
Abstract
Background:
Incidental finding of differentiated thyroid microcarcinomas (DTMc) in patients undergoing thyroid surgery for benign indications has become increasingly common. Even though carcinogenesis might relate to the background disease of the gland, the incidence of DTMc in the setting of various thyroid disorders remains unclear. We designed the present study to address this question.
Materials and Methods:
We reviewed data from two prospectively collected databases of consecutive patients undergoing thyroid surgery in two high-volume tertiary care referral centers, one in the United States (A) and the other one in Greece (B) over 18 years. We collected data on the preoperative surgical indication, fine-needle aspiration (FNA) cytology, and surgical pathology. We excluded subjects operated for thyroid cancer or with high risk for malignancy (FNA suspicious for thyroid cancer, follicular neoplasm, suspicious for follicular neoplasm, follicular lesion of undetermined significance/atypia of undetermined significance, or preoperative features of malignancy) and those with postsurgical pathology consistent with papillary thyroid cancer (PTC) ≥1 cm in largest diameter. We divided our subjects based on pathology data into those with chronic lymphocytic thyroiditis (CLT), Graves' disease (GD), or multinodular goiter (MNG).
Results:
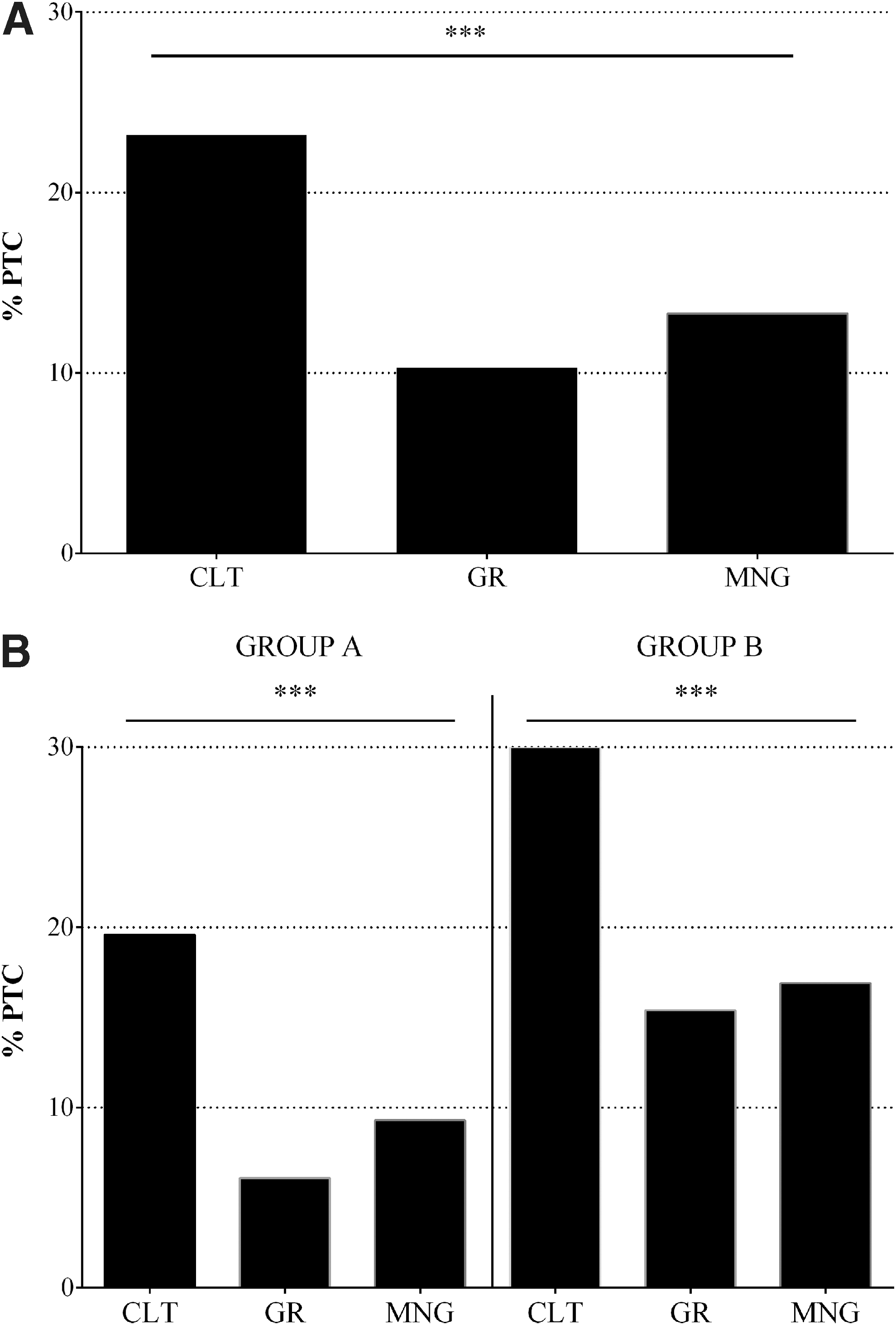
We reviewed 6096 cases of thyroid surgery (A: 2711, B: 3385). We included 3909 subjects in the analysis. Overall, 569 (14.6%) PTC subjects were identified (A: 221/2003 [11%], B: 348/1906 [18.3%], odds ratios [OR] = 0.56, p < 0.0001). CLT was present in 617 subjects; PTC sonographic was present in 143 subjects (23.2%) (A: 79/404 [19.6%], B: 64/213 [30%], OR = 0.56, p = 0.003). GD was present in 359 subjects; PTC was present in 37 subjects (10.3%) (A: 12/197 [6.1%], B: 25/162 [15.4%], OR = 0.36, p = 0.004). MNG was present in 2933 subjects; PTC was present in 389 subjects (13.3%) (A: 130/1402 [9.3%], B: 259/1531 [16.9%], OR = 0.50, p < 0.0001). The incidence of PTC was significantly higher in CLT compared with MNG (OR = 1.75, p < 0.0001) or GD (OR = 2.25, p < 0.0001) but not in MNG compared with GD (OR = 1.29, p > 0.05).
Conclusions:
Incidentally discovered PTC are more commonly identified in surgical specimens from subjects with CLT compared with patients with MNG, while patients with GD present with a lower incidence compared with both groups. These data support previously published findings that euthyroid Hashimoto thyroiditis favors carcinogenesis, while GD may have a protective role.
