
Abstract
Background:
Anaplastic thyroid cancer (ATC) has poor prognosis with median overall survival (OS) of ∼6 months. We previously reported high PD-1/PDL-1 staining in ATC, raising the possibility of the productive application of the immunotherapeutic pembrolizumab. However, having found pembrolizumab to anecdotally have limited single-agent activity in ATC, we sought to alternatively define whether pembrolizumab might synergistically combine with chemoradiotherapy as initial ATC therapy.
Methods:
An investigator-initiated therapeutic phase 2 trial of pembrolizumab, 200 mg intravenously (IV) every 3 weeks, combined with chemoradiotherapy (docetaxel/doxorubicin, 20 mg/m2 each IV weekly plus volumetric modulated arc therapy) was initiated as frontline therapy (with or without surgery) in ATC to assess efficacy and toxicities. Six-month OS was selected as the primary endpoint using a Simon's optimal design with interim analysis (targeting accrual of 25 patients; Cohort A: prior resection, Cohort B: no resection). Based on a prior patient cohort-treated similarly, but without pembrolizumab, the design was such that, if 6-month true survival is 75%, the probability of declaring the approach worthy of further pursuit would be 91%.
Results:
Three patients were enrolled, two with rapidly enlarging unresectable neck masses. Early tumor responses were favorable in all three, and all three satisfactorily completed: intended radiotherapy, preceding and radiotherapy-concurrent pembrolizumab, and concurrent chemoradiotherapy. However, all three patients died <6 months following therapy initiation—one from pulmonary metastases and two from otherwise unexpected fatal pulmonary complications occurring subsequent to chemoradiotherapy completion—prompting study closure.
Conclusions:
Although initially tolerated and effective in terms of locoregional disease control, disappointing survival outcomes compared with historical controls raise uncertainty that the piloted approach merits further pursuit in ATC.
Introduction
Differentiated thyroid cancer (DTC) is the most common thyroid cancer histology and is increasing in incidence principally due to the more frequent diagnosis of micropapillary thyroid cancer, but mortality remains low (1). However, anaplastic thyroid cancer (ATC), an undifferentiated variety of thyroid cancer, remains a devastating, although rare, malignancy—an oncologic emergency with extremely poor survival (2 –4). Chemoradiotherapy, combined with surgical resection when feasible, has emerged as standard initial therapy for ATC; when this multimodal therapy is applied in ATC, improved survival has been noted by several groups compared with historical approaches (5 –7). Recently, a basket study demonstrated combination of dabrafenib and trametinib to be effective in ATC with the BRAFV600E mutation, and this combination therapy was subsequently Food and Drug Administration approved for locally advanced or metastatic BRAFV600E-positive ATC with no satisfactory locoregional treatment options (8).
At our institution, treatment of ATC usually involves surgical resection when feasible, followed by chemoradiotherapy (volumetric modulated arc radiation therapy [VMAT] administered concurrently with combination chemotherapy). Weekly docetaxel and doxorubicin is our preferred regimen based on prior favorable results indicating improved overall survival (OS) and excellent locoregional disease control (5,9). However, most stage IVB ATC patients ultimately develop distant metastasis; moreover, the prognosis for stage IVC patients is generally dismal despite multimodality therapy (5). Therefore, further innovations to more effectively control micrometastatic and distant disease are needed.
Cancer can evade immune surveillance by reduced expression of unique antigens, downregulation of majar histocompatibility complex class I and II molecules, secretion of immunosuppressive cytokines such as transforming growth factor beta, recruitment of regulatory T cells, and/or overexpression of ligands (e.g., PD-L1) that inhibit host antitumor immunity. Recently, antibodies targeting the PD-1/PD-L1 or PD-L2 pathways including pembrolizumab have shown impressive and durable clinical benefits in melanoma (10), with promising activity emerging in multiple other solid tumors (11,12), associated with well-defined safety established via multiple phase 3 studies.
