
Abstract
Background:
Diagnosis of thyrotropin (TSH)-secreting pituitary adenomas (TSHoma) before surgery remains a challenge, especially for microadenomas. We aimed to establish a short-term somatostatin analogue (SSA) test to differentiate TSHomas from other causes of syndromes of inappropriate secretion of TSH (IST), mainly resistance to thyroid hormone β (RTHβ).
Materials and Methods:
We first evaluated the sensitivity and specificity of SSA test in a training cohort (TSHoma, n = 32; RTHβ, n = 20). The test was then validated in an independent cohort (TSHoma, n = 9; RTHβ, n = 2). We finally applied the SSA test in 12 perceptively enrolled IST cases with negative imaging findings and absent thyroid hormone receptor beta (THRB) mutations or mixed hormone imbalances.
Results:
Both TSHoma and RTHβ patients showed a decrease of TSH at the start of the SSA test, but the velocity of the TSH suppression slowly decreased in RTHβ patients after 2 hours. The suppression ratio of TSH at 24 hours versus 2 and 0 hours was significantly greater in TSHoma patients compared with RTHβ patients (70.58% ± 18.6% vs. 6.01% ± 25.41%, p < 0.0001, 79.83% ± 12.79% vs. 51.16% ± 13.62%, p < 0.0001, respectively). The 24- versus 2-hour suppression ratio showed the best diagnostic accuracy at a cut point of 44.46% in the training cohort, with a sensitivity of 95.00%, a specificity of 93.75%, and a positive predictive value (PPV) of 88.89%. The accuracy was confirmed in the validation cohort. Three out of 12 patients in the prospective cohort showed a TSH suppression ratio greater than 44.46% and all developed microadenomas during follow-up.
Conclusions:
A short-term SSA test provides an alternative diagnostic approach for TSHomas. A positive SSA test result is suggestive for a TSHoma even before positive findings become apparent on pituitary imaging. However, studies including larger number of patients, especially those with RTHβ, are needed to confirm our findings.
Introduction
The regulation system of thyroid hormones (THs) involves a precise negative feedback control mechanism, including the hypothalamus, pituitary, the thyroid gland, and thyroid hormone receptors (TRs) in peripheral organs. Dysfunction of this negative feedback leads to syndromes of inappropriate secretion of TSH (IST), characterized by elevated TH and unsuppressed thyrotropin (TSH) concentrations.
A TSH producing tumor, mainly TSH-secreting pituitary adenomas (TSHomas), can produce excessive amounts of TSH and thereby result in high levels of THs and present as IST (1). Patients with mutations in the thyroid hormone receptor beta (THRB) have a reduced sensitivity to THs, resulting in the syndrome of resistance to thyroid hormone β (RTHβ) (2,3), which also results in IST. In addition to TRβ, genetic defect in TRα, the monocarboxylate transporter 8 (MCT8), and the SECIS binding protein 2 (SBP2), among others, can also lead to reduced sensitivity to THs. However, these patients may present with different clinical and biological characteristics compared with patients with RTHβ.
The differential diagnosis of TSHoma from RTHβ can be challenging. Ideally, TSHomas should be associated with positive pituitary findings, lack a response to the thyrotropin-releasing hormone (TRH)/triiodothyronine (T3) test, and carry no germ line THRB mutations (1). However, the presence of a pituitary microadenoma has also been reported in a patient with RTHβ (4), and IST patients with negative pituitary findings may develop TSH producing microadenomas during long-term follow-up (5). A T3 suppression test can be contraindicated in elderly patients or in those with coronary heart disease. Finally, 25% of patients with an RTH phenotype do not have THRB germ line mutations (2). Guidelines suggest a comprehensive diagnostic algorithm, including family history, biochemical tests, dynamic tests, pituitary imaging, and germ line THRB sequencing (1). However, there are patients with negative pituitary findings, negative germ line mutations (double negative), and no access to TRH or T3 tests.
Expression of somatostatin receptors (SSTRs), particularly SSTR2 and SSTR5, is one important feature of TSHomas. Consequently, somatostatin analogues (SSA) have been suggested as first-line treatment for TSHomas, with long-acting SSA achieving a TSH suppression in 80% of patients (6). In contrast, RTHβ patients show a less significant TSH suppression compared with patients with TSHomas (7). These findings suggest that SSA might be used in differentiating TSHomas from RTHβ. In 2005, Mannavola et al. (8) found a significant reduction of free triiodothyronine (fT3) and free thyroxine (fT4) after two injections of long-acting octreotide in TSHoma patients, but not in RTHβ patients. The authors concluded that administration of long-acting SSA for at least 2 months can differentiate TSHomas and RTHβ. However, the test is time-consuming and the sample size was limited (eight TSHoma and four RTHβ patients).
