
Abstract
Background:
Nondiagnostic results are common following fine-needle aspiration biopsy (FNAB) of thyroid nodules, but recommendations for the management of these patients vary. We sought to determine the outcomes and predictors of nondiagnostic FNABs in a single-center cohort of patients undergoing thyroid nodule evaluation.
Methodology:
We identified all first time ultrasound-guided FNABs performed between May 2007 and June 2013 at the Beth Israel Deaconess Medical Center Thyroid Nodule Clinic and examined demographic data, follow-up ultrasounds, repeated FNABs, and histopathologic findings. We examined the likelihood of diagnostic findings and of cancer with increasing numbers of nondiagnostic evaluations with their exact binomial confidence intervals [CIs] and potential predictors of nondiagnostic status using generalized estimating equations.
Results:
During the six-year period, 2234 unique individuals underwent ultrasound-guided FNAB of a thyroid nodule. The probability of obtaining a diagnostic biopsy declined from 84.4% [95% CI 82.8–85.8%] for initial FNABs to 57.6% [CI 50.8–64.2%] for the first re-FNAB and further to 42.4% [CI 25.5–60.8%] for second re-FNABs. Adjusted risk of nondiagnostic FNAB strongly increased with increasing numbers of previous biopsies and was also higher among whites. The overall rate of diagnosis of malignancy after a nondiagnostic FNAB was 8.1% [CI 4.2–13.7%] and was similar regardless of the number of previous nondiagnostic aspirations.
Conclusion:
Following an initial nondiagnostic FNAB, the probability of yielding a diagnostic result declines with each sequential repeat FNAB. Nonetheless, a tangible possibility of malignancy remains even after repeated nondiagnostic FNABs.
Introduction
Thyroid nodules are commonly encountered in the ambulatory setting. Ultrasonography can detect nodules in as many as 35–68% of asymptomatic patients (1 –3). Nodular thyroid disease is more common in women and with increasing age (1,2). Thyroid nodules are typically benign, but up to 15% are malignant (4,5) representing a serious diagnostic challenge to internists, endocrinologists, and radiologists.
Although guidelines recommend ultrasonography as an initial step in thyroid nodule evaluation, in part because of its ease, availability, and cost, a major pitfall remains its inability to differentiate benign from malignant nodules definitively. Fortunately, ultrasound-guided fine-needle aspiration biopsy (FNAB) has proven to be a cost-effective, minimally invasive, and accurate means of evaluating the risk of malignancy in thyroid nodules (6,7). Nonetheless, 2–24% of FNABs provide nondiagnostic results, and management of thyroid nodules with a nondiagnostic FNAB remains a vexing clinical challenge (8). The risk of malignancy in nondiagnostic FNABs has been reported to be 1–4%, yet, of those eventually surgically resected, ∼10–20% of these nodules eventually prove to be malignant when subjected to surgical resection (8,9). Limitations of FNAB include variability in the skill of the aspirator, threshold for determination of adequacy of specimen by the cytologist, and the number and areas of the nodule sampled (10 –13). FNABs performed on more cystic nodules and smaller nodules increase inadequacy rates even further (14,15).
Current guidelines recommend that initial nondiagnostic cytology should be followed by repeat ultrasound-guided FNAB (13,16). Subsequent nondiagnostic FNABs can be managed by surgery for histopathologic diagnosis or close observation, depending on clinical risk factors and sonographic patterns (16). However, limited real-world evidence exists to inform management of nondiagnostic FNABs, despite their prevalence.
To address this lack of evidence, we sought to describe the clinical outcomes in a large retrospective cohort study of patients with initially nondiagnostic FNAB. We sought to establish the likelihood of diagnostic findings after initial and repeated nondiagnostic aspirations, the ultimate likelihood of cancer in these scenarios, and the determinants of nondiagnostic findings for any given FNAB.
Methods
Patient population
This study received institutional review board (IRB) approval, delegated from the Beth Israel Deaconess Medical Center (BIDMC) to the Dana Farber Cancer Institute IRB. The requirement for informed consent for this retrospective cohort study was waived.