ATC has a highly immune cell-infiltrated tumor microenvironment, with tumor-associated macrophages predominant (13) and high PD-L1 expression (14,15). ATC is also associated with higher rate of mutations, especially BRAF, TP53, and TERT promoter mutations (16 –18). Furthermore, there is potential for increased expression of novel tumor-associated antigens in response to cytolysis from multimodal therapy, which, when coupled with PD-1 blocking antibodies, may augment antitumor responses. With this rational in mind, a phase 2 study combining pembrolizumab and chemoradiotherapy was initiated with the primary endpoint of OS, and secondary/exploratory endpoints including efficacy of locoregional control and safety.
Materials and Methods
Study design and patient selection
This study (
There were two prespecified patient cohorts: Cohort A, patients with resectable disease, and Cohort B, those with unresectable disease. Patients with residual disease after subtotal resection were eligible for chemoradiotherapy and were enrolled in Cohort B. The study was designed by the first and the last authors (neither received funding related to the trial) and was reviewed by all authors. Merck, Inc., personnel reviewed, approved, and funded the study, supplied pembrolizumab, and had opportunity to review the article—but had no role in study conduct, data collection, analysis, writing, or publication. The Mayo Clinic Institutional Review Board approved the study; the Institutional Data and Safety Monitoring Board (DSMB) along with the study investigators had oversight of the safety of the enrolled subjects.
Treatment
Protocol treatment incorporated pembrolizumab immunotherapy into our core multimodality ATC protocol. For each of the two study cohorts, patients were to receive study drug (pembrolizumab 200 mg intravenously [IV]), ≥3 days before surgical resection (Cohort A) or chemoradiotherapy (Cohort B), then every 3 weeks thereafter until progressive disease, intolerance, or withdrawal of consent. Chemoradiotherapy with docetaxel (20 mg/m2) and doxorubicin (20 mg/m2) would start typically within 2–4 weeks of surgical resection as deemed appropriate by treating providers. In the primary setting, VMAT consisted of 66 Gy administered in 33 fractions over 6.5 weeks to all gross disease in the neck. Elective nodal regions (bilateral levels II–V, VI, and VII) were treated to 59.4 Gy in 33 fractions over 6.5 weeks.
Statistics
This was a two-cohort, open-label phase 2 study with an interim analysis, based on the Simon's optimal design (19) chosen to assess the potential of pembrolizumab in combination with standard chemoradiotherapy to improve OS in comparison to historical cohort, but without pembrolizumab. The primary endpoint was selected as the 6-month OS rate in Cohorts A and B combined, as ATC has dismal prognosis with historical median OS of 6 months. All patients meeting the eligibility criteria and signing consent were to be evaluated for 6-month OS. The trial was designed with a one-sided test to detect a ≥48.5% reduction of OS hazard rate compared with historical median OS of 6 months, favoring the addition of pembrolizumab; this corresponds to a 20% increase in 6-month OS rate, assuming exponential distribution of OS—predicted to yield an 80% chance of detecting that the 6-month OS rate is at least 70% at a one-sided 0.2 significance level. A total sample size of 20, with ≤5 additional patients allowed, enrolled to account for ineligible patients. Secondary endpoints included safety and tolerance of study therapy. All patients who received at least one dose of study drug were included in safety analyses, with data frozen February 13, 2018, when the study was halted due to futility concerns, with all enrolled patients deceased by that time.
Results
Three patients were enrolled, all on Cohort B before the study was closed upon agreement of the study co-investigators and DSMB over concerns of futility due to unexpectedly short survival of all accrued patients. Patient characteristics are shown in Table 1; median age was 56 years; two were female and one was male; all tumors were clinical American Joint Committee Cancer stage IVB at enrollment. Two patients had coexistent papillary thyroid cancer of classical subtype, but none of the three had known history of DTC, neck irradiation, autoimmune thyroid disease, or prior treatment with radioactive iodine. All pathology was confirmed upon central review by a single expert pathologist (M.R.): one was sarcomatoid subtype, one epithelial, and one unspecified.
