
Abstract
Background:
Patients with primary hypothyroidism are treated with levothyroxine (LT4) to normalize their serum thyrotropin (TSH). Finding the optimal dosage is a long-lasting process, and a small change can have major impact. Currently, limited data are available on the impact of dose-equivalent substitution between brands. This study aimed to determine the effect of the shortage of the LT4 brand Thyrax® in the Netherlands and the resulting dose-equivalent switch to another brand on plasma TSH concentrations in a large cohort of patients.
Methods:
Observational cohort study. Two registries representative for the Dutch population containing prescription and laboratory test data: the Nivel Primary Care Database and the PHARMO Database Network. Patients using at least 25 μg Thyrax daily for one year or longer were included. Two cohorts were formed: a switch cohort consisting of patients who switched from Thyrax to an alternative brand, and a Thyrax cohort including patients who continued to use Thyrax. Patients in the switch cohort did switch from Thyrax to a different brand of LT4 in 2016 and had two consecutive TSH measurements on the same dose of LT4, one before and one 6 weeks after the switch. Patients in the Thyrax cohort had two consecutive TSH measurements on the same dose of Thyrax that were 6 weeks apart.
Results:
In the Thyrax cohort, 19% of euthyroid patients using ≤100 μg had a TSH level outside the reference range at the subsequent measurement compared with 24% in the switch cohort (p < 0.0001). For patients using >100 μg Thyrax, these figures were 24% and 63%, respectively (p < 0.0001). Furthermore, patients using >50 μg Thyrax were four to five times more likely to become hyperthyroid after a dose-equivalent switch to a different brand compared with patients who stayed on Thyrax.
Conclusions:
In euthyroid patients continuing the LT4 product Thyrax at the same dose, TSH was out of range in 19–24% at least 6 weeks later. A dose-equivalent switch from Thyrax to other LT4 brands induced biochemical signs of overdosing in an even larger proportion (24–63%) of patients. The results indicate that a dose-equivalent LT4 brand switch may necessitate a dose adjustment in a large number of patients.
Introduction
Primary hypothyroidism is a common condition with an estimated prevalence in the general population ranging between 0.3% and 3.7% in the United States and between 0.2% and 5.3% in Europe depending on the definition used (1). Consequently, a considerable proportion of the adult population receives lifelong treatment with thyroid hormone. Standard treatment of hypothyroidism consists of daily oral administration of synthetic levothyroxine (LT4). The dose is titrated to achieve physiological plasma concentrations of thyrotropin (TSH).
Patients with hypothyroidism should receive optimal substitution therapy reflected in a normal TSH to minimize thyroid-related complaints. The standard treatment modality for hypothyroidism is substitution with LT4 [for review, see Ref. (2)]. Stable substitution is only possible if the LT4 bioavailability from LT4-containing tablets is constant. In recent years, there have been several examples of changes in the formulation and packaging of LT4 tablets or availability of LT4 tablets necessitating a brand switch, which resulted in a sharp increase in reported side effects in a number of European countries (3). In December 2013, the manufacturer of the LT4 brand Thyrax® in the Netherlands (Aspen) changed the packaging from vials to blisters, which resulted in by more than 2000 reports of side effects to Lareb, the Dutch National Pharmacovigilance Centre. However, the reason for these complaints remains speculative at this stage but may relate to differences in degradation of the product in relation to the packaging (4).
In 2017, the manufacturer of Euthyrox® in France changed the formulation of Euthyrox resulting in a steep increase of reported side effects among 3 million Euthyrox users in France (5). The new formulation of Euthyrox was introduced to the market after pharmacokinetic bioequivalence testing (6). As such, the new product was rated AB (therapeutically equivalent). These health issues prompted the European Thyroid Association (ETA) together with the Thyroid Federation International (TFI), the umbrella organization for thyroid patient organizations from many parts of the world, to issue a position statement on the interchangeability of LT4 products in EU countries. The position statement recommends that patients should be maintained on the same formulation/brand name of LT4, that manufacturers should carefully prepare the introduction of a formulation change together with representatives of relevant stakeholders, and that the preparation of a formulation change should include a monitoring plan to become active immediately after introduction. Moreover, the definitions of LT4 potency and bioequivalence requirements should be reevaluated (3).