In the present study, we aimed to establish a short-term SSA test to diagnose TSHomas by exploring the TSH response to a series of octreotide injections in patients with IST.
Materials and Methods
Study design and patients
We first retrospectively reviewed 87 patients with confirmed diagnosis of IST in Ruijin Hospital from 2004 to 2013. All patients withdrew antithyroid drug for at least 3 weeks and had independent tests with intervals of at least 1 month. We excluded patients who had a history of thyroidectomy or radioiodine therapy, or who refused to undergo a short-term SSA test. A total of 52 patients were included as the training cohort to evaluate the sensitivity and specificity of the SSA test. Patients diagnosed with TSHomas (n = 9) and RTHβ (n = 2) from 2014 to 2019 were included as the validation cohort to validate the diagnostic accuracy of the SSA test. We finally applied the test in prospectively enrolled patients with IST, including 10 patients negative for THRB gene mutations and imaging findings, as well as two patients with microadenomas cosecreting prolactin (PRL)/TSH or growth hormone (GH)/TSH (Fig. 1).

Diagnosing flowchart of patients with IST. IST, inappropriate secretion of thyrotropin.
Dynamic tests, including TRH and T3 tests, were performed as previously reported (2). A positive TRH test was defined as a TSH increase of more than 50% of baseline and a net increase of at least 4 mU/L according to previous studies (9,10). Transsphenoidal or subfrontal adenomectomy was performed for those with pituitary adenomas on MRI. A TSHoma was diagnosed when the surgery achieved euthyroidism and positive TSH staining was detected in the resected pituitary adenoma. RTHβ was diagnosed when a pathogenic germ line THRB mutation was detected according to the 2015 American College Medical of Genetics (ACMG) guidelines (11). The Board of Medical Ethics of Ruijin Hospital approved the study, and all patients provided informed written consent.
Short-term SSA test
Sandostatin (Novartis, Switzerland) was administered subcutaneously three times at a dose of 100 mcg every 8 hours. Serum TSH levels were measured at 0, 2, 4, 6, 8, and 24 hours after the first injection. The short-term SSA tests were conducted with an interval of 3 days from other dynamic tests, if applicable.
Thyroid function tests
Thyroid function and antibody measurements were performed in the Shanghai Institution of Endocrine and Metabolic Diseases, which is certified by the College of American Pathologists. Levels of serum fT3, fT4, TSH, thyroid peroxidase antibodies (TPOAb), and thyroglobulin antibodies (TgAb) were determined by chemiluminescent microparticle immunoassays (Abbott Laboratories, Abbott Park). We used the M22 monoclonal antibody (Roche Diagnostics, Switzerland) to test the presence of serum TSH receptor antibodies (TRAb). The reference ranges were as follows: fT3: 2.62–6.49 pmol/L; fT4: 9.01–19.047 pmol/L; TSH: 0.35–4.94 lU/mL; TRAb: <1.75 U/L; TPOAb: <5.61 IU/mL; and TgAb: <4.11 IU/mL. Serum sex hormone-binding globulin (SHBG) concentrations were measured on the Abbott Architect i2000SR system using chemiluminescence. The SHBG ratio was expressed as value of SHBG to upper reference limit (URL) corrected for age and sex. The URL of SHBG recorded in normal controls matched for age and sex according to the manufacturer's instructions and previous reports (12) and was as follows: (1) prepubertal boys and girls, 162.4 nmol/L; (2) premenopausal women, 147.7 nmol/L; (3) postmenopausal women, 118 nmol/L; and (4) men, 77.6 nmol/L.
THRB mutation analysis
Germ line DNA from peripheral blood was extracted using the QIAamp DNA Mini Kit (Qiagen, Germany) and evaluated by NanoDrop 2000 spectrophotometer (NanoDrop Technologies, Wilmington, Germany). Polymerase chain reactions were performed in 25 μL of buffer containing 1.5 mM MgCl2, 200 mM deoxynucleoside triphosphates, 50–100 ng genomic DNA, 0.5 mM of each primer, and 2.5 U Taq DNA polymerase (Takara, Tokyo, Japan). Thirty-five cycles with annealing temperatures optimized at 60° were performed. Exons 3–10 of the THRB gene were amplified and analyzed by Sanger sequencing using specific primers (Supplementary Table S1).
Statistical analyses
The thyroid function tests (TFTs) and other biochemical parameters are reported as mean ± standard deviation. Statistical analyses were performed using SPSS version 21 and a p < 0.05 was considered statistically significant. Receiver operating characteristic (ROC) curves were plotted by GraphPad Prism 6. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were evaluated by best area under the ROC curve (AUC) with 95% confidence interval (CI) according to the method by Agresti and Coull (13).
