
Abstract
Background:
The prevalence of antithyroid drug (ATD)-related drug-induced liver injury (DILI) has been reported to vary among patients in several countries. The purpose of this study was to summarize the prevalence of liver injury induced by ATD and to determine the actual prevalence of severe liver injury.
Methods:
The medical records of 18,558 patients who were newly diagnosed with Graves' disease between January 2005 and December 2016 were retrospectively reviewed. Severe DILI was defined as alanine aminotransferase (ALT) 8 times higher than the upper limit of normal (ULN) or total bilirubin (T-bil) 3 times higher than the ULN. The most severe DILI was defined as ALT higher than 20 times the ULN or T-bil higher than 10 times the ULN.
Results:
A total of 461 subjects (470 cases) were analyzed, and they consisted of 10 males and 451 females, with a median age of 37 years (range 10–82 years). Nine of 461 patients had severe DILI with both drugs. The total prevalence of severe DILI in this study was 2.5%, and the prevalence of DILI by drug was 1.4% with metimazole (MMI) (n = 198) and 6.3% with propylthiouracil (PTU) (n = 272) (p < 0.001). The prevalence of the most severe ATD-related DILI was 0.22% (n = 40), and the prevalence for each drug was 0.08% with MMI (n = 11) and 0.68% with PTU (n = 29). The median time to DILI development was 30 days (range 7–314 days), and all patients recovered from DILI, with no fatalities. The prevalence of MMI-related DILI was significantly age dependent (p < 0.001).
Conclusions:
Though there were no fatalities in this study, the prevalence of PTU-related severe DILI was significantly higher than that of MMI-related severe DILI.
Introduction
Treatments for Graves' disease (GD) include antithyroid drug (ATD), surgery, and radioactive iodine (131I) therapy. In Japan, the first-line treatment for GD consists of the use of ATD, which comprises propylthiouracil (PTU) and metimazole (MMI); these agents were introduced for clinical use in 1947 and 1952, respectively (1). Although ATD is not a curative treatment, it is so effective in controlling hyperthyroidism that it would be suitable for almost every patient who chooses it as treatment for GD. On the other hand, these agents have potentially fatal side effects such as agranulocytosis, vasculitis (2 –4), and liver injury, and there have been many case reports describing severe liver injury caused by ATDs (5 –7).
According to a retrospective analysis (8), PTU-related severe drug-induced liver injury (DILI) occurred more frequently at a younger age, especially younger than 17 years old, though this tendency was not seen for MMI-related DILI. Because of the severity of this adverse effect especially for children, the Food and Drug Administration (FDA) of the United States has issued a Black Box Warning on the risk of severe liver injury with PTU in children, and recommended not choosing PTU as first-line medication in children to avoid this potentially fatal adverse event.
The prevalence of ATD-related DILI has been reported to vary among patients from several countries, ranging from 0.03% to 0.5% (9 –13). It is difficult to identify the actual prevalence of ATD-related DILI, because liver enzymes, including transaminase, γ-glutamyltransferase, and alkaline phosphatase (ALP), are highly affected by hyperthyroidism (14,15), and even transient thyrotoxicosis can increase liver enzymes (16).
Based on these facts, the aim of this study was to summarize ATD-related severe DILI and to determine the actual prevalence of severe and fatal liver injury in newly diagnosed Japanese patients with GD.
Materials and Methods
Subjects
A total of 18,588 newly diagnosed patients with GD (3170 males and 15,388 females) to whom an ATD was administered for the first time between January 2005 and December 2016 were enrolled in this retrospective study, and laboratory data were collected from their medical records. GD was diagnosed based on both hyperthyroidism and positive thyrotropin receptor antibody (TRAb) or high RAI uptake. MMI was administered to 14,271 patients (3030 males and 11,241 females), and PTU was administered to the remaining 4287 patients (140 males and 4147 females). Patients who had a history of autoimmune hepatitis, viral hepatitis, fatty liver, alcoholic liver disease, heart failure, constitutional jaundice (Gilbert's disease), primary biliary cholangitis, and liver dysfunction due to other causes were excluded. The patients who had liver dysfunction that met the criteria of severe liver dysfunction used in this study before the initiation of ATD therapy were excluded, as were patients who were lost to follow-up within three months, because the follow-up period was too short to identify the subsequent adverse events of ATD therapy. Patients who developed and recovered from DILI and then were transferred to another hospital within three months were included.