Introduction
The incidence of differentiated thyroid cancer (DTC) has significantly increased over the past 40 years (1). Papillary thyroid microcarcinomas (PTMc) are tumors of papillary histological subtype (papillary thyroid cancer [PTC]) with a maximal diameter ≤1 cm. They have the most rapidly increasing incidence in post-thyroidectomy pathology specimens among all thyroid tumors (1). When these tumors are identified during unrelated head and neck imaging (2), or during a detailed histopathology examination following a thyroidectomy performed for reasons not pertaining to malignancies of the thyroid gland, they are termed incidental (3). The majority of differentiated thyroid microcarcinomas (DTMc) are PTMc cases (3). In recent years, a concurrent rise in the incidence of autoimmune thyroid diseases (AITDs) has been noted, with chronic lymphocytic thyroiditis (CLT) being the most common (4). Autoimmunity is a form of inflammation known to promote carcinogenesis in many organs (5); therefore, investigating its role in the rising incidence of PTC is worthwhile.
Studying the association of thyroid cancer and autoimmunity can generate a selection bias. Thyroid cancers are usually diagnosed by fine-needle aspiration (FNA) and then operated on. Incidentally discovered PTMc are thyroid cancers found by chance in thyroids operated on for other reasons than cancer. Therefore, comparison of their association with CLT, Graves' disease (GD), or non-autoimmune thyroid diseases (non-AITDs) could shed unbiased light on their pathogenesis. This type of analysis has not been performed to date. Therefore, we designed the present study to address these relationships to investigate if they are random or not.
Materials and Methods
All patients referred for thyroid surgery in two high-volume tertiary care referral centers, one in the United States and the other one in Greece (Center A and B, respectively, as per authors' affiliation), were enrolled in a prospective registry. As part of the research protocol, we collected clinical, laboratory, imaging, cytological and histological data. For the present study, data from all patients operated during 18 consecutive years, regarding their preoperative surgical indications, the FNA cytology, and the surgical pathology results, were reviewed.
