs for FSH, LH, E2, and progesterone were 3.6–4.5%, 1.6–2.2%, 1.9–5.7%, and 3.2–8.2%, respectively.
Measurement of thyroid function
The serum TSH, free triiodothyronine (fT3), fT4, thyroperoxidase antibody (TPOAb), and thyroglobulin antibody (TgAb) concentrations were also measured using ELICAs on a Cobas E601 analyzer (Roche), as described in a previous publication (18). The following reference ranges were recommended by the manufacturer: 0.27–4.20 μIU/mL for TSH, 3.1–6.8 pmol/L for fT3, 12–22 pmol/L for fT4, < 10.0 IU/mL for TgAb, and <34 IU/mL for TPOAb. The ranges of intra-assay CVs for TSH, fT3, fT4, TgAb, and TPOAb were 1.1–3.0%, 1.3–6.5%, 1.6–5.0%, 1.8–2.1%, and 2.8–4.8%, respectively. The ranges of interassay CVs for TSH, fT3, fT4, TgAb, and TPOAb were 3.2–7.2%, 1.6–7.2%, 1.9–6.3%, 4.6–5.1%, and 3.5–6.1%, respectively. A diagnosis of SCH was made if the TSH concentration was >4.2 mIU/mL, while the fT4 concentration remained within the reference range (12–22 pmol/L). A TPOAb concentration >34 IU/mL was considered positive.
Ovarian stimulation and oocyte aspiration
The women were treated with different ovarian stimulation protocols, including long-term GnRH agonist (long protocol, n = 1093), GnRH antagonist (antagonist protocol, n = 514), mild stimulation protocol (n = 555), natural cycle protocol (n = 41), and other protocols (n = 40) according to the patients' conditions, as detailed in previous studies (19 –21). An adjusted dose (1.0 to 2.0 mg) of triptorelin depot (Decapeptyl; Ipsen Pharma Biotech, Paris, France) was used for the long protocol, according to the patients' weight and body mass index (BMI). The GnRH antagonist (Cetrotide; Serono, Geneva, Switzerland) (0.25 mg/day) was used for the antagonist protocol. The results of B-ultrasound imaging and serum hormone levels guided the clinicians' decisions on the timing and dosage of the gonadotropin (Gonal-F; Merck Serono, Geneva, Switzerland). Recombinant human chorionic gonadotropin (HCG, 250 mg, Ovidrel; Serono) was administered when two leading follicles reached a mean diameter of 18 mm. Oocytes were retrieved transvaginally 34–36 h after HCG administration, and the follicles were aspirated using a single lumen needle attached to a syringe under transvaginal ultrasound guidance. The oocytes were identified in a culture dish using a stereomicroscope.
Statistical analysis
The serum FSH and AMH concentrations, AFC, and the number of aspirated oocytes were used to evaluate the ovarian reserve. As none of these parameters was normally distributed, the results are presented as medians (interquartile ranges). We initially used the Mann–Whitney U test (continuous variables) or chi-square test (categorical variables) to compare differences in demographic and clinical data between euthyroid women and women with SCH. The associations of SCH with AFC and number of aspirated oocytes were analyzed using multivariable generalized linear models with a Poisson distribution and log-link function. The associations of SCH with FSH and AMH were analyzed using multivariable linear regression models. The FSH and AMH values were subjected to log(10) transformation before all regression analyses to reduce skewness, as described in previous studies (22,23). The models were adjusted for the women's age, BMI, infertility diagnosis, and TPOAb positivity. The ovarian stimulation protocol was also adjusted when the dependent variable was the number of aspirated oocytes.