Currently, very limited data are available on the impact of dose-equivalent substitution between preparations on the biochemical control as reflected by plasma free thyroxine and TSH concentrations (6,7). In 2016, the manufacturer of Thyrax moved one of its production facilities from the Netherlands to Germany. Due to start-up issues at the new facility, Thyrax was unavailable for many months, and consequently ∼350,000 patients using Thyrax (∼75% of all LT4 users in the Netherlands) had to switch to another LT4 brand. This undesirable situation in terms of public health offered a unique opportunity to study the effects of a forced LT4 brand switch by using data from two independent databases. The aim of the present study was to determine the effect of a dose-equivalent LT4 brand switch resulting from a shortage of the LT4 brand Thyrax on plasma TSH concentrations in a large cohort of patients.
Materials and Methods
Study design and data sources
For this study, data from two registries were used, the Nivel Primary Care Database (Nivel-PCD) and the PHARMO Database Network (PHARMO). The Nivel-PCD contains routinely collected electronic medical records from 500 general practices in the Netherlands and contains data about visits to the general practitioner (GP), the medical history of patients, prescriptions, and results from laboratory tests. The PHARMO is a population-based network of health care databases combining data from different health care settings on a patient level, including outpatient pharmacies and clinical laboratories. The registries each contain a representative sample of the Dutch population. There is no overlap between the two samples of the two registries; therefore, it was possible to pool the data without including patients twice. Separate baseline characteristics for the two registries are shown in Table 1. Based on their similarity, both registries were pooled. From this pooled data set, two cohorts of patients were formed. The first cohort consists of patients who used the LT4 brand Thyrax in 2014 (PHARMO) or 2015 (Nivel-PCD) (the Thyrax cohort). The second cohort consists of patients who used Thyrax in 2016 and were forced to switch to a different brand of LT4 in 2016 due to the shortage of Thyrax (the switch cohort).
Patient Characteristics (Per Cohort and Registry)
LT4, levothyroxine; SD, standard deviation; TSH, thyrotropin.
Selection of patients
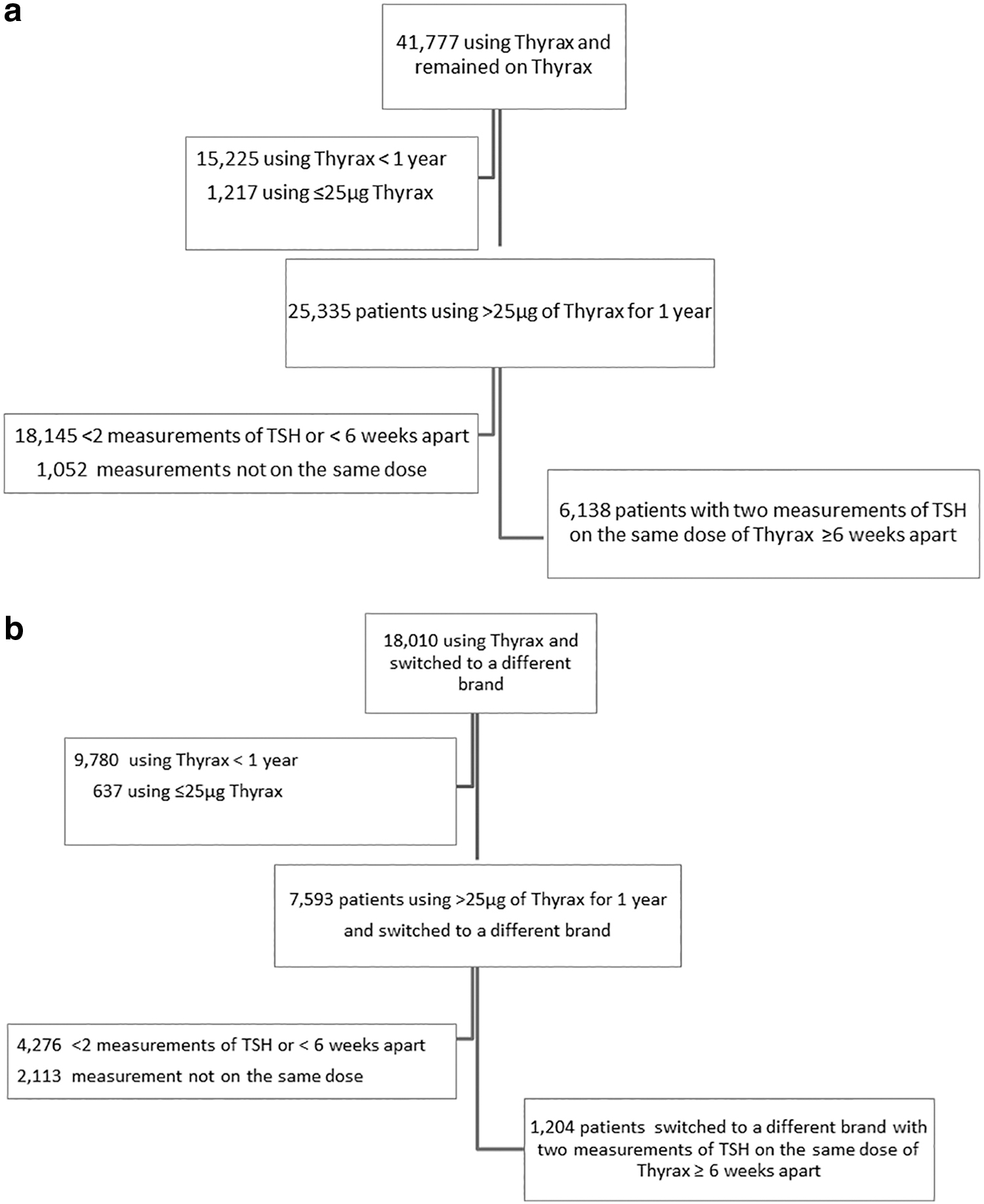