Patient Characteristics
AJCC, American Joint Committee Cancer; ATC, anaplastic thyroid cancer; ECOG, Eastern Cooperative Oncology Group; DTC, differentiated thyroid cancer
All three patients completed chemoradiotherapy administered along with the investigational agent, pembrolizumab, administered every 3 weeks. Radiation treatment details are summarized in Table 2. No patient required pembrolizumab dosage adjustment. One patient needed dose modification of cytotoxic chemotherapy due to leukopenia, neutropenia, and Clostridium difficile diarrhea. All patients completed intended radiotherapy with a median dose of 66 Gy.
Radiation Treatment Details
Because of a rapidly compromised airway, this patient started with a hypofractionated course of three-dimensional conformal radiotherapy. The patient received 20 Gy in 5 fractions. Once the airway was stabilized, the patient was switched to volumetric modulated arc therapy and received an additional 40 Gy in 20 fractions for a total dose of 60 Gy in 25 fractions.
All patients demonstrated initial therapy-associated reduction in the size of their neck masses (Fig. 1A). As an illustration of the rapid initial locoregional tumor response seen in association with study therapy, Figures 1B and C show representative neck computed tomography (CT) images for patient 1 at the initiation of protocol treatment (Fig. 1B) and 9 days later (Fig. 1C), showing rapid reduction in the size of the neck mass and resolution of tracheal deviation and mucosal edema.