Diagnoses of severe DILI were made following the criteria reported by Tajiri and Shimizu (17). In addition, according to the same criteria, DILI was divided into three types: hepatocellular, cholestatic, and mixed type. The hepatocellular type was defined as serum alanine aminotransferase (ALT) higher than 8 times the upper limit of normal (ULN), or serum ALT higher than 5 times the ULN for more than 2 weeks. On the other hand, the cholestatic type was defined as a serum total bilirubin (T-bil) value higher than three times the ULN. Finally, the mixed type was defined as serum ALT higher than 3 times the ULN, co-existing with a serum T-bil higher than 2 times the ULN.
Following the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 (18), the patients with the most severe DILI were collected. CTCAE was published by the U.S. Department of Health and Human Services, and a grading (severity) scale is provided for each adverse event term. The grade ranges from 1 to 5, and the severity becomes worse as the number of the grade goes up. In detail, grade 1 means mild, and this grade does not need any treatment for the adverse event. Grade 2 means moderate, and minimal intervention is needed. Grade 3 means severe or medically significant, but not immediately life-threatening. Grade 4 is life-threatening, and urgent intervention is required. Finally, grade 5 means death due to the adverse event. Grade 4 was used as the definition of the most severe DILI, since this grade is life-threatening. Specifically, if the value of ALT was higher than 20 times the ULN or 20 times the baseline if the baseline value was abnormal, or the value of T-bil was higher than 10 times the ULN or 10 times the baseline if the baseline level was abnormal, the suspected drugs should be discontinued.
Finally, 461 patients (470 cases) met the criteria. All patients were followed up by using serum T-bil, aspartate aminotransferase (AST), and ALT every 2 weeks for the first 3 months, and then every month to every 4 months to detect liver injury, since routine monitoring is recommended by the Japanese guidelines for the management of GD.
Laboratory methods
Serum ALT values were measured by using the Japan Society of Clinical Chemistry transferable method. Until August 2014, the reference range was 5–40 U/L, and after September 2014, it was 7–23 U/L because of changes in the measurement methodology. The T-bil value was measured by using the chemical oxidation method. The reference range was 0.2–1.2 mg/dL until August 2014, and 0.4–1.5 mg/dL after September 2014. ALP was not used as an index of DILI in this study, because patients with GD are known to have elevated ALP levels due to activated bone metabolism (14).
Serum-free triiodothyronine (fT3) was measured by using an ECLusys fT3 electrochemiluminescence immunoassay kit (Roche Diagnostics, Basel, Switzerland; reference range 2.2–4.3 pg/mL). Serum-free thyroxine (fT4) was measured by using an ECLusys fT4 electrochemiluminescence immunoassay kit (Roche Diagnostics; reference range: 0.8–1.6 ng/dL). Thyrotropin (TSH) was measured by using an ECLusys TSH electrochemiluminescence immunoassay kit (Roche Diagnostics; reference range: 0.2–4.5 μU/mL). The same devices for measuring fT3, fT4, and TSH have been used since May 2004, and, therefore, the reference ranges for these values have been the same throughout the observation period. TRAb were measured with TRAb-CT (Cosmic, Tokyo, Japan) between January 2005 and September 2008. Levels are expressed in terms of the inhibition index of TSH binding and are presented as percentages (the <10% reference range was defined by the manufacturer). Starting from October 2008, all levels were measured by using an ECLusys TRAb electrochemiluminescence immunoassay (Roche Diagnostics; normal range: <2.0 IU/L).
Statistical analysis
The baseline parameters and the collected data were analyzed by using JMP version 14.0 software (SAS Institute, Cary, NC). The prevalence of DILI related to MMI and PTU was compared by using the Chi-squared test. Correlation analyses were performed by using Spearman's rank correlation test, and Pearson's Chi-squared test was used to compare items between age groups.