From both cohorts, patients who were known to have used at least 25 μg Thyrax daily for one year or longer were selected. Patients from the switch cohort needed to switch to a different brand of LT4 in 2016 and to have two consecutive measurements of TSH of the same dose of LT4, one before and one after the switch. The first measurement of TSH took place while still using Thyrax and the second measurement while using the new LT4 brand for at least 6 weeks. The median time interval between these measurements was 37 weeks (PHARMO) and 14 weeks (Nivel-PCD). Patients from the Thyrax cohort needed to have two consecutive TSH measurements on the same dose of Thyrax that were at least 6 weeks apart. The median time interval between these measurements was 25 weeks (PHARMO) and 28 weeks (Nivel-PCD). In Nivel-PCD, the date of prescription of medication is known, and in PHARMO, the date of dispensing is known. As such, assumptions about the duration of use could be made. In the Netherlands, prescription drugs are allowed to be dispensed for a maximum medication use of 3 months. For the present study, we assumed that patients who had two prescriptions/dispenses of LT4 that were less than six months apart represented continued use of LT4. If two prescriptions/dispenses were apart for more than six months, we assumed that patients used the medication for three months, discontinued the use of LT4 and restarted at the second prescription. Flowcharts for the Thyrax cohort and the switch cohort are shown in Figure 1.
(
Statistical analysis
Baseline characteristics including age, sex, and average dose of Thyrax were assessed for both cohorts separately. To unmask potential dose-dependent effects, all analyses were carried out separately for patients who used ≤100 and >100 μg LT4, assuming that the impact of a brand switch might be more pronounced for patients using a higher dose. Measures of TSH were divided into hyperthyroid, normal, and hypothyroid according to the Dutch guidelines for GPs. TSH concentrations were considered normal between 0.4 and 4.0 mIU/L, reflecting hyperthyroidism when <0.4 mIU/L and hypothyroidism when >4.0 mIU/L. For both cohorts, the proportion of patients belonging to each of the TSH groups was compared between the first and second TSH measurement using a chi-square test. As the effect of a brand switch on plasma TSH appeared to be different for patients who used ≤100 or >100 μg LT4, the patients were divided into six subgroups based on the dose (26–50, 51–75, 76–100, 101–150, 151–200, and >200 μg) to observe if there was dose equivalence for the whole range of doses for those who did and did not switch from brands of LT4. Per subgroup, the percentage of patients who were hyperthyroid or hypothyroid at the second measurement was calculated.