The goal was to identify patients who were not operated for thyroid cancer, so that true incidental microcarcinomas incidence could be analyzed. Therefore, we excluded subjects with a preoperative diagnosis of a thyroid cancer of any histological type, those with cytological diagnoses associated with a high risk for malignancy (suspicious for thyroid cancer, follicular neoplasm, suspicious for follicular neoplasm, follicular lesion of undetermined significance [FLUS], or atypia of undetermined significance [AUS]), those with nodules with sonographic features suggestive of malignancy (TIRADS IV-V when reported, or with punctate microcalcifications, lobulated/irregular margins, sonographically apparent extrathyroidal extension, reported by institutional radiologists), those with a history of head/neck irradiation, those with a known mutation related to the development of PTC, as well as patients with postsurgical pathology consistent with PTC with a maximal tumor diameter ≥1 cm.
Eligible subjects were divided into those with CLT, GD, or multinodular goiter (MNG), based on preoperative diagnosis and/or background pathology of the specific thyroid disorder. Pathologists at both institutions follow routine and systematic evaluation of thyroid specimens. For a single dominant circumscribed nodule, a minimum of 10 sections (or the entire nodule if smaller) that include the capsular parenchymal interface were generated. For single nonencapsulated lesions larger than 2 cm, several sections of the tumor, including surrounding margins adjacent to normal thyroid, thyroid capsule, and isthmus, were analyzed. For multinodular glands, sections of several representative nodules (∼3–5 per lobe) were routinely analyzed, including any unusual or suspicious nodules. For diffusely enlarged homogeneous glands (such as GD), a minimum five sections from each lobe were processed, although additional sections were warranted for heterogeneous glands to sample a variety of areas. The latter is especially relevant for cases such as Hashimoto thyroiditis to detect small PTCs.
The incidence of PTMc was identified and compared between the different subgroups. GraphPad Prism software v.6.1 (GraphPad Software, Inc., La Jolla, CA) was used for the statistical analysis. Normality of the data distribution was assessed with the Kolmogorov–Smirnov test. Data not following the normal distribution were log-transformed. Categorical variables were compared using the nonparametric Kruskal–Wallis test, and the data are presented as mean ± standard deviation. Proportions were analyzed with chi-squared test (χ 2), and odds ratios (OR) and 95% confidence intervals [CI] were calculated. A p-value of <0.05 was deemed significant. The present study was approved by institutional review boards at both institutions.
Results
A total of 6096 consecutive cases of total thyroidectomy at both institutions (A: 2711, B: 3385) were reviewed: 2187 subjects met our exclusion criteria and the remaining 3909 subjects were included in this analysis. Ultimately, 569 cases of PTC were identified (incidence 14.6%). The age and sex of the entire study population and those in each subgroup are presented in Table 1. The incidence of incidentally discovered PTC among all subjects and subgrouped by sex, as well as their comparisons are presented in Table 2.
Baseline Characteristics of the Study Population
SD, standard deviation.
Papillary Thyroid Microcarcinomas by Sex and Population Group
CI, 95% confidence interval; PTMc, papillary thyroid microcarcinomas.
The incidence of PTC is presented in Table 3 and depicted in Figure 1. The incidence of PTC was compared between groups and was found to be significantly higher in patients with CLT compared with MNG (OR = 1.75 [CI 1.42–2.16], p < 0.0001) or GD (OR = 2.25 [CI 1.53–3.3], p < 0.0001). Also, patients with MNG had a higher PTC incidence compared with GD, although this comparison is not statistically significant (OR = 1.29 [CI 0.9–1.84], p = 0.19). Lymphatic spread of the tumor and tumor size was not statistically significantly different between subgroups. We also found 19 cases of FTC (0.49%), 18 in group A and 1 in group B. CLT was present in 3 FTC patients and MNG in 16 patients (OR = 0.89, p = 0.90).
(
Incidence of Papillary Thyroid Microcarcinomas by Subgroup
Statistically significantly higher incidence of PTC compared with group A.
+LN, metastasis to the regional lymph nodes; CLT, chronic lymphocytic thyroiditis; MNG, multinodular goiter; PTC, papillary thyroid cancer; TMD, tumor maximal diameter.