As previously described (17), the BIDMC Thyroid Nodule Clinic (TNC) is staffed by a multidisciplinary team of physicians. An endocrinologist or endocrine surgeon with thyroid expertise consults on each patient and refers to either a board-certified radiologist with more than 25 years of experience in performing ultrasound-guided FNABs or an endocrinologist with at least 3 years of experience performing ultrasound-guided FNABs, who then performs ultrasonography and ultrasound-guided FNABs of appropriately selected nodules. All endocrinologists are certified in the Endocrine Certification in Neck Ultrasound (ECNU) program and perform at least 50 FNABs annually.
A cytopathology fellow is present in approximately half of the sessions to provide rapid on-site determination of specimen adequacy including in cases where there is a previous nondiagnostic FNAB. Patients may also undergo FNAB upon direct referral from general endocrinology or endocrine surgery clinics. In all cases, an ongoing quality improvement system tracks outcomes of all patients undergoing FNAB.
We identified all first FNABs that were performed between May 2007 and June 2013 in the TNC. FNAB results were classified based on the Bethesda criteria and American Thyroid Association (ATA) guidelines as diagnostic or nondiagnostic. We followed those patients with an initial nondiagnostic finding to determine whether they underwent a repeat FNAB, clinical follow-up, surgery, or were lost to follow-up (defined as no follow-up in the BIDMC). (Supplementary Table S2). We repeated this process for each successive FNAB, identifying those with a nondiagnostic FNAB and following their outcomes forward (Fig. 1). This was continued through all FNABs until no further follow-up was recommended (e.g., benign finding); patient had surgery with subsequent pathology results; or patients were lost to follow-up (i.e., did not return to the BIDMC through March 2019).
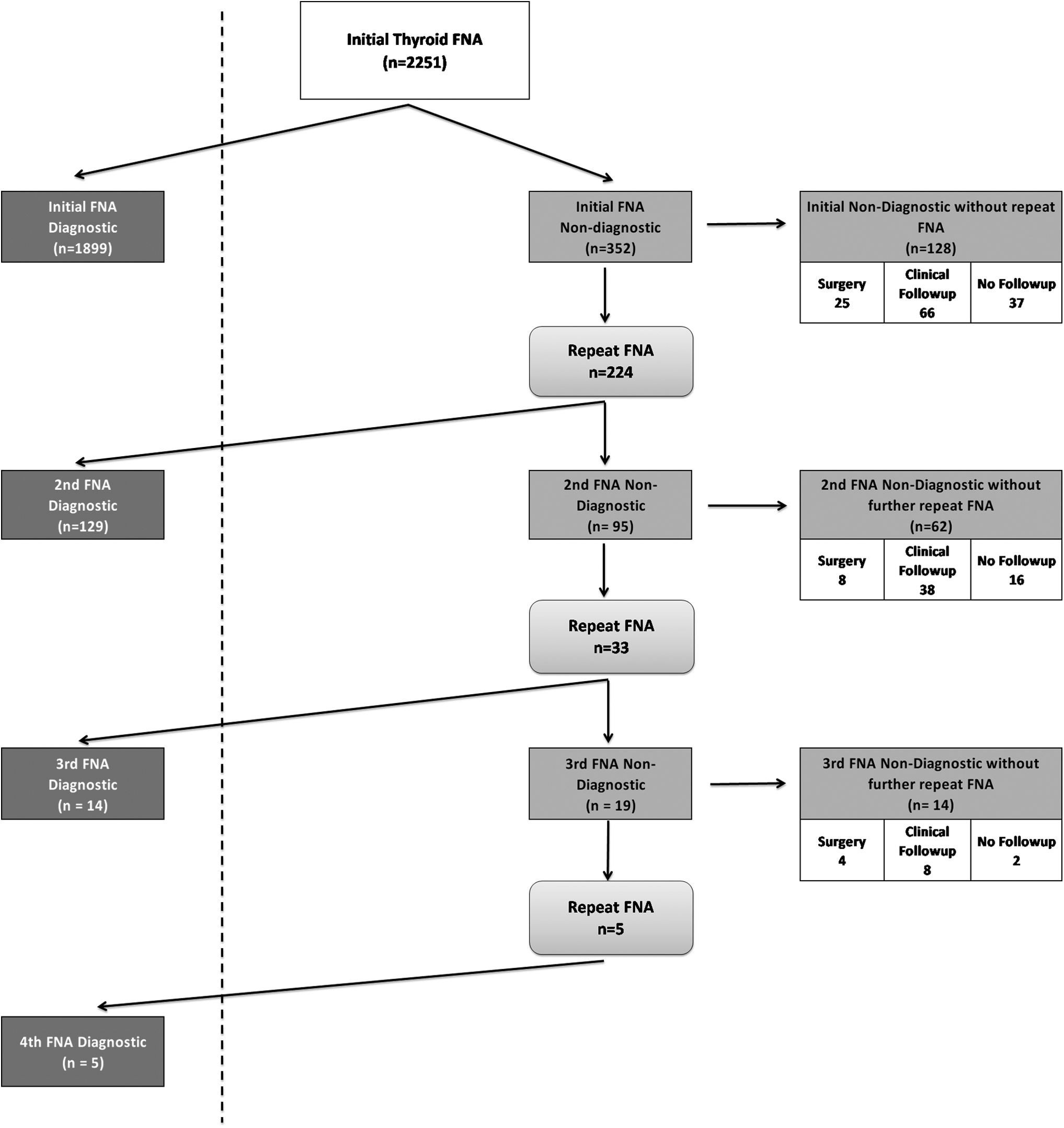
FNA findings and follow-up results flowchart. For the purposes of this study—once a patient had a diagnostic finding, they were not followed further. FNA, fine-needle aspiration.
Covariates and outcomes
All information was abstracted from the electronic medical record including age, sex, and race/ethnicity. Additional clinical data abstracted included results of all follow-up ultrasounds, FNABs, and surgical interventions and the histopathologic findings of the nodule(s). An independent reviewer unaffiliated with the clinical practice reviewed all electronic medical records. We also conducted additional manual review through appointment logs to confirm loss to follow-up.