Results
Patient characteristics and severe DILI
Of the 18,558 newly diagnosed GD patients, 461 patients (2.5%; 10 male and 451 female) matched the criteria for severe DILI. The detailed characteristics of the 461 patients are shown in Table 1. The overall incidence of severe DILI among the newly diagnosed GD patients was 0.32% in males and 2.93% in females. Females had a significantly higher incidence rate of severe DILI than males (p < 0.0001). Nine of these female patients developed DILI after exposure to both MMI and PTU (Table 2). In total, 470 cases were analyzed. The median age of the 461 patients was 37 years (range 10–82 years). Overall, 198 of 470 cases developed MMI-induced DILI (1.4%), and the remaining 272 cases developed PTU-induced DILI (6.3%). Of the 470 cases, 7 (1.5%) had a cholestatic type, 454 (96.6%) had a hepatocellular type, and the remaining 9 had a mixed type (1.9%). The median values of T-bil and ALT at the highest points were 0.8 mg/dL (range 0.3–18.6 mg/dL) and 238.5 U/L (range 16–1424 U/L), respectively. The median time to DILI development was 30 days (range 7–314 days), and the median time to recovery from liver injury was 28 days (range 7–203 days). In total, 456 out of 470 cases (97.0%) developed DILI within 90 days after starting ATD, and the remaining 14 cases developed it after 91 days. The median follow-up period of the 461 patients was 2509 days (range 33–5045 days), and there were 4 patients whose follow-up periods were shorter than 90 days. This was because 3 of 4 of these patients needed immediate surgery and were transferred to another hospital. The one remaining patient was also transferred after recovery from liver injury to another hospital due to moving. As an alternative treatment for GD after recovery from DILI, 165 of 470 cases (35.1%) chose the other ATD: 103 patients switched from PTU to MMI, and 62 patients switched from MMI to PTU; while 186 of 470 cases (39.6%) chose 131I therapy, 29 patients (6.2%) chose surgery, and 55 patients (11.7%) chose potassium iodide. The remaining 35 patients (7.4%) continued the same ATD that was suspected to have caused the liver injury.
Characteristics of the 461 Patients with Severe Drug-Induced Liver Injury
ALT, alanine aminotransferase; DILI, drug-induced liver injury; fT3, free triiodothyronine; fT4, free thyroxine; MMI, metimazole; PTU, propylthiouracil; T-bil, total bilirubin.
Characteristics of the Nine Female Severe Drug-Induced Liver Injury Patients with Both Metimazole and Propylthiouracil
ATD, antithyroid drug; GD, Graves' disease; HC, hepatocellular type; RAI, radioactive iodine; UDCA, ursodeoxycholic acid.
Half of the cases recovered from liver injury after ATD withdrawal, though 205 cases (43.6%) received ursodeoxycholic acid (UDCA) as a treatment, 25 cases (5.3%) received glycyrrhizin, 2 cases (0.43%) received prednisolone (PSL), another 2 cases (0.43%) received a combination of glycyrrhizin and PSL, and 1 case received a combination of PSL and UDCA therapy.
Of these patients, 176 had elevated serum ALT higher than twice the ULN before the initiation of ATD; 31 of the 176 patients had ALT values higher than 100 U/L; and 10 of the 31 patients had ALT values higher than 150 U/L. No patients showed T-bil elevation higher than twice the ULN before the initiation of ATD. The median value of initial ALT was 38 U/L (range 6–180 U/L), and the median initial T-bil was 0.7 mg/dL (range 0.2–3.0 mg/dL).
Median fT3 and fT4 values at the time of DILI diagnosis were 5.4 pg/mL (range 1.6–32.5 pg/mL) and 1.88 ng/dL (range 0.54–7.77 ng/dL), respectively, and their values after recovery from DILI were 4.0 pg/mL (range 0.9–32.5 pg/mL) and 1.29 ng/dL (range 0.22–7.77 ng/dL), respectively. There were no correlations between thyroid hormone values and the levels of T-bil (fT3: r = −0.08, p = 0.17; fT4: r = −0.05, p = 0.29) or ALT (fT3: r = −0.03, p = 0.61; fT4: r = 0.03, p = 0.55).