To investigate the potential effect of the patient's age on the association between SCH and ovarian reserve, we tested the interaction by adding a product term of SCH (yes/no) and the patient's age (SCH × age) to the model. We also performed a regression analysis stratified by age. Here, subgroups of women aged <35 and ≥35 years were analyzed separately to determine whether the associations between SCH and ovarian function varied between younger and older women. To evaluate whether TPOAb positivity affected the ovarian reserve, the patients were further subdivided into four groups: euthyroidism, isolated SCH, isolated TPOAb positivity, and SCH complicated with TPOAb positivity (SCH+TPOAb positivity). Poisson and linear regression models were also utilized while adjusting for the women's age, BMI, and infertility diagnosis. We also used regression models to evaluate the associations between SCH and ovarian reserve markers in women who received a different infertility diagnosis after adjusting for age, BMI, and TPOAb positivity. The associations of TSH with FSH, AMH, AFC, and the number of aspirated oocytes were also analyzed, and nonlinearity was assessed using restricted cubic splines with three knots. All of the statistical tests were two sided, and a p-value <0.05 was considered statistically significant. SPSS 25.0 (SPSS, Inc., Chicago, IL) and R 3.5.0 (packages rms and ggplot2) were used for the data analysis.
Given the observational nature of our study and no available reference for the association of SCH with ovarian reserve, a sample size calculation was not part of the initial design of our study. In this study, AMH was regarded as a major marker to reflect the ovarian reserve, our sample size of 2568 (2279 in the euthyroidism group and 289 in the SCH group) has a power of 88% to detect a difference of 0.5 ng/mL in AMH levels between groups, with a significance level (alpha) of 0.05 using a one-sided Mann–Whitney test. Sample size calculation was performed in PASS 11 software.
Ethical approval
This study was approved by the First Affiliated Hospital of Kunming Medical University. All patients provided signed informed consent before enrollment into an ART treatment cycle and agreed to the use of their clinical data for scientific research.
Results
Characteristics of the enrolled participants
The ages of the 2568 women ranged from 20 to 50 years. Descriptive characteristics of the included participants are presented in Table 1. There were no significant differences in the mean age and BMI between euthyroid women and women with SCH (p = 0.22 and 0.56, respectively). The levels of reproductive hormones (FSH, LH, E2, and progesterone) were similar between the two groups. The TPOAb and TgAb levels were tested in only 2173 women. The incidence of TPOAb positivity was higher in the SCH group than in the euthyroid group (26.1% vs. 10.9%, p < 0.001). Furthermore, the median AFC and AMH concentrations were significantly lower in women with SCH than in euthyroid women (10 vs. 11 and 2.05 vs. 2.51 ng/mL, respectively; p = 0.013 and 0.015, respectively). In addition, a lower median value of the number of aspirated oocytes was observed in women with SCH (5.5 vs. 8.0), although the difference was not statistically significant (p = 0.054).
Characteristics of Included Participants
Reproductive hormone measurements during days 2–4 of the menstrual cycle were performed in only 2236 women (1986 euthyroid women and 250 women with SCH).
TPOAb test was only conducted in 2173 women (1928 euthyroid women and 245 women with SCH).
Two thousand two hundred forty-three participants received in vitro fertilization/intracytoplasmic sperm injection treatment. Other parameters were measured in all these 2568 women.
AFC, antral follicle count; AMH, anti-Müllerian hormone; BMI, body mass index; E2, estradiol; FSH, follicle-stimulating hormone; fT3, free triiodothyronine; fT4, free thyroxine; IQR, interquartile range; LH, luteinizing hormone; P, progesterone; SCH, subclinical hypothyroidism; TPOAb, thyroperoxidase antibody; TSH, thyrotropin.
Associations of SCH with ovarian reserve markers in the overall population
In the total study population, patients with SCH had a significantly higher day 2–4 FSH level than euthyroid women (adjusted mean: 8.41 vs. 7.28 mIU/mL, mean difference = 1.13 mIU/mL, p < 0.001). In contrast, patients with SCH had significantly lower concentrations of AMH and AFC than euthyroid women (adjusted mean: 2.87 vs. 3.15 ng/ml, mean difference = −0.27 ng/mL, p = 0.001 and adjusted mean: 10.3 vs. 11.0, mean difference = −0.7, p = 0.005, respectively). Patients with SCH also had a significantly lower number of aspirated oocytes than euthyroid women (adjusted mean: 8.0 vs. 8.4, mean difference = −0.4, p = 0.03), as shown in Table 2.