Results
Patients
For both cohorts, about 2% of all patients in the combined registries used Thyrax. The switch cohort consisted of 18,010 eligible patients and the Thyrax cohort consisted of 41,777 eligible patients (Fig. 1a, b). Most patients were excluded because they used Thyrax for less than a year and/or at a dose <25 μg per day. Of the selected Thyrax users in the Thyrax cohort, 20% had at least two consecutive measurements of TSH on the same dose of Thyrax that were at least 6 weeks apart. For the switch cohort, 9% of the selected Thyrax patients fulfilled the criteria. This lower percentage is mainly caused by the more strict criteria for the switch cohort: switch of LT4 brand and two consecutive measurements around this switch. In the end, 6438 patients fulfilled the criteria and were selected for the Thyrax cohort and 1204 patients for the switch cohort (Table 1). Although the percentage of included patients was different for the switch cohort, the characteristics of both cohorts were similar (Table 1). In both cohorts, 85% of the patients were women, and the mean age was around 60 years. Only the dose of Thyrax used differed slightly between the two cohorts.
Changes in TSH concentrations between two measurements
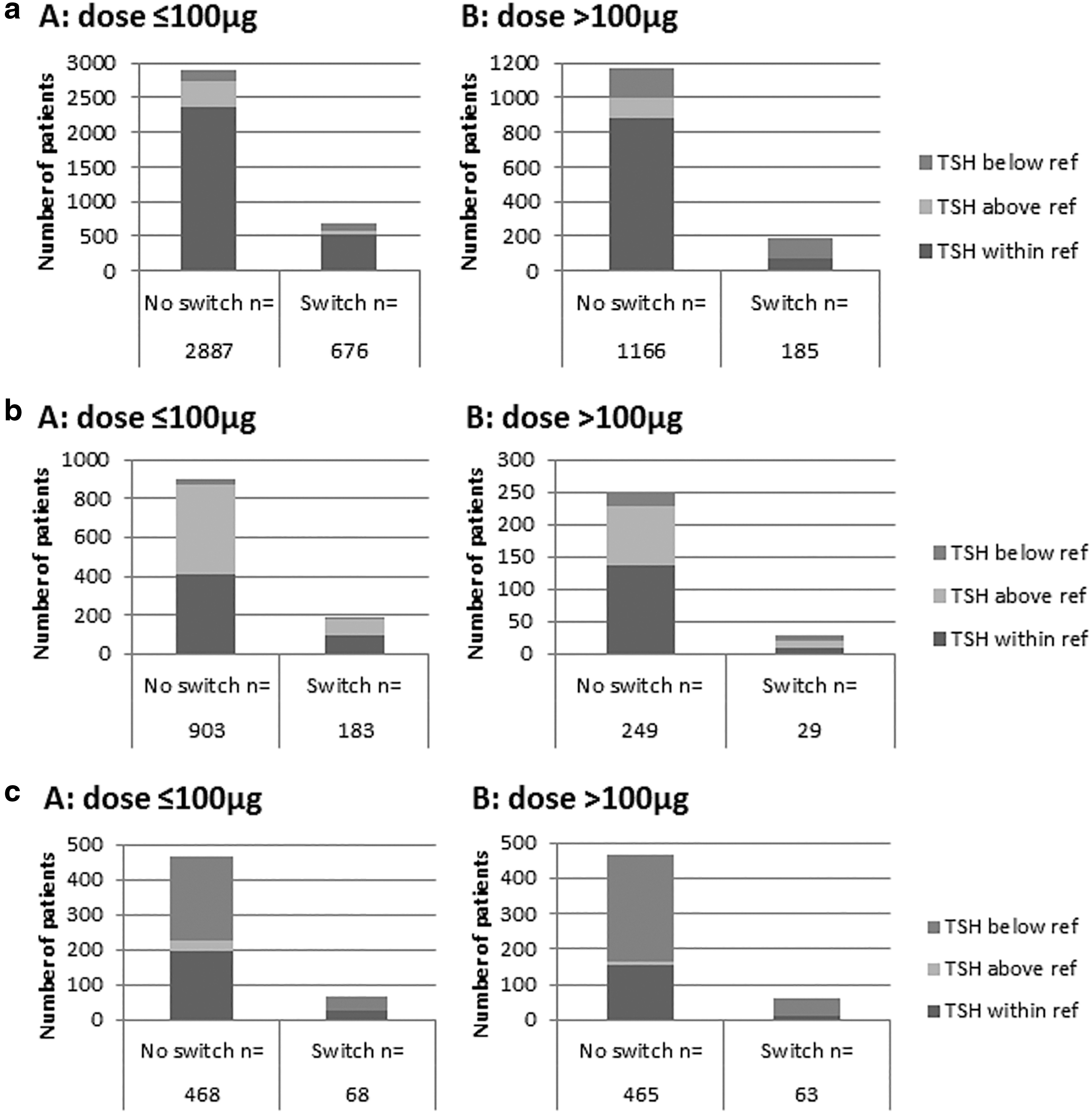
Plasma TSH concentrations at the second measurement for patients with a normal, elevated, or decreased initial TSH are shown in Figure 2a, b, and c, respectively. Of the patients with a normal TSH at the first measurement, who used a low dose of Thyrax (≤100 μg) and who did not switch to a different brand, 19% had a TSH level outside the reference range at the second measurement (Fig. 2a). When patients with a normal TSH at the first measurement used ≤100 μg Thyrax and switched to a different brand, 24% had a TSH level outside the reference range after the switch (Fig. 2a). This difference in the percentage of TSH outside the reference range at the second measurement between the Thyrax cohort and the switch cohort was statistically significant (p < 0.00001). There was no statistically significant difference in the percentage of TSH outside the reference range at the second measurement between the Thyrax cohort and the switch cohort for patients with a first TSH measurement outside the reference range.
(
For patients who used >100 μg Thyrax, a similar but much more pronounced pattern was observed. Of the patients with a normal TSH at the first measurement who did not switch to a different brand, 24% had a TSH level outside the reference range at the next measurement. Of the patients who did switch, 63% had a TSH level outside the reference range at the next measurement (Fig. 2a) (p < 0.00001). The majority of these patients had plasma TSH concentrations below the reference range, indicative of overdosing.