MMI-induced severe DILI
MMI-induced severe DILI occurred in 198 of 14,271 patients (1.4%). Of the 198 patients, 8 were male, and the remaining 190 were female. The overall incidence was 0.26% in male and 1.69% in female patients. Likewise, in the entire cohort, female patients had a significantly higher incidence of MMI-induced severe DILI than male patients (p < 0.0001). The median age of the 198 patients was 49 years (range 10–82 years), and the median daily dosage of MMI at the time of DILI diagnosis was 15 mg (range 5–30 mg). The median values of T-bil and ALT at the highest point were 0.8 mg/dL (range 0.3–15.7 mg/dL) and 235 U/L (range 16–1424 U/L), respectively. The median time to the development of DILI was 25 days (range 7–155 days) (Fig. 1), and the median time to recovery from liver injury was 29 days (range 8–203 days). Of these 198 patients, 186 (93.9%) had a hepatocellular type, 5 (2.5%) had a cholestatic type, and 7 (3.5%) had a mixed type. Seven of the 198 patients needed to be hospitalized for treatment of liver injury. As an alternative treatment for GD, 74 of 198 patients chose 131I therapy (37.4%), 62 patients chose PTU (31.3%), 8 patients chose surgery (4.0%), 31 patients chose potassium iodide (15.7%), and the remaining 23 patients (11.6%) continued MMI after recovery from liver injury. Median fT3 and fT4 values at the time of DILI diagnosis were 5.4 pg/mL (range 1.6–23.1 pg/mL) and 1.87 ng/dL (range 0.54–7.32 ng/dL), respectively, and after recovery from liver injury, they were 3.8 pg/mL (range 1.5–32.5 pg/mL) and 1.16 ng/dL (range 0.27–7.77 ng/dL), respectively. No correlations were found between thyroid hormone values and the severity of T-bil or ALT elevations. Moreover, there was no correlation between the MMI dose and the severity of liver injury (T-bil: r = −0.08, p = 0.24; ALT: r = 0.08, p = 0.24).
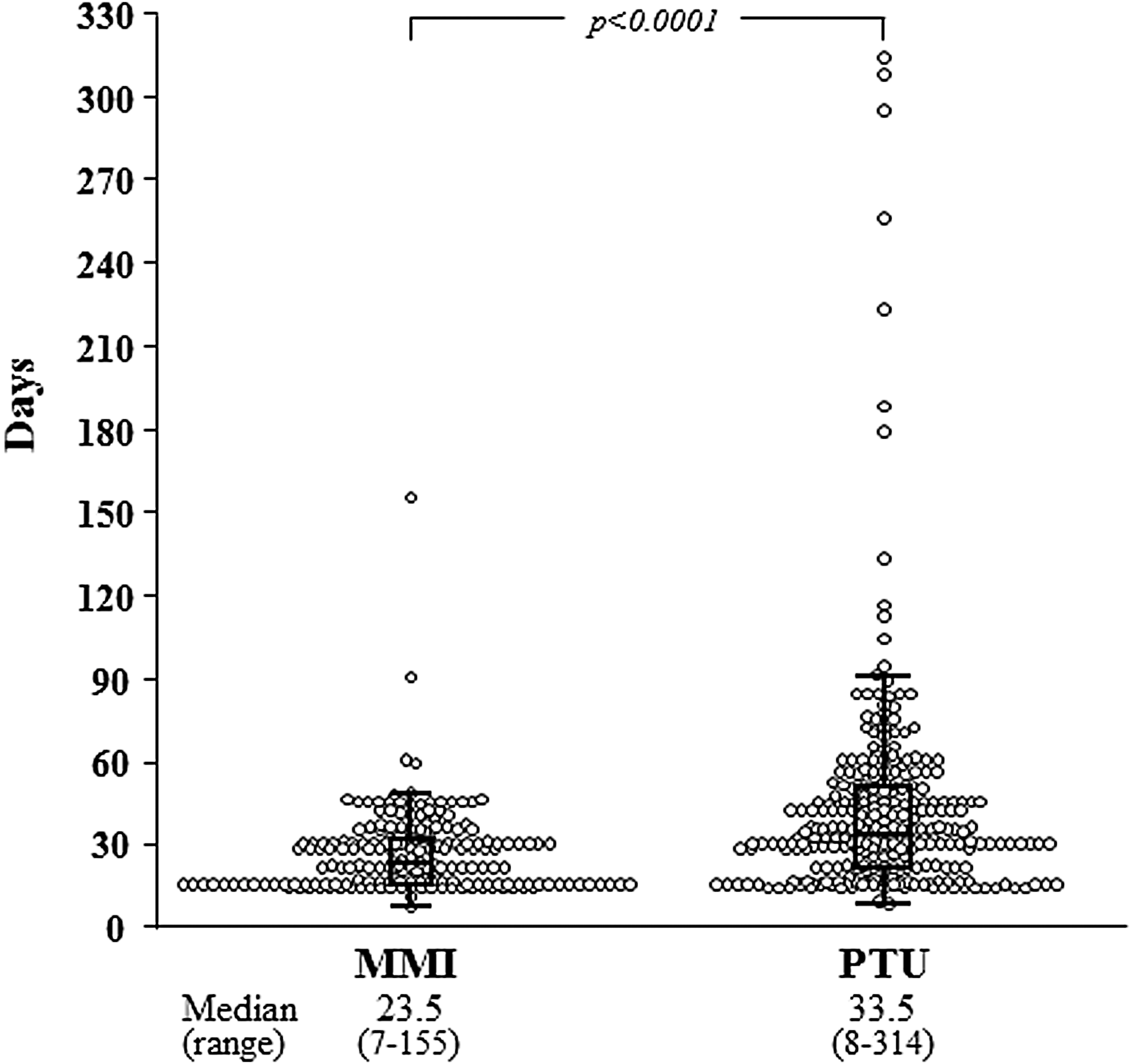
Comparison of the onset of DILI with antithyroid drugs. The median time to develop MMI-related DILI is 23.5 days, while the median time to develop PTU-related DILI is 33.5 days. The median time to the development of PTU-related DILI is significantly longer than that of MMI-related DILI (p < 0.001). DILI, drug-induced liver injury; MMI, metimazole; PTU, propylthiouracil.