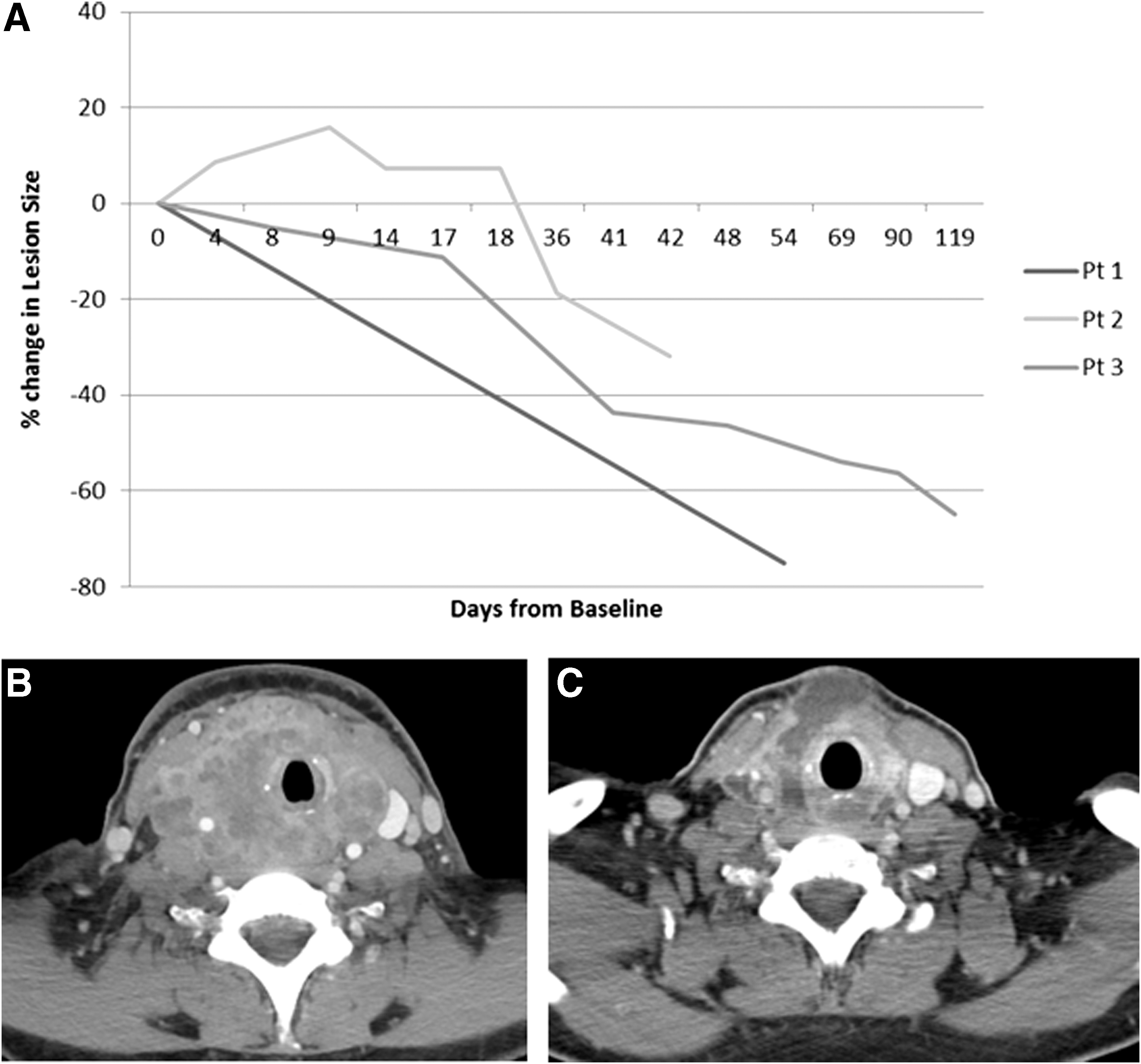
Initial locoregional response to study therapy. (
Patient 1 completed four cycles of pembrolizumab before progressive disease was observed; patients 2 and 3 completed three cycles of pembrolizumab. All patients tolerated study therapy in accord with expectation for patients previously treated in a similar manner but lacking concurrent pembrolizumab immunotherapy. Adverse events possibly, probably, or definitely related to pembrolizumab are noted in Table 3.
Adverse Events Related to Pembrolizumab
AE, adverse event.
Despite initially favorable locoregional tumor response to study therapy (Fig. 1), all patients died <6 months after study therapy initiation: patient 1 from distant metastatic disease, patient 2 of pneumonitis/pneumonia, and patient 3 of pneumonia. The median OS was 2.76 months. All three deaths occurred sooner than observed among our historical cohort of stage IVB patients (Fig. 2), leading the study investigators to halt accrual and to ultimately close the trial in consultation with the DSMB. Patients 1, 2, and 3, respectively, received a mean total lung dose of 9.91, 9.66, and 11.05 Gy. The mid-thoracic