The observation that patients in the switch cohort who used >100 μg Thyrax were more likely to become hyperthyroid at the second measurement than patients on a lower Thyrax dose suggested that different brands are not bioequivalent. To study dose dependency in more detail, the percentage of patients with a normal TSH at the first measurement who became hyperthyroid or hypothyroid at the second measurement was calculated for six different dose groups of LT4 (Table 2). We found that patients with a normal TSH who switched from Thyrax to the same dose of a different brand of LT4 (Euthyrox, Levothyroxinenatrium Teva®, Nycomed®, or Thyrofix®) were four to five times more likely to develop hyperthyroidism compared with patients who did not switch between brands if they used >50 μg of LT4, whereas there was no obvious difference for patients using 50 μg or less. Patients were less likely to develop hypothyroidism compared with patients who did not switch between brands. This strongly suggests that the different brands of LT4 are not bioequivalent.
Bioequivalence
The table shows the percentage of patients who became hyperthyroid or hypothyroid at the second measurement when the first plasma TSH was within reference in both cohorts per dosage of LT4 used.
Discussion
The population prevalence of thyroid hormone medication use by adults in the Netherlands was recently reported to be 3.1%. In 2016, ∼350,000 patients using the LT4 brand Thyrax had to switch to another LT4 brand. By analyzing data from two independent Dutch registries containing data on medication use and laboratory measurements, we were able to determine the effect of dose-equivalent substitution between different LT4 preparations on plasma TSH concentrations. Of the patients with a normal TSH using ≤100 μg Thyrax daily, a small but statistically significant increase in the proportion of patients with a TSH level outside the reference range was identified at the next measurement in the switch cohort compared with patients who continued use of Thyrax (24% vs. 19%). For patients using >100 μg, these figures were 63% and 24%, respectively (p < 0.0001), indicating a substantial number of patients in need of a dose change after the brand switch. Furthermore, patients using >50 μg Thyrax were four to five times more likely to become hyperthyroid after a dose-equivalent switch to a different LT4 brand compared with patients who stayed on Thyrax. Thus, a dose-equivalent LT4 brand switch may induce biochemical signs of over- or underdosing in a large proportion of patients using >50 μg Thyrax daily. This study also shows that when patients do not switch between brands and remain on the same dose, 20% will be out of range at a second measurement; however, it is unknown whether these patients experience clinical symptoms.