Results
Clinical characteristics of patients
In the training cohort, patients with TSHomas (N = 32) were older at the age of diagnosis (44.88 ± 13.28 vs. 24.80 ± 12.45, p < 0.0001) and showed higher SHBG levels (75.50% ± 38.56% vs. 38.69% ± 20.82%, p < 0.001) than patients with RTHβ (n = 20) (Supplementary Fig. S1). There was no significant difference in (TFTs) between the two groups (Supplementary Table S2). The median size of TSHomas was 12.9 mm (interquartile range [IQR] 10.0–19.5). Five TSHoma patients (15.6%) had pituitary microadenomas and one had an ectopic nasopharyngeal TSHoma. One RTHβ patient showed a 2 mm microadenoma with normal anterior pituitary hormone profiles (Supplementary Fig. S2). All mutations found in RTHβ patients were missense mutations in exons 7–10 of the THRB gene.
In the validation cohort, the median age in TSHoma patients (n = 9) was 52.0 years (IQR 46.0–59.5) and the median size of microadenoma was 7.0 mm (IQR 5.5–8.5). Two RTHβ patients carried pathogenic variants in the THRB gene (R320L and Y321C, respectively) and showed negative pituitary findings on MRI scan.
In the application cohort, none had a germ line THRB gene mutation. Ten patients showed negative pituitary MRI findings (double negative IST) and two showed microadenomas with cosecreting PRL/TSH and GH/TSH.
Response to short-term SSA test in patients with IST in the training cohort
Both TSHoma and RTHβ patients showed an instant decrease of TSH (3.234 ± 2.348 vs. 2.627 ± 2.946 mIU/L, p = 0.415) in response to the first injection of octreotide. After 2 hours, TSH continuously decreased in patients with TSHomas, whereas it barely decreased in patients with RTHβ patients, and then returned to baseline at 8 hours. At 24 hours, the TSH level in TSHoma patients was significantly lower than in RTHβ patients (0.884 ± 0.698 vs. 2.773 ± 3.668 mIU/L, p = 0.006). The suppression ratio of TSH suppression at 24 versus 0 hours was significantly greater in TSHoma patients than in RTHβ patients (79.83% ± 12.79% vs. 51.16% ± 13.62%, p < 0.0001). Most strikingly, this difference was even greater for the suppression ratio of TSH at 24 versus 2 hours (70.58% ± 18.69% vs. 6.01% ± 25.41%, p < 0.0001) (Table 1, Fig. 2).
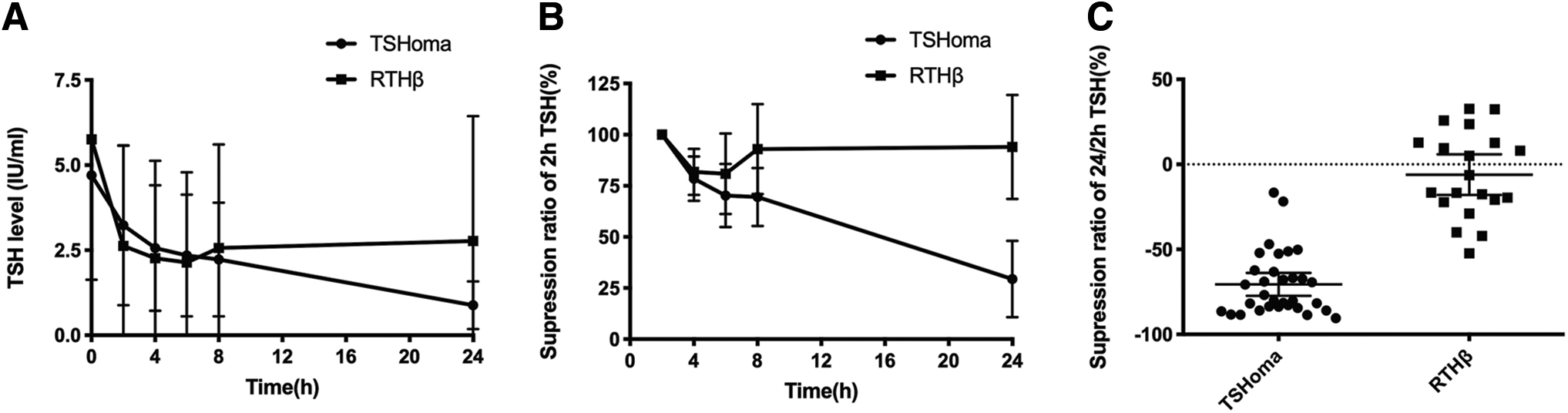
Response to short-term SSA in training cohort. (
Clinical Characteristics of Patients with TSHoma and Resistance to Thyroid Hormone β in Training Group
Ectopic nasopharyngeal TSHoma.
fT3, free triiodothyronine; fT4, free thyroxine; NA, not available; Neg, negative; RTHβ, resistance to thyroid hormone β; SSA, somatostatin analogue; THRB, thyroid hormone receptor beta; TRH, thyrotropin-releasing hormone; TSH, thyrotropin.