coronal images of radiotherapy dosimetry and dose volume histograms are depicted in Figure 3. Somatic analysis of patients tumors also showed usual mutations associated with ATC; patient 1 had an NRAS (Q61R) mutation and patient 3 had a BRAFV600E and a TERT promoter mutation (124C>T).
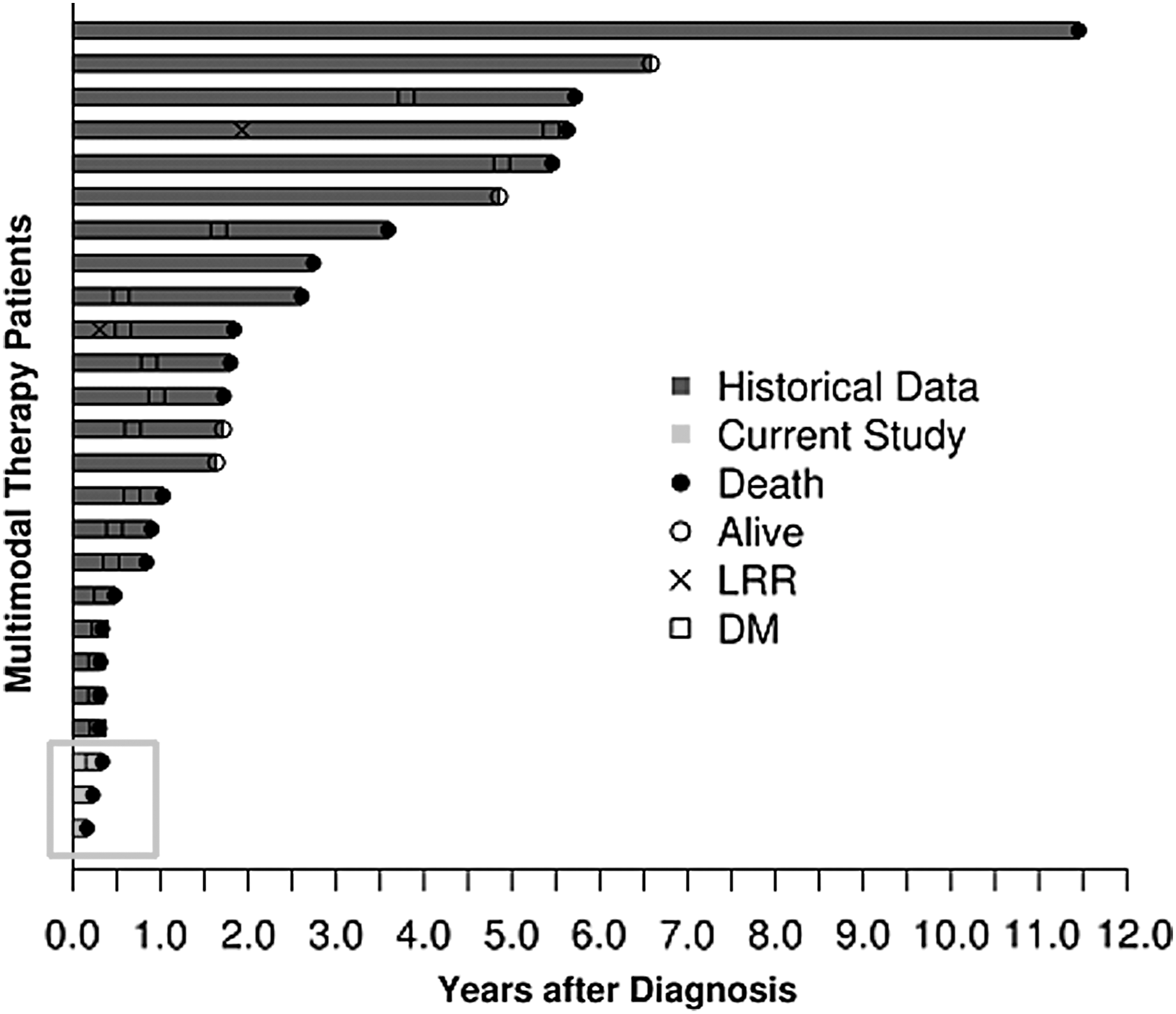
Swimmer plot demonstrating the outcome in recent cohort of anaplastic thyroid cancer patients (American Joint Committee Cancer stage IVB only) compared with the patients treated on MC1679. DM, distant metastasis; LRR, loco-regional recurrence.
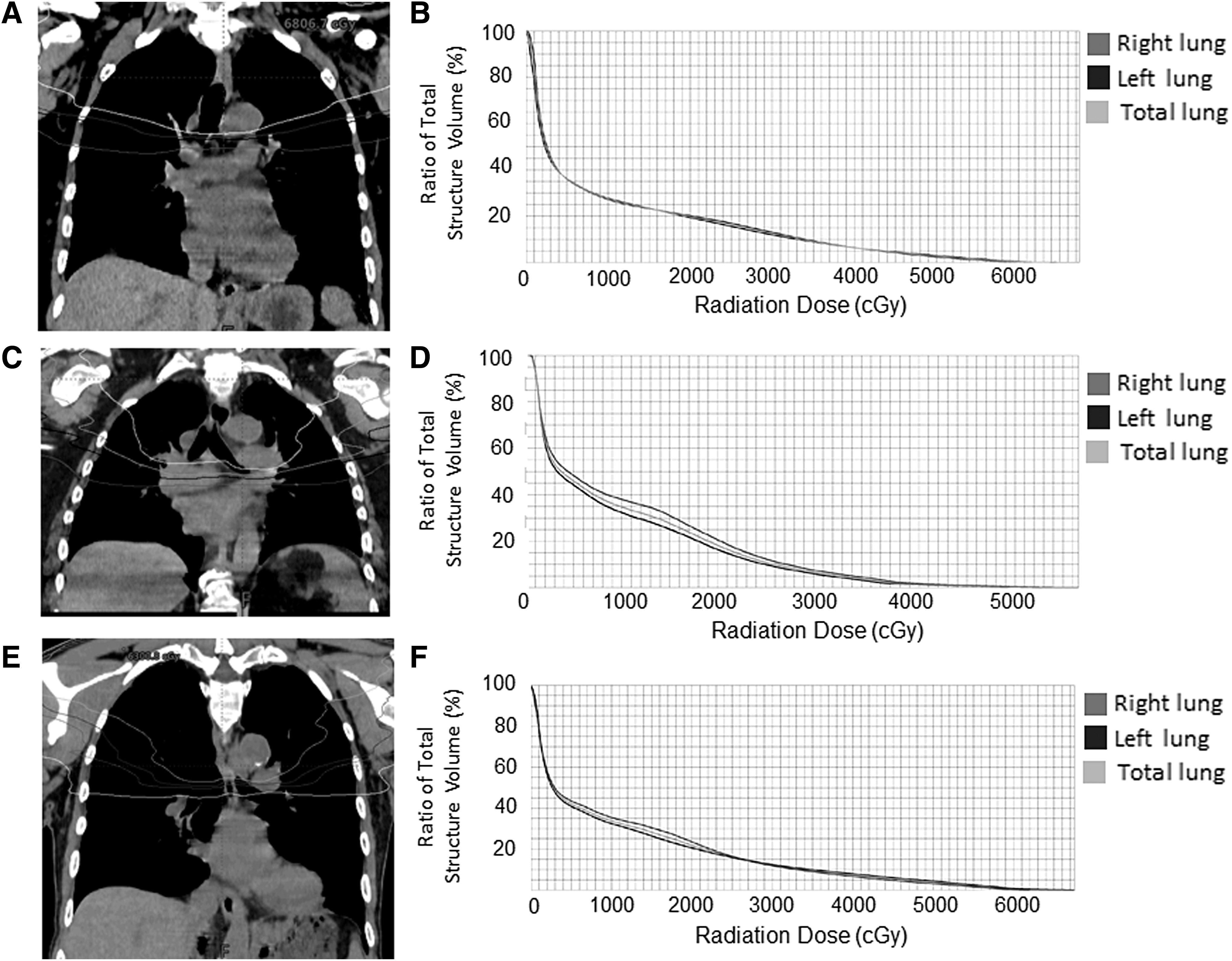
Mid-thoracic coronal images for radiotherapy dosimetry (5, 10, 20, and 30 Gy isodose lines) are shown for patients 1, 2, and 3 (
Patient synopses
Patient 1 was a 56-year-old female presenting with a large neck mass of 1–2 months duration associated with pain referred to her ears; biopsy revealed an undifferentiated carcinoma consistent with ATC, and it was deemed unresectable. After detailed discussions, patient 1 elected protocol treatment, initiating radiotherapy 3 days after pembrolizumab. Two days later, she presented to the emergency department with nausea, vomiting, stridor, and laryngeal edema. A CT scan of neck demonstrated mucosal edema in the hypopharynx and supraglottic airway. She was admitted to the intensive care unit, IV dexamethasone was initiated, and chemoradiotherapy was continued. A rapid improvement in symptoms and improvement in the size of the mass and laryngeal edema was demonstrated by CT. The patient was discharged 7 days later, and she completed cycles 2 and 3 of pembrolizumab. Chemoradiotherapy, however, was complicated by brief neutropenic fever, but she required no dose modifications; she received a total of 66 Gy. Interim imaging later demonstrated a subcentimeter lung nodule that did not meet criteria for progressive disease by RECIST 1.1, and pembrolizumab cycle 4 was administered. Three week later, however, imaging revealed diffuse progressive disease in the lungs in the absence of neck progression and she was taken off the study.
Lenvatinib at 24 mg/day was initiated as salvage therapy, complicated by fatigue and hypertension. One week later, the patient was admitted to the local hospital for dyspnea; chest CT demonstrated progressive lung metastases; she died 1 week later.
Patient 2 was a 55-year-old female who underwent surgical resection for a presumed DTC at an outside institution. Postsurgical recovery was complicated by a rapidly enlarging neck mass; review at our institution about a month later revealed this to be a spindle cell ATC; there were three foci of coexistent papillary thyroid carcinoma.