PTU-induced severe DILI
Of the 4287 patients, 272 (6.3%) developed PTU-induced DILI. Of these 272 patients, 2 were male and 270 were female, and the overall incidence was 1.43% in male and 6.51% in female patients. Female patients had a significantly higher incidence than male patients (p = 0.015). The median age of these 272 patients was 33 years (range 17–66 years), and the median daily dosage of PTU at the time of DILI diagnosis was 300 mg (range 50–500 mg). The median values of T-bil and ALT at the highest point were 0.8 mg/dL (range 0.4–18.6 mg/dL) and 240 U/L (range 32–1329 U/L), respectively. The median time to DILI development was 33.5 days (range 8–314 days) (Fig. 1), and the median time to recovery from liver injury was 28 days (range 7–168 days). The median time to the development of PTU-DILI was significantly longer than that of MMI-DILI (p < 0.001). Of the 272 patients, 269 (98.9%) had a hepatocellular type, 2 (0.7%) had a mixed type, and 1 (0.4%) had a cholestatic type liver injury. Of the 272 patients, 7 needed to be hospitalized for treatment of liver injury. Alternative treatments for the GD were 131I for 112 patients (41.2%), a switch to MMI for 103 patients (37.9%), surgery for 21 patients (7.7%), potassium iodide for 24 patients (8.8%), and the remaining 12 patients continued PTU (4.4%). The median fT3 and fT4 values at the time of DILI diagnosis were 5.5 pg/mL (range 2.0–32.5 pg/mL) and 1.89 ng/dL (range 0.64–7.77 ng/dL), respectively, and after recovery from liver injury, they were 4.2 pg/mL (range 0.9–32.5 pg/mL) and 1.4 ng/dL (range 0.27–7.77 ng/dL), respectively. No correlations were found between thyroid hormone values and the severity of T-bil or ALT elevations. Similar to MMI, there was no correlation between the PTU dose and the severity of liver injury (T-bil: r = −0.03, p = 0.58; ALT: r = −0.03, p = 0.57). However, there was a significant difference in the prevalence of DILI between MMI and PTU (1.4% vs. 6.3%, p < 0.001).