Sensitivity and specificity of short-term SSA test in the training cohort
An ROC with best AUC was plotted based on the suppression ratio of TSH at 24 versus 2 hours. The best diagnostic cutoff point of suppression ratio was 44.46% with an AUC of 0.9719. The sensitivity was 95.00% (CI, 75.13–99.87%), and the specificity was 93.75% (CI, 79.19–99.23%) (Fig. 3) for diagnosing a TSHoma.
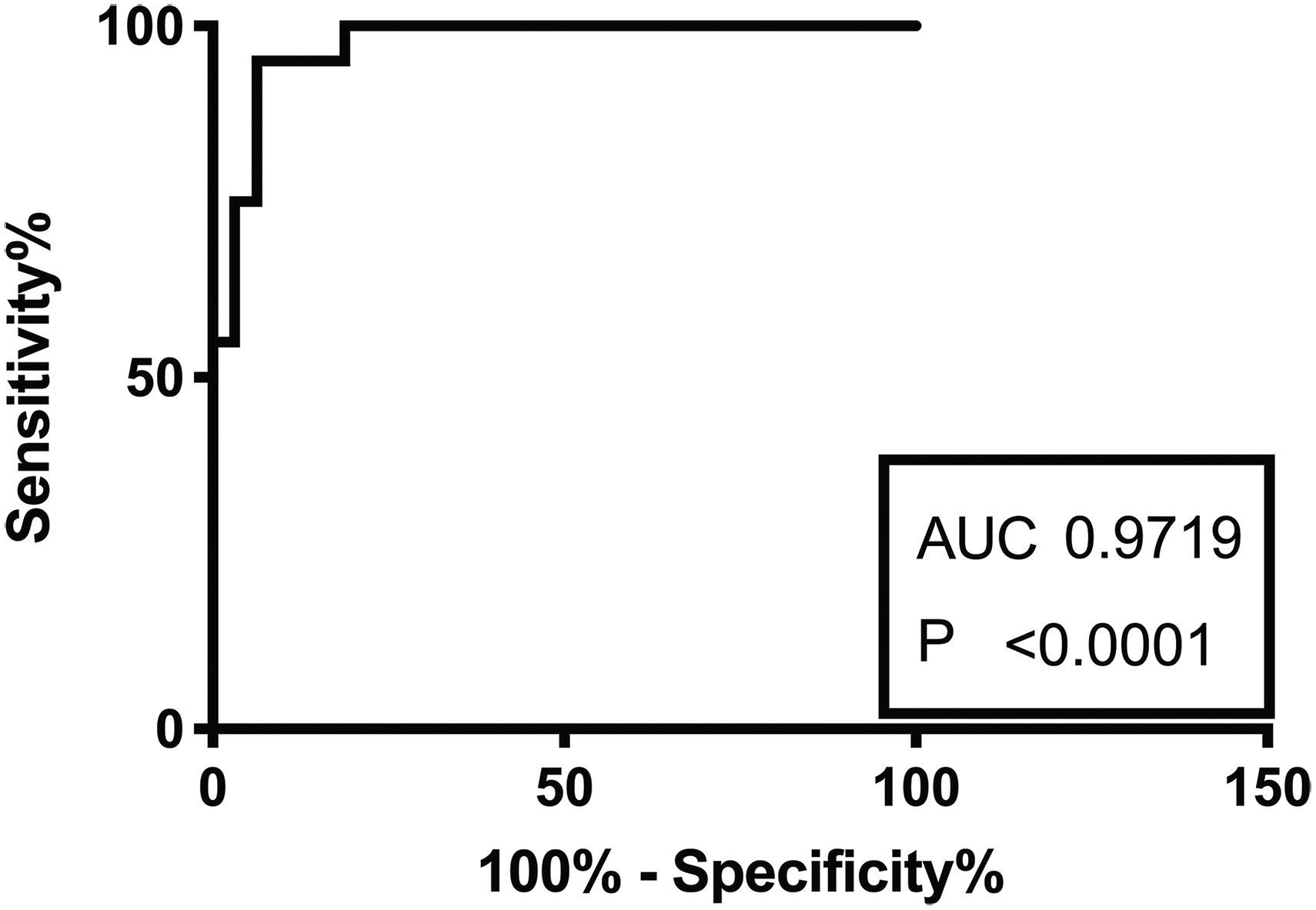
ROC plot of the suppression ratio TSH at 24 versus 2 hours. ROC, receiver operating characteristic.
The suppression ratio of TSH at 24 versus 0 hours showed less diagnostic efficacy