Associations Between Subclinical Hypothyroidism and Ovarian Reserve Markers in Women Overall
CI, 95% confidence interval.
Associations of SCH with ovarian reserve markers in women aged <35 and ≥35 years
To investigate whether the woman's age would affect the association between SCH and ovarian reserve, we performed a subgroup analysis after stratifying the patients by age (<35 and ≥35 years). Among women aged <35 years, a slightly but significantly higher FSH level was observed in women with SCH than in euthyroid women (adjusted mean: 6.84 vs. 6.55 mIU/mL, mean difference = 0.30 mIU/mL, p < 0.001). In contrast, SCH was not significantly associated with the AMH concentration (adjusted mean: 4.08 vs. 4.09 ng/mL, mean difference = −0.01 ng/mL, p = 0.84), AFC (adjusted mean: 12.7 vs. 13.3 ng/mL, mean difference = −0.6, p = 0.06), or the number of aspirated oocytes (adjusted mean: 11.3 vs. 10.9, mean difference = 0.4, p = 0.21) in this subgroup. Among women aged ≥35 years, SCH was significantly associated with an increased FSH concentration (adjusted mean: 9.77 vs. 8.03 mIU/mL, mean difference = 1.74, p < 0.001) and a decreased AMH concentration (adjusted mean: 1.68 vs. 2.08 ng/mL, mean difference = −0.40, p < 0.001), AFC (adjusted mean: 7.5 vs. 8.3, mean difference = −0.8, p < 0.001), and number of aspirated oocytes (adjusted mean: 5.1 vs. 5.9, mean difference = −0.8, p < 0.001), as shown in Table 3.
Associations Between Subclinical Hypothyroidism and Ovarian Reserve Markers in Women Stratified by Age
Ref., reference.
The association of SCH with FSH and the number of aspirated oocytes differed for younger versus older women (p for difference = 0.037 and <0.001, respectively), but the association of SCH with AMH or AFC did not (p for difference = 0.37 and 0.17, respectively).
Associations of SCH with ovarian reserve markers in women with different infertility diagnoses
Of the total study population, 1499, 650, 209, 173, and 37 women were characterized as having tubule factor infertility, diminished ovarian reserve, male factor infertility, unexplained infertility, and ovulation dysfunction, respectively. In patients with tubule factor infertility, SCH was significantly associated with an increased FSH (adjusted mean: 7.43 vs. 6.47 mIU/mL, mean difference = 0.96 mIU/mL, p < 0.001) and decreased AMH concentration (adjusted mean: 3.48 vs. 3.71 ng/mL, mean difference = −0.23 mg/mL, p = 0.004). Although women with SCH also had a lower AFC (adjusted mean: 11.9 vs. 12.5) and number of aspirated oocytes (9.4 vs. 9.9) compared with women with euthyroidism, these differences were nonsignificant (p = 0.06 and p = 0.12, respectively). In patients with diminished ovarian reserve, SCH was significantly associated with an increased FSH concentration (adjusted mean: 11.37 vs. 10.73 mIU/mL, mean difference = 0.63 mIU/mL, p < 0.001), whereas the AMH concentration, AFC, and the number of aspirated oocytes did not differ significantly between patients with SCH and euthyroidism (p = 0.13, 0.73, and 0.20, respectively). In patients with unexplained infertility, SCH was significantly associated with an increased FSH concentration and decreased AMH concentration and AFC (p < 0.001, 0.041, and 0.027, respectively). In patients with male-factor infertility and ovulation dysfunction, no significant associations of SCH with ovarian reserve markers were observed (all p > 0.05), as shown in Table 4.