Patients with the most severe DILI
There were 40 patients (0.22%) who met the criteria of CTCAE severe liver injury greater than grade 4 (the most severe liver injury); 37 were female and 3 were male, and the suspected drug was MMI for 11 patients (0.08%) and PTU for 29 patients (0.68%). Of the 40 patients, 38 had a hepatocellular type, 1 had a cholestatic type, and the other had a mixed type liver injury (Table 3).
Characteristics of the 40 Patients with the Most Severe Drug-Induced Liver Injury
The patients with hepatocellular type liver injury included 35 females and 3 males, with a median age of 36 years (range 20–72 years); 28 developed DILI due to PTU, and the median daily dosage of PTU at the time of DILI diagnosis was 250 mg (range 100–300 mg), while 10 patients developed DILI due to MMI, and the median daily dosage was 15 mg (range 5–30 mg). Median values of T-bil and ALT at the highest point were 1.0 mg/dL (range 0.5–3.8 mg/dL) and 625 U/L (range 462–1424 U/L), respectively. The median time to DILI development was 33 days (range 14–94 days), and the median time to recovery from liver injury was 34.5 days (range 12–203 days). Of the 38 patients, 19 were treated with UDCA for DILI, 6 were treated with glycyrrhizin, and 1 was treated with a combination of PSL and UDCA. The remaining 12 patients did not receive any treatment. Of the 38 patients, 9 needed to be hospitalized. Alternative treatments chosen for the 38 patients were 131I for 25 patients (65.7%), a switch to the other ATD for 8 patients (21.1%), total thyroidectomy for 1 patient (2.6%), and potassium iodide for 4 patients (10.5%). Median fT3 and fT4 values at the time of DILI diagnosis were 5.8 pg/mL (range 2.2–32.5 pg/mL) and 2.07 ng/dL (range 0.7–7.77 ng/dL), respectively, and after recovery from liver injury, they were 3.5 pg/mL (range 0.9–29.9 pg/mL) and 1.16 ng/dL (range 0.22–6.78 ng/dL), respectively.
The patient who developed severe cholestatic type DILI was a 65-year-old woman who was being treated with 15 mg of MMI at the time of the DILI diagnosis. The patient did not need to be hospitalized and recovered from DILI without any treatment except withdrawal of MMI. The values of T-bil and ALT at the highest point were 15.7 mg/dL and 33 U/L, respectively. The time to DILI development was 36 days, and the time to recovery from liver injury was 85 days. She chose RAI therapy as an alternative treatment. fT3 and fT4 values at the time of DILI diagnosis were 2.5 pg/mL and 1.28 ng/dL, respectively, and after recovery from liver injury, they were 4.7 pg/mL and 1.4 ng/dL, respectively.
Finally, the patient who developed a mixed type non-coma fulminant liver failure was a 27-year-old woman who was being treated with 100 mg of PTU at the time of DILI diagnosis. The patient needed to be hospitalized for general intensive care and was treated with PSL pulse therapy combined with UDCA. She recovered from fulminant liver failure without liver transplantation. The values of T-bil and ALT at the highest point were 18.6 mg/dL and 1164 U/L, respectively. The time to DILI development was 91 days, and the time required to recover from liver injury was 82 days. She also chose RAI therapy as an alternative treatment for GD. The fT4 value at the time of DILI diagnosis was 7.77 ng/dL, and the fT3 and fT4 values after recovery from liver injury were 3.3 pg/mL and 0.91 ng/dL, respectively.