Statistical analysis
We report prevalence estimates for diagnostic findings and malignancy with their exact 95% confidence intervals [CIs] using the Clopper–Pearson method. To evaluate demographic predictors of nondiagnostic status, we used all available biopsies and constructed generalized estimating equations to account for repeated biopsies within person. In these models, we derived relative risks for nondiagnostic biopsy status using a Poisson outcome, log link, and exchangeable correlation matrix (18). To address the possibility that malignancy rates may have differed among patients with and without extended follow-up, we performed a series of sensitivity analyses. First, we imputed rates of malignancy among those without follow-up using two extremes—either assuming that no malignancies occurred or that the rate of malignancy was equal to the upper 95% confidence bound of the proportion among those with an initially diagnostic fine-needle aspiration (FNA). Second, we fitted a logistic regression model, estimating the likelihood of lack of follow-up as a function of other covariates, and outputted the predicted values for each patient. We then created stabilized inverse probability weights, applied these to recreate the original sample size, and estimated the likelihood of malignancy in the resulting pseudo-population of patients who had complete follow-up (19).
Results
Study population
From 2007 to 2013, 2234 patients underwent an initial ultrasound-guided biopsy of 2251 thyroid nodules (Fig. 1). Demographic characteristics of these patients are shown in Table 1. As expected, the population largely consisted of middle-aged women, but the racial and ethnic composition was diverse.
Demographic Characteristics of the Study Population at Initial Biopsy
Likelihood of nondiagnostic FNAB
A total of 352 initial biopsies yielded nondiagnostic results (Fig. 1 and Supplementary Table S2). Among these 352 patients with an initial nondiagnostic FNAB, 224 underwent a repeat FNAB and 33 patients with a nondiagnostic evaluation at the repeat ultimately underwent a third. As outlined in Table 2, the probability of obtaining a diagnostic biopsy declined progressively from 84.4% for initial FNABs to 42.4% for the third biopsy.
Probability of Obtaining a Diagnostic Biopsy at the Initial Biopsy or After Previous Nondiagnostic Fine-Needle Aspiration Biopsy
CI, confidence interval; FNAB, fine-needle aspiration biopsy.