Although the interchangeability of different LT4 preparations has been hotly debated both in the scientific and in the public domain (3,7), only very limited data are available on the impact of dose-equivalent substitution between preparations on the biochemical control in patients with hypothyroidism (7). When the manufacturer of Thyrax (Aspen) moved one of its production facilities from the Netherlands to Germany in 2016, Thyrax became unavailable for many months in the Netherlands and ∼350,000 patients using Thyrax had to switch to another LT4 brand. This created a unique opportunity to provide the first population-based study to address the consequences of a dose-equivalent brand switch of LT4 on plasma TSH. That the motivation for the brand switch was not related to health issues, but rather to the availability of the medication, reduces the risk of selection bias and adds to the strength of the study. We used two different Dutch registries containing data on medication use and laboratory measurements. Both registries have shown to be representative for the Dutch population but reflect a different parts of the population. Thus, the fact that baseline characteristics for the two registries were remarkably similar and TSH data could be pooled further strengthens the present study. Finally, the study is based on unbiased and objective data (brand, dose, TSH) instead of subjective data such as questionnaires and self-reported side effects.
A limitation of the present study is that changes in plasma TSH within the reference range following the switch are not addressed. However, TSH changes within the reference range following a small dose change are unlikely to result in changes in hypothyroid symptoms, well-being, or quality of life (8,9). Furthermore, in the Nivel-PCD prescriptions from the GPs, no actual dispensing data are known, while the reverse is true for PHARMO. Therefore, some patients might have a prescription which they did not collect at the pharmacy. However, this was the case both before and after the shortage of Thyrax. Moreover, only patients using Thyrax for more than one year were included, so that they had obtained at least four prescriptions for Thyrax and were regular users, making it likely that the new prescription was also collected at the pharmacy. Furthermore, TSH measurements needed to be at least 6 weeks apart, so missing data included patients who had a shorter TSH interval, likely resulting from subjective complaints. This may have led to an underestimation of the percentage of TSH outside the reference range at the second time point. A final weakness might be that some patients anticipating a shortage of Thyrax may have started to collect extra stock of Thyrax, and as a consequence did not appear in our switch cohort. However, patients need a prescription provided by a health care provider to obtain Thyrax, and we did not find any compression of frequency of prescriptions, making this less likely.
A relatively large number of studies have addressed the effect of a LT4 formulation change from tablets to a liquid formulation on plasma TSH. A recent systematic review and meta-analysis showed that a significant proportion of patients with suboptimal TSH on tablet LT4 showed improved TSH levels after switching to liquid formulation LT4 at unchanged dose. This indicates that a liquid form of LT4 may increase bioavailability compared with tablets, perhaps resulting from less sensitivity of the liquid formulation to factors reducing the absorption of LT4 tablets (10). Only few data are available on effects of generic versus brand-name LT4 tablets on TSH. A study in children with severe congenital hypothyroidism reported that generic and brand-name LT4 were not bioequivalent, but this was a rather small study in an academic medical center setting (11). To the best of our knowledge, there are no population-based studies available on the effects of a brand or formulation change on serum TSH.
The present study focuses on two LT4 products to replace the brand-name drug Thyrax, that is, LT4 Teva and Euthyrox. Thyrax and Euthyrox are brand name stand-alone drugs and are not generics of each other. LT4 Teva is a generic of L-thyroxin Henning®, which has been registered in Germany but not in the Netherlands. Thus, the products that were substituted cannot be considered AB rated. Therefore, the outcome of our study may not be surprising in the eyes of the regulator, but it certainly is in the eyes of most clinicians and their patients.
Over the past years, a number of European countries have seen major health issues, in particular increased prevalence of reported side effects, after a switch from one LT4 brand to another. Until now, it was not possible to ascertain whether these health issues were pharmacologically related to the brand change as data on the effect of the brand change on thyroid function tests were lacking. The present study reports an increased prevalence of biochemical hyperthyroidism after a dose-equivalent LT4 brand switch from Thyrax to other brands of LT4 in the Netherlands in 2016, especially in patients using >100 μg of LT4 daily. This observation may explain the steep increase in the number of reported LT4 side effects in the Netherlands in 2016 (3). The results of the study suggest that there are differences in bioavailability between the different LT4 brands. Given the considerable prevalence of hypothyroidism, it is very likely that the brand change has led to significantly increased health care consumption and health care expenses. Thus, our study has implications for relevant stakeholders, including health care professionals, national endocrine societies, medicine evaluation boards, pharmacovigilance centers, pharmacists and GP associations, and thyroid patient organizations as it strongly supports a number of recommendations issued recently by the ETA together with the TFI (3). First, patients should be maintained on the same formulation/brand of LT4, if possible. If a change is necessary, a blood test after six weeks should be performed to determine whether any adjustment to dosage is required. Second, manufacturers should carefully prepare the introduction of a formulation change together with representatives of relevant stakeholders to prevent insufficient communication and coordination. Third, the preparation of a formulation change should include a monitoring plan to become active immediately after introduction.