Characteristics of ATD-induced DILI by age group
Since the ages of the 461 patients ranged widely, the patients were examined by age. Their detailed characteristics and the prevalence of DILI by age are shown in Table 4. No one in the 70s and 80s age group developed DILI with PTU. In all ages, female patients outnumbered male patients. Among the age groups, except for the 20s and 30s, patients with MMI-related DILI outnumbered those with PTU-related DILI. There was no age dependence in the severity of liver injury, median duration of drug administration, and median time to recovery from liver injury. However, there was a significant age dependence in the prevalence of MMI-related DILI (p < 0.001), which was not seen with PTU (p = 0.1163). That is to say, severe DILI was more prevalent in older patients who took MMI, but there was no age dependence for PTU. The number of patients who met the criteria of severe DILI greater than CTCAE grade 4 in each age group is shown in Table 3. No patient developed severe DILI in the patient group under the age of 20 years (<20s) and in the 80s.
Characteristics of the 461 Antithyroid Drug-Induced Severe Drug-Induced Liver Injury Patients by Age Group
p < 0.0001, MMI versus PTU, ** p < 0.001, age dependence in MMI.
Patients with DILI who could continue the suspected drug
Of the 470 ATD-induced severe DILI cases, 35 could continue the same ATD that was suspected to have caused DILI without interruption, though they needed a reduction of the dosage of ATDs, and their liver function was carefully monitored over a short term. These 35 patients consisted of 23 patients treated with MMI and 12 patients treated with PTU; all subjects were female, with a median age of 38 years (range 12–75 years). The median daily dosage of each drug at the onset of DILI was 10 mg (range 5–30 mg) for MMI and 275 mg (range 100–300 mg) for PTU. All subjects developed hepatocellular type DILI, and no patient needed hospitalization. The median values of T-bil and ALT at the highest point were 0.7 mg/dL (range 0.4–2.1 mg/dL) and 210 U/L (range 185–288 U/L), respectively. The median time to DILI development was 22 days (range 14–155 days), and the median time to recovery from liver injury was 39 days (range 16–137 days). Median fT3 and fT4 values at the time of DILI diagnosis were 3.7 pg/mL (range 2.4–23.1 pg/mL) and 1.51 ng/dL (range 0.72–7.17 ng/dL), respectively, and after recovery from liver injury, they were 3.3 pg/mL (range 2.1–9.0 pg/mL) and 1.15 ng/dL (range 0.57–3.67 ng/dL), respectively.
Discussion
This study analyzed the prevalence of ATD-induced severe DILI in newly diagnosed GD patients in a single medical institute in Japan. According to a previous report, ATD is a common cause of DILI (17), and, especially, PTU is the third most common cause of DILI in patients under the age of 20 years, resulting in liver transplantation in about 10% of GD patients in that age group who developed liver failure (8,19). Compared with the prevalence of ATD-induced DILI reported from the United States (5,8,11), the rates of both MMI and PTU-induced DILI were extremely high in this study. On the other hand, compared with reports from Asian countries (10,12), there was a similar but still higher prevalence. Similarly, the prevalence of the types of liver injury also differed among patients from several countries, since it was reported that the major type of MMI-induced liver injury was cholestasis (5,20), although the reports from China (10), Taiwan (9), and this study had a lower incidence of cholestasis. This difference between the United States and Asian countries might be related to differences in race/ethnicity, the number of included subjects, the method of collecting participants, or the definition of liver injury. Although a study from Taiwan (9) reported a lower frequency compared with the prior two reports from Asian countries, the participants in that study were only hospitalized patients, and that might result in a lower rate. In the present retrospective study, a strict definition of DILI was applied so that false-positive DILI patients should not have been enrolled. As a result, this study shows that the total prevalence of ATD-induced severe DILI was 2.5%, 0.22% for the most severe cases, and these results were higher than expected from previous reports. In 2010, the FDA added a Black Box alert to the label of PTU to inform on the risk of severe liver failure. Because of the risk of fatal DILI induced by PTU, the FDA recommended the use of PTU only for patients who cannot tolerate other treatments for both adults and children. Although there were no fatalities among the present patients, similar to a previous review article (20), this study also shows that PTU had a higher prevalence of DILI (MMI vs. PTU: 1.4% vs. 6.3% and 0.08% vs. 0.68% in severe cases), supporting the notion that PTU is associated with a higher risk of severe liver injury.