Associations Between Subclinical Hypothyroidism and Ovarian Reserve Markers in Women Stratified by Infertility Diagnosis
Associations of SCH and/or TPOAb positivity with ovarian reserve
In the total study population, 1718, 181, 210, and 64 patients were characterized as having euthyroidism, isolated SCH, isolated TPOAb positivity, and SCH+TPOAb positivity, respectively. A multivariable regression analysis revealed significant differences in FSH and AMH concentrations and AFC across these four groups. The FSH levels were significantly higher in women with isolated SCH (adjusted mean: 8.08 mIU/mL) and women with SCH+TPOAb positivity (adjusted mean: 8.12 mIU/mL), compared with euthyroid women (adjusted mean: 7.34 mIU/mL, both p < 0.001). Similarly, patients with isolated SCH and SCH+TPOAb positivity had significantly lower AMH concentrations, compared with euthyroid women (adjusted mean: 2.80 vs. 3.19 ng/mL, 2.80 vs. 3.19 ng/mL, p = 0.001 and 0.009, respectively). A significant association was observed between isolated SCH and a decreased AFC (p = 0.005) and number of aspirated oocytes (p = 0.017), whereas isolated TPOAb positivity was not associated with the FSH, AMH, AFC, or the number of aspirated oocytes (p = 0.42, 0.25, 0.92, and 0.16, respectively), as shown in Table 5.
Ovarian Reserve Between Euthyroid Women and Women with Subclinical Hypothyroidism and/or Thyroperoxidase Antibody Positivity
Associations of TSH with ovarian reserve
Patients were subdivided into three groups according to two TSH cutoff values: 2.5 and 4.2 mIU/mL. Accordingly, 1337, 942, and 289 patients were found to have TSH levels of ≤2.5, 2.5–4.2, and >4.2 mIU/mL, respectively. No differences in FSH and AMH concentrations and AFC were observed between patients with a TSH ≤2.5 mIU/mL and those with a TSH of 2.5–4.2 mIU/mL (p = 0.80, 0.87, and 0.56, respectively) (Table 6). Furthermore, the regression models demonstrated that TSH was significantly and positively associated with FSH (p = 0.025) and negatively associated with AMH (p = 0.022), AFC (p = 0.009), and the number of aspirated oocytes (p = 0.038) (Fig. 2).

The plots show the association of TSH with FSH, AMH, AFC, and the number of aspirated oocytes. The black line is the predicted mean value of FSH, AMH, AFC, and the number of aspirated oocytes, and the gray area is the corresponding 95% confidence interval. TSH, thyrotropin.
Ovarian Reserve Between Euthyroid Women and Women with Subclinical Hypothyroidism, When the Cutoff Values of Thyrotropin 2.5 and 4.2 mIU/mL Were Used
Compared with women with a TSH between 0.27 and 2.5 mIU/mL.
Discussion
This population-based study investigated the association between SCH and ovarian reserve in women of reproductive age. The results demonstrate that SCH was associated with a higher basal FSH concentration and a lower AMH, AFC, and number of aspirated oocytes following controlled ovarian stimulation. However, further analysis indicated that those associations were only present in women aged ≥35 years. Furthermore, TPOAb positivity was not associated with ovarian reserve. Taken together, the results of this study suggest that SCH is associated with a lower ovarian reserve in older women of reproductive age (≥35 years).