On our initial evaluation, she had a large neck mass, stridor, and associated right vocal cord palsy. A positron emission tomography-CT scan demonstrated a large right thyroid bed mass extending from the right oropharynx to the thoracic inlet and crossing the midline associated with airway narrowing. Subcentimeter lung nodules were seen, but they were stable in size compared with a CT obtained 1 month previously, and they were non-fluorodeoxy glucose avid; no other distant metastases were discovered.
The tumor was deemed unresectable, and the patient elected study treatment, initiating pembrolizumab the next day. One day later, the patient presented with worsening dyspnea and was hospitalized, initiating chemotherapy, but her dyspnea and stridor continued to worsen. The following day she underwent bridging nasotracheal intubation and she initiated radiotherapy the next day. Hospitalization was complicated by a C. difficile infection and leukopenia. Chemotherapy doses were reduced by 25% per protocol. Her neck mass responded well to the treatment thereafter and she was extubated 2 weeks later, receiving a second dose of pembrolizumab 3 days later; she thereafter completed chemoradiotherapy without additional acute events, receiving 60 Gy delivered to her neck and thyroid bed.
Patient 2 was admitted to an outside institution 2 weeks later with somnolence, weakness, dyspnea, diarrhea, fever, radiation dermatitis involving her neck, mucositis, dehydration, hyperglycemia, and hypoxic respiratory failure. A chest X-ray showed bilateral lung infiltrates. Supportive care, including IV fluids, steroids, and antibiotics, was initiated; blood and urine cultures grew Enterobacter. Three days later, she was intubated and mechanically ventilated as respiratory failure worsened; recurrent C. difficile diarrhea was treated with oral vancomycin. She briefly improved but continued to be critically ill. Repeat CT neck showed continued regression of the tumor, but a CT showed bilateral infiltrates. She was again intubated; bronchoalveolar lavage showed purulent secretions and grew penicillin-resistant Moraxella; comfort measures were elected and the patient died in the hospital.
Patient 3 was a 76-year-old male who underwent surgical resection of ATC with coexistent DTC. He was seen at our institution 5 weeks later and had residual/recurrent disease in the neck. Standard chemoradiotherapy versus treatment on the current protocol was discussed, and he elected treatment per protocol and initiated pembrolizumab 1 week later and chemoradiotherapy shortly thereafter. The therapy was complicated by failure to thrive. Hospitalization and placement of a feeding tube allowed treatment, and he completed three cycles of pembrolizumab and chemoradiotherapy to a total of 66 Gy; no chemotherapy dose adjustments were needed.
Patient 3 was admitted to his local hospital 10 days later with rapidly progressing fatigue, diarrhea, and dyspnea, requiring transport via ambulance. He denied chest pain, fevers, and chills, but he was hypoxemic and required endotracheal intubation and mechanical ventilation. He was found to be in septic shock. A CT of the chest showed predominantly left-sided consolidation/pneumonia and blood cultures grew methicillin-sensitive Staphylococcus aureus. Despite intensive supportive care, the patient died 2 days later.
Discussion
ATC is a devastating disease with high mortality. Chemoradiotherapy combined with surgery (when feasible) as an initial therapeutic approach in nonmetastatic ATC has, however, been associated with improved survival (3 –5). Nevertheless, most ATC patients still succumb to distant metastases. The present trial was configured as an attempt to build upon prior gains in terms of improved outcomes achieved in response to chemoradiotherapy by superimposing pembrolizumab immunotherapy.
All three accrued trial patients completed intended therapy and recovered sufficiently to return to their homes for further convalescence, but their outcomes were highly discouraging. In ATC, however, the therapies applied, and the disease itself, are highly toxic; this is the nature of ATC and of ATC therapy. Whether our negative experience with pembrolizumab plus chemoradiotherapy reflects an improbable negative random outcome, or instead actual augmented toxicities from the combination in ATC, remains unknown based on available sparse data. Recently, a case where adjuvant radiotherapy concurrent with cisplatin and immunotherapy was successfully completed without any complication has been published (20).