According to the report from Woeber (5), the potential risk factors for MMI-induced cholestatic liver injury are older age and higher MMI dosage. Moreover, one review article suggested that the risk factors for MMI-induced cholestatic liver injury were female sex and age 50 years or older; while for PTU-induced hepatocellular liver injury, female sex and age 30 years or younger were risk factors (15). Further, another report studying the two ATDs indicated that PTU-induced liver injury was only observed in the group of patients aged <17 years. However, in this study, there was no trend of dose dependence in developing DILI in both the MMI and PTU groups. On the other hand, similar to previous reports, a significant trend of age dependence in developing DILI was seen in the MMI group, but not in the PTU group. This suggests that for GD patients treated with MMI, the risk for DILI increases as a function of age. The reasons for this trend might be the small number of patients in the older age groups, or perhaps their hepatic reserve could be declining. Thus, we should be cautious about treating older patients with MMI.
A relationship between liver injury and thyrotoxicosis itself has been reported (15,16,21), and the prevalence varies from 37% to 78%, though some of these studies used ALP as an index of liver injury. Since bone turnover is accelerated by hyperthyroidism through direct stimulation of bone cells, ALP derived from bone can remain above the normal limit for up to 20 months after initiating treatment for hyperthyroidism (14,15). Due to this potential uncertainty, this study did not analyze ALP as an index of liver injury. The mechanism of liver injury resulting from hyperthyroidism has been demonstrated in rats (22,23), in which a high concentration of thyroid hormone induces hepatic cell apoptosis through activation of a mitochondrial-dependent pathway. On the other hand, there are known mechanisms of ATD-induced DILI, such as a direct effect of the drug or its metabolites to the cell, or by way of immune responses mediated by metabolites (20,24,25), but they are not completely understood. A possible mechanism explaining PTU-related DILI has been proposed: PTU may form active metabolites that interact with the macromolecules of the endoplasmic reticulum and lead to centrilobular hepatic necrosis (26). On the other hand, Kobayashi et al. (24) demonstrated that an immune response mediated by interleukin-4, a Helper T cell 2 cytokine, is related to the mechanism of MMI-related DILI in rats. In this study, some patients were able to continue the same ATD after the diagnosis of liver injury, even though the values of ALT were high enough to meet the criteria for DILI. The explanations for this could be that the causes of liver injury might be related not only to the ATD but also to other causes, such as an allergic reaction (6,27), or thyrotoxicosis itself could contribute to the liver injury. Liaw et al. (28) suggested that PTU therapy may be continued with caution in patients with asymptomatic liver injury, and for that reason, the 35 patients in this study might have been able to continue the suspected drugs. Moreover, according to Kubota et al. (16), ATD can be continued in patients with ALT as high as 150 IU/L, and this study provides similar results, since it included patients with ALT >184 IU/L. In this study, there were no fatalities, even among the patients who continued ATD. However, this does not mean that continuing ATD should be recommended in cases of severe liver injury, because there is always the risk of fatal DILI during the use of ATD. Thus, ATD should be discontinued promptly if severe DILI is suspected.
This study has some limitations. This is a retrospective, observational study in a single hospital specializing in thyroid disorders, which means that there could have been bias in patient selection, or patients who had very severe liver dysfunction or liver failure might not have been included. Further, there is no evidence demonstrating a benefit of treating DILI with any agents. Thus, treatment criteria and the therapeutic modality for liver injury remain to be established. Therefore, the decision to treat DILI patients currently remains entirely dependent on the choice of the treating physician.
Conclusions
Though there were no fatalities in this study, the prevalence of PTU-related severe DILI was significantly higher than that of MMI-related severe DILI, and the prevalence of MMI-related DILI showed significant age dependence.
Footnotes
Author Disclosure Statement
All authors declared no conflicts of interest associated with this article.
Funding Information
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.