We examined determinants of nondiagnostic findings among all 2516 biopsies (representing the initial biopsies of 2251 nodules and repeat biopsies in the 352 nodules that were initially nondiagnostic), including age, sex, race/ethnicity, and the number of previous biopsies. We observed no associations with age (p = 0.19) or sex (p = 0.86). Race/ethnicity was strongly associated with nondiagnostic status (p = <0.001); compared with whites, the likelihood of a nondiagnostic biopsy was lower among Latinos (adjusted relative risk 0.84 [CI 0.76–0.93]). African Americans, Asians, and those of other or mixed race/ethnicity were similar to whites. Compared with the initial biopsy, the likelihood of nondiagnostic findings also increased progressively and significantly with each succeeding biopsy, with adjusted relative risks of 5.78 [CI 5.09–6.56] for the second biopsy and 9.83 [CI 8.56–11.28] for the third biopsy (p for all comparisons <0.001).
Likelihood of malignancy
Among all 2251 thyroid nodules biopsied, 285 were found to have a malignancy (12.7% [CI 11.3–14.1%]). Two hundred seventy-four were identified as papillary cancer, 6 as follicular cancer, 3 as medullary cancer, and 2 unknown (pathology unconfirmed as surgeries were performed at outside hospitals).
Of the 352 patients with an initial nondiagnostic FNA findings, 26 patients (7.4% [CI 4.9–10.6%]) were ultimately found to have thyroid cancer, all of whom had surgery and papillary histopathology. The overall course and malignancy rate after a nondiagnostic FNAB is shown in Table 3.
Malignant Findings Among Patients with a Nondiagnostic FNAB According to the Number of Repeat Nondiagnostic FNABs Following an Initial Nondiagnostic FNAB
Reasons for surgery for patients with nondiagnostic FNAs
Of 37 patients who ultimately underwent surgery for definitive diagnosis of their nodules, patient preference (n = 10) and diagnostic FNA in a different nodule (n = 9) were the most prevalent reasons for patients being referred for surgery. Other reasons included compressive symptoms, increasing growth of thyroid nodule, ultrasound characteristics, and physician recommendation (Table 4).
Indications for Surgery in Patients Who Underwent Surgical Treatment of Thyroid Nodules
FNA, fine-needle aspiration.
Sensitivity analyses for malignancy rates
To examine the robustness of our analyses of malignancy rates to assumptions about follow-up, we performed two sets of analyses. First, we imputed the likelihood of malignancy among those without follow-up using extreme assumptions. As shown in Supplementary Table S1, the imputed rates (5.9–8.9% for the total cohort of 352) fall well within the original confidence intervals. Second, we estimated the likelihood of malignancy accounting for missingness using inverse probability weights. The likelihood of malignancy in this analysis was 8.3% [CI 5.4–11.1%], again similar to the original estimate.
Discussion
In this retrospective, pragmatic cohort study that included more than 2500 thyroid biopsies, the likelihood of nondiagnostic findings on initial biopsy was ∼15%. This proportion rose steadily with successive biopsies of the same nodule, suggesting that diagnostic yield may be asymptotic and hence that the risk from continued biopsies may eventually exceed the benefit, although the threshold appears to be above three nondiagnostic results. This observation must be balanced by the corresponding recognition that cases of thyroid cancer continued to be identified at an ∼8% rate, even among patients who had received repeatedly nondiagnostic biopsy results. Thus, even repeated nondiagnostic findings cannot be considered entirely benign.
Our results provide insight into the most recent ATA clinical practice guidelines (16). These guidelines recommend that nondiagnostic FNABs undergo a repeat FNAB under ultrasound guidance and if available, on-site cytologic evaluation.
Surgical management of nondiagnostic FNAB can be considered in the presence of suspicious ultrasound characteristics (such as microcalcifications, irregular margins, a taller than wide shape, or hypoechogenicity), growth of the nodule (defined as >20% in two dimensions), or concerning clinical factors such as radiation exposure or family history of thyroid cancer (16). Nodules causing neck compressive symptoms such as dysphonia, dysphagia, or orthopnea may warrant surgical evaluation (20). In clinical practice, thyroid surgery may also be considered based on patient preference (i.e., anxiety of nodule presence or cosmetic considerations). In our study, patient preference and cytopathology/lesion in another nodule were the predominant reasons why patients were referred for surgical management. Other factors that guided surgical management included neck compressive symptoms, increased growth in nodule size, ultrasound characteristics, and physician recommendation.
The guidelines also state that “repeatedly” nondiagnostic nodules without a high suspicion sonographic pattern should undergo either close observation or surgical excision for definitive diagnosis.