The possibility of augmented combined toxicity of pembrolizumab plus chemotherapy is very important to consider, as is the alternatively possibility of combined toxic effects of pembrolizumab plus neck/chest/mediastinal radiotherapy. These questions and alteration from the current study design must be critically considered in the development in any further trials of combination therapies in the primary/initial treatment of nonmetastatic ATC.
There are many data to indicate that pembrolizumab can be safely combined with most chemotherapy regimens, studied in prior phase 1 trials (21), wherein no unanticipated therapy-related complications were attributed to chemotherapy plus pembrolizumab regimens. In oncology practice, we and most other groups now have thus become very comfortable combining pembrolizumab with most any chemotherapy regimen. Pembrolizumab plus taxane regimens have proven safe and are approved in lung cancer, as has pembrolizumab plus doxorubicin (21). Hence, there are convincing data that chemotherapy plus pembrolizumab produce no clear augmented, only additive, toxicities.
Alternatively, whether the addition of pembrolizumab to chemoradiotherapy in ATC may be prohibitively toxic remains unanswered. Pulmonary immunological toxicities of immunotherapy/pembrolizumab can be considerable but have been observed in <10% of checkpoint inhibitor only-treated patients (22), making it seem unlikely that the two trial patients with lung events associated with their deaths in our study are purely immunological lung injury events; moreover, one of the two patients had unilateral lung changes, an unlikely cause of pure immunological toxicity. In lung carcinoma treated with chemoradiotherapy, consolidation therapy with PD-L1 inhibitors in the PACIFIC study demonstrated a combined incidence of pneumonitis and radiation pneumonitis greater than placebo (33.9% vs. 24.8%, respectively), but grade 3 or 4 toxicities occurred only in 3.4% and 2.6%, respectively (23). On the contrary, data from early head and neck squamous cell carcinoma studies combining PD-1 inhibitors with surgery or radiotherapy have demonstrated no apparent increased risk of adverse events (24,25). A recent abstract also demonstrated safety of single-agent anti-PD-1 therapy in ATC in the absence of chemoradiotherapy (26).
We are thus prompted to consider why there might be augmented toxicities from chemoradiotherapy in ATC. In pursuit of this possibility, we noted that a review of the lung radiation dosages received by our three ATC patients compared with a series of our head and neck cases was enlightening, as ATC patients received over twice the lung radiation doses. In particular, the mean lung activities for patients 1, 2, and 3 were 9.91, 9.66, and 11.05 Gy, respectively, whereas the corresponding mean lung dose for 50 randomly selected patients with laryngeal or hypopharyngeal squamous cell carcinoma at our institution was much lower at 4.17 Gy (range 1.51–10.16 Gy). It is therefore possible that the two lung event-associated deaths in our study might be attributable in part to the greater lung radiation doses administered concurrently with immunotherapy. Nevertheless, we would not have anticipated fatal radiation pneumonitis within 2 weeks of completing treatment with a mean lung dose of 10 Gy and V20Gy of 20%.
There is little doubt that ATC chemoradiotherapy is perhaps the most toxic of all combination therapies that can be reasonably administered. Further therapeutic additions therefore might not be possible to this particular chemoradiotherapy protocol. However, given that the survival is extremely poor in ATC, and immunotherapy alone has shown some promising results in recurrent and metastatic ATC (26), we do not believe that further development of pembrolizumab or other immunotherapeutic strategies in ATC should cease. Clearly, additional studies are required to best define how to apply checkpoint inhibitors in ATC.
Footnotes
Acknowledgments
The authors sincerely thank our patients and their families for their unrelenting commitment to their care, to advancing therapies in ATC, and for participating in the study. We also thank Ms. Bobbi Jebens for editorial assistance, and the Mayo Clinic DSMB for their input and assistance.
Author Disclosure Statement
The authors have no competing financial disclosures.
Funding Information
This study was sponsored by Merck, Inc., personnel reviewed, approved, and funded the study, supplied pembrolizumab, and had opportunity to review the article but had no role in study conduct, data collection, analysis, writing, or publication.