In 2016, Weghofer et al. reported that in euthyroid patients with infertility, a TSH <3.0 μIU/mL was associated with a higher AMH concentration (relative to a TSH ≥3.0 μIU/mL), suggesting a beneficial effect of a lower TSH level on follicular recruitment (9). Similarly, another study of girls aged 10–18 years observed a negative correlation between the serum concentrations of AMH and TSH (24). In 2017, a population-based cohort study of Chinese women (n = 184,611) showed that an elevated preconception TSH concentration was associated with increased risks of miscarriage and preterm birth (10). These adverse pregnancy outcomes may be at least partially attributable to decreases in ovarian function and oocyte quality in women with elevated TSH concentrations (25 –27). Our results are consistent with the abovementioned findings, despite differences in the analytical approaches and TSH cutoff values among the studies. Our conclusions are further strengthened by those of another recent study, which showed that levothyroxine supplementation improved the serum AMH concentrations of infertile patients with preconception TSH concentrations of ≥2.5 μIU/mL and thyroid autoimmunity (28). Both SCH and thyroid autoimmunity have been recognized as mild forms of thyroid dysfunction that may reflect a relatively low thyroid functional capacity. This dysfunction may become apparent during a state of increased demand for TSH synthesis such as early pregnancy, despite an fT4 level within the normal range. Although one study based on a small number of women reported no significant correlations between serum AMH and TSH concentrations, another study found a significant negative correlation between the AMH and TSH concentrations in patients who were either TPOAb-positive or TgAb-positive (29).
The results of this study are inconsistent with earlier findings that the incidence rates of overt hypothyroidism and SCH do not differ significantly between women with low, normal, and high ovarian reserves (30). These inconsistent conclusions may be attributable to differences in the study populations, sample sizes, and approaches to data analysis. The associations between SCH and clinical outcomes after IVF/ICSI have been well documented in several randomized controlled trials (RCTs) and meta-analyses. In addition, levothyroxine supplementation can attenuate the risk of adverse clinical outcomes caused by SCH (31). One potential explanation was the improvement of levothyroxine on oocyte and embryo quality, and luteogenesis (32). Two recent studies reported that women with thyroid carcinoma have a decreased AMH concentration after radioactive iodine therapy (33,34). Taken together, a causal relationship may be established between decreased thyroid capacity and diminished ovarian function. It has been reported that patients older than 35 years are more likely to experience a marked reduction in AMH after radioactive iodine therapy (30), indicating that older women may be more susceptible to deficiencies in thyroid function related to ovarian reserve. This result is consistent with our conclusion that an association between SCH and lower ovarian reserve only exists in women aged ≥35 years. It is worth noting that the age of 35 years is not a very strict cutoff. We selected this cutoff because women older than 35 years generally exhibit obvious decreases in ovarian function (12,13). Therefore, this study demonstrates that aging may amplify the effects of SCH on the ovarian reserve.
It has been reported that the association between SCH and ovarian reserve is affected by the type of infertility diagnosis (11). For example, thyroid function and TPOAb positivity were not found to affect the AFC, whereas patients with a diminished ovarian reserve or unexplained infertility tend to have a lower AFC. In this study, we found that SCH was associated with a lower ovarian reserve in patients with only tubal factor infertility and unexplained infertility, but not those with other infertility diagnoses. These differences may be at least partially due to the large differences in sample sizes among the infertility diagnosis. We hypothesize that thyroid dysfunction may be associated with specific causes of infertility. As reported in a large RCT by Wang et al. (35), levothyroxine supplementation led to improved pregnancy outcomes after IVF in patients with thyroid autoimmunity who were characterized by female factor infertility, but not infertility related to other factors. However, this difference was not statistically significant, indicating that the ovarian function of patients with female-factor infertility may be more susceptible to a mild change in the thyroid functional state. More studies are needed to test this hypothesis and clarify the underlying mechanism.
This study also found no association between TPOAb positivity and ovarian reserve. Specifically, the ovarian reserves of patients with both SCH and TPOAb positivity were not worse than those of patients with isolated SCH. This finding is consistent with another study that found no significant differences in the basal FSH and AMH concentrations between women with TPOAb negativity and positivity (29). However, our conclusion is contradicted by a study in which thyroid autoimmunity was more frequent in patients with primary ovarian insufficiency (36). Although thyroid autoantibodies have been detected in follicular fluid, the influence of these antibodies on folliculogenesis has not yet been determined (37). Other studies have focused on the effect of an elevated but still normal preconception TSH concentration on pregnancy outcomes. For example, a recent population-based study found that women with a preconception TSH concentration of 2.5–4.3 mmol/L had higher risks of spontaneous miscarriage and preterm birth, compared with those with a TSH <2.5 mmol/L (3). However, these increased risks may not be attributable to diminished ovarian function, as our study did not identify any differences in ovarian reserve between patients with higher (2.5–4.2 mIU/mL) and lower (<2.5 mIU/mL) TSH concentrations.