The extent of the burden of the forced brand switch following the Thyrax shortage in the Netherlands in terms of mental stress for the patient, health care consumption, and health care expenses is likely to be substantial. One of the key questions is how the observed increase in biochemical signs of hyperthyroidism after the switch for Thyrax to other LT4 brands can be reconciled with the fact that the switch took place within the existing legal framework of regulations and monitoring. A similar question arose from observations in France, where Merck introduced a new formulation for the LT4 brand Levothyrox® based on the need for tighter specification (95–105%) over the whole shelf life. Similar to the Dutch situation, this change involved a large number of patients as 2.6 million patients were being treated in France with Merck's Levothyrox in 2017 (data from the French Agence Nationale de Sécurité des Médicaments). In January 2018, 17,310 reports of adverse effects had been received by the French site for drug surveillance (BNPV, Base National de Pharmacovigilance). This large number of reported side effects was in contrast with a pharmacokinetic study showing that the new formulation meets potency specification and bioequivalence guidelines (6). These discrepancies should be the subject of future research. Furthermore, a joint and multidisciplinary effort is needed to limit the burden for patients with hypothyroidism to prevent increased health care consumption and health care expenses when future brand or formulation changes are anticipated.
In summary, in euthyroid patients continuing the LT4 product Thyrax at the same dose, TSH was out of range in 19–24% at least 6 weeks later. A dose-equivalent switch from Thyrax to other LT4 brands induced biochemical signs of overdosing in an even larger proportion (24–63%) of patients. By inference, a substantial proportion of patients needed a dose adjustment after a LT4 brand switch. Future (forced) changes of brand or formulation should therefore be announced in time, accompanied by balanced patient information, be monitored closely, and include advice on dose adjustment if needed.
Authors' Contributions
All authors participated in designing the study, generating hypotheses, interpreting the data, and critically reviewing the article. L.E.F. and E.F. wrote the first draft of the report. Other members of the writing group were J.G.K., J.C.K., P.H.B., and T.P.L., with support from L.v.D., R.H., K.H., and E.H. L.E.F., K.H., J.G.K., and E.H. had full access to anonymized individual-patient data. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Ethical Approval
The use of electronic health records for research purposes under certain conditions. When these conditions are fulfilled, neither obtaining informed consent from patients nor approval by a medical ethics committee is obligatory for this type of observational studies containing no directly identifiable data (art. 24 GDPR Implementation Act jo art. 9.2 sub j GDPR).
Dissemination Plan
The results of this study are integrated in the advice given to GPs in case patients need to change from levothyroxine brand.
Transparency
The lead author affirms that this article is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Exclusive Licenses
The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors, a worldwide license to the publishers and its licensees in perpetuity, in all forms, formats, and media (whether known now or created in the future), to (i) publish, reproduce, distribute, display, and store the contribution, (ii) translate the contribution into other languages, create adaptations, reprints, include within collections, and create summaries, extracts, and/or abstracts of the contribution, (iii) create any other derivative work(s) based on the contribution, (iv) exploit all subsidiary rights in the contribution, (v) the inclusion of electronic links from the contribution to third party material wherever it may be located, and (vi) license any third party to do any or all of the above.
Footnotes
Author Disclosure Statement
All authors have completed the ICMJE uniform disclosure form and declare: no support from any organization for the submitted work (except the research grants listed in funding); no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Funding Information
This study was supported by a grant from the Netherlands Organisation for Health Research and Development (ZonMw) on advice from The Dutch Ministry of Health, Welfare and Sport. The sponsor had no involvement in the conduct of the study nor the interpretation of the findings or the writing of the article.