Our results support re-biopsy after an initially nondiagnostic result, for which we documented a satisfactory diagnostic yield for a second biopsy. Our results also support the inference that continued re-biopsies are apt to be of incrementally lower value, making surgery a more attractive option if diagnostic results are needed. Given the low but tangible rate of malignancy even among those with repeatedly nondiagnostic results, a strategy of close observation appears reasonable.
Our results, which derive from a single large thyroid center, are generally consistent with previous studies. Rates of nondiagnostic FNABs in the literature generally match those noted here (8,9,21,22). The malignancy rates we observed also tend to agree with a previous meta-analysis (23) but were substantially higher than the 2–4% predicted by the authors of the Bethesda report (13). Although some authors have used the lower rates proposed in the Bethesda report to suggest that ultrasound follow-up alone would be most appropriate in these patients (22,24), our results suggest that there is clinical value in attempting to obtain a diagnostic result.
Even though a second FNAB is less likely to result in a diagnostic specimen, the nearly 58% likelihood of obtaining a diagnosis to help guide clinical decision-making is not inconsequential. The finding that a third FNAB will also yield useful information in more than 40% of cases supports this approach to nodules lacking particularly high-risk sonographic or clinical features, where surgical intervention would presumably be in the patient's best interest. Suspicious sonographic features and the Thyroid Imaging Reporting and Data Systems score have been proposed for this purpose (25 –27). Despite the declining yield from repeated biopsies when previous results have been nondiagnostic, we could not identify a clear limit above which further FNAB would be fruitless, in part reflecting the limited number of patients who underwent a fourth FNAB. Additional studies that follow patients who undergo more FNAB attempts, ideally as part of a prospective research protocol, will be needed to clarify the yield curve in this setting.
Our study is subjected to important limitations. Our results reflect a large sample of patients in real-world conditions and hence are more generalizable than those reported from specialized protocols, but they therefore include inevitable clinical heterogeneity. For example, FNABs were performed by experienced clinicians but biopsy techniques were not standardized, and decisions to undergo FNAB or surgery were made clinically and in deference to patient wishes.
The use of cytologists to perform on-site specimen adequacy appears to improve diagnostic rate, although its benefit is highest when adequacy rates are low (28,29). Nonetheless, concerns exist regarding the significant expense in cytologists' time and resulting cost-effectiveness (30). At our institution, rapid on-site adequacy assessment occurs under special circumstances such as in previously nondiagnostic FNABs. Most samples were collected directly in Cytolyt® solution for THINPREP® monolayered slides, and hence, our diagnostic yields might differ from clinics with consistent on-site cytopathology. The impact of rapid on-site evaluation for specimen accuracy was not assessed in our study but would be an important consideration for future study. Loss to follow-up also reflected in real-world realities; some 25–30% of patients did not return after each nondiagnostic FNAB. Due to the retrospective nature of the study, we could not determine the reasons for loss to follow-up, but likely reflects the unique dynamics of the local insurance market and medical community, including a plethora of well-known, accomplished endocrine units. Our sensitivity analyses provide some reassurance that this did not markedly bias our estimates of malignancy. We did not collect sonographic features as part of this quality initiative, and additional studies are needed to determine if specific characteristics might identify patients with nondiagnostic FNABs who are most likely to require surgery for a diagnostic result, thereby reducing the time to a definitive outcome. In addition, the association between race/ethnicity and nondiagnostic FNAB is interesting, but further studies would be required to understand this and any potential correlation with parameters such as body mass index or nodule size.
In conclusion, in this retrospective, real-world cohort of more than 2500 thyroid biopsies, the initial rate of nondiagnostic findings approximated 15%, but this rate climbed with each subsequent FNAB. Nonetheless, we did not observe a zero-yield threshold even with up to four FNABs. At the same time, the risk of malignancy remained low but measurable and minimally altered even after three nondiagnostic findings. Together, these results suggest that continued efforts to obtain diagnostic pathology appear to be warranted in many cases, but with the recognition that continued FNAB alone is increasingly unlikely to produce that result with persistently nondiagnostic findings. Additional large series are still needed to confirm our findings and to inform clearer guidelines for this common but vexing problem.
Footnotes
Acknowledgment
We would like to thank Fred Milgrim for his assistance in the case review and the original data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received to achieve this work.
Supplementary Material
Supplementary Table S1
Supplementary Table S2