TSH receptors and thyroid hormone receptors are expressed abundantly in human ovarian tissues, including follicles of different stages (38 –40). Accordingly, these receptors may contribute to the regulation of ovarian function. Animal studies have indicated that thyroid hormones enhance FSH-induced preantral follicular development (41) and interact with FSH to suppress granulosa cell apoptosis (42). Furthermore, an inadequate supply of thyroid hormones was shown to disturb folliculogenesis by hindering the differentiation of granulosa cells in prepubertal rats (43). Potentially, thyroid hormones may affect ovarian function by altering nitric oxide synthase activity (44). Furthermore, SCH is thought to reflect a subtle deficiency in thyroid function. Even a slight change in thyroid hormone levels within the reference range may result in a decline in ovarian function, as demonstrated in this study. Ovarian hyperstimulation with exogenous gonadotropins was found to elevate the E2 levels and thus promote the development of mild hypothyroidism (45 –47). Therefore, patients with an elevated TSH should receive prompt levothyroxine supplementation before ovarian stimulation is initiated.
The results of this study suggest that a thyroid function test should be included in the routine screening protocol for female fertility. For a patient with diminished ovarian reserve, consideration should be given to the possibility of thyroid dysfunction. In addition, levothyroxine supplementation may theoretically improve the ovarian function in women with SCH. If this hypothesis is proven to be correct, patients with SCH should be treated before the initiation of ART to improve clinical outcomes.
To the best of our knowledge, this is the largest study to investigate the association between SCH and ovarian reserve. The reliability of the results is enhanced by the application of strict inclusion and exclusion criteria to the participants. Several parameters, including the AFC, AMH, and baseline FSH concentrations, and the number of aspirated oocytes following controlled ovarian stimulation, were used to evaluate the ovarian reserve. In addition, all transvaginal ultrasound detection procedures were performed by two well-trained reproductive endocrinologists. Similarly, all measurements of reproductive hormone levels, thyroid function, and AMH concentrations were conducted by two well-trained technicians to minimize the effects of interassay variability. However, several limitations should be considered when interpreting our results. The first limitation involves the retrospective design, which made it impossible to establish a causal relationship between SCH and a diminished ovarian reserve. Second, the data analyses were only adjusted for the patients' age, BMI, and thyroid autoimmunity. Several other factors that may have affected the associations, including lifestyle habits and dietary patterns, were not recorded in our database and could not be considered. In addition, as all patients were recruited at a single center, a type II error resulting from selection bias cannot be excluded. Finally, the study participants were patients seeking infertility care. Therefore, it remains unclear whether SCH is associated with a decreased ovarian reserve in the general population.
In conclusion, this is the largest study to investigate the association between SCH and ovarian reserve. Notably, our results show that SCH is associated with a lower ovarian reserve in women aged ≥35 years, but not in younger women. Furthermore, we did not find an association between TPOAb positivity and ovarian reserve. Future research is needed to investigate the underlying molecular mechanism that regulates the diminished ovarian reserve in women with SCH and to evaluate whether levothyroxine supplementation may improve the ovarian function of women with SCH.
Footnotes
Acknowledgment
We are grateful to the patients who participated in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (Number 81801416), the Technology and Innovation Team of Reproduction and Genetics at Kunming Medical University (Number CXTD201708), and Scientific Funding from the First Affiliated Hospital of Kunming Medical University (Number 2017BS008).