Discussion
PTC incidence has been rising worldwide for decades (1). This increase comprises all disease stages, but the steepest rise is found in DTMc (1). These are tumors <1 cm in largest diameter, which in many cases, were not known to exist preoperatively and are incidentally discovered by surgical pathology. The vast majority of the incidentally discovered tumors are of the papillary histological type (1). Despite their usually indolent behavior, they can occasionally present with aggressive features such as extrathyroidal extension, regional lymph node involvement, or even distant metastasis, and therefore produce disease-related morbidity (2,3).
Concurrently with the increasing incidence of differentiated thyroid cancer, autoimmune thyroid disorders have been on the rise for several decades as well (4,6). Since autoimmunity is a form of inflammation, which is thought to favor tumorigenesis in several organ systems (5), the rising incidence in autoimmunity could have a significant impact on thyroid cancer development. Indeed, studies dating back to the 1950s have found an association between CLT and PTC in postsurgical series (7). This hypothesis was challenged by a prospective study published in the 1980s that failed to reveal such an association as thyroid cancer was rarely clinically diagnosed in patients with Hashimoto thyroiditis (8). Following that study, a large number of surgical pathology studies continued to point out such an association (9 –13), but the risk of selection bias was implied, due to the nature of these studies.
To avoid such a selection bias, we designed the current study by excluding all patients who underwent surgery for clinically diagnosed thyroid cancer from our analysis. This led to the exclusion of patients undergoing surgery for thyroid nodules with sonographic features suspicious for cancer, those with FNA findings, which are frequently found to be malignant, or are known to raise the likelihood for cancer diagnosis (e.g., AUS), those with a history of exposure to ionizing radiation, or the presence of a family history of thyroid cancer. Therefore, the present study included only patients with truly incidentally discovered PTC.
Our analysis found a highly significant association between the presence of background CLT by pathology and incidental microscopic carcinomas of the papillary histological type when compared with those found in patients without autoimmune thyroid disease. The association was even stronger when compared with patients with GD in whom the likelihood of carrying such tumors was nonstatistically significantly lower than in patients with no autoimmune thyroid disease. These findings suggest that the various forms of autoimmune responses could have different effects on their ability to promote or suppress tumorigenesis. This is in agreement with previous findings published by our group, where the presence of distinct populations of immune cells in thyroid glands seemed to confer protection from PTC or promote its formation and survival (14,15). In addition, patients with autoimmune thyroiditis harboring thyroid malignancies, and those with thyroid malignancies without autoimmune thyroiditis, are found to have different epitope recognition patterns by thyroglobulin antibodies, indicating differences in immune responses between the two conditions (16). In another study, the cytokine profile of patients with PTC and associated autoimmune thyroiditis indicated a marked shift toward Th2 lymphocyte-mediated immunity than in those with autoimmune thyroiditis alone (17).
Of note, some studies have suggested that thyroid cancer coexisting with GD might be more frequent and aggressive compared with that found in patients without GD (18,19). Our present observation of a lower incidence of PTMc in GD, however, is supported by our recently published study, which showed that the immunologic conditions that affect carcinogenesis in patients with GD could have a suppressive effect on cancer development (15).
Thyroid cancers in patients without autoimmune thyroid disorders have been found to be less frequent but more aggressive than the ones found in patients with overt autoimmune thyroid disorders (either GD or Hashimoto thyroiditis) (13,15,20 –23), with the exception of patients younger than 45 years, in one study (24).
Some studies have identified an imbalance between cytotoxic and regulatory T lymphocytes in the peritumoral microenvironment in patients with CLT, which may affect the tumor-specific immune response (14,20). Therefore, the specific type of inflammatory cells (cytotoxic macrophages type 1 in GD and overt Hashimoto's, or regulatory macrophages type 2 and double negative T cells in silent euthyroid Hashimoto's) (14,15) could determine the fate of a thyroid cancer.
In conclusion, our study suggests that the presence of CLT as a background disease is an important risk factor for small, incidentally discovered PTCs when compared with those found in GD, or the absence of any known form of autoimmune thyroid disease in patients undergoing total thyroidectomy for entirely benign indications.
Footnotes
Acknowledgment
We would like to thank Dr. Herbert Chen for sharing U.S. postoperative database.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported in part by institutional grants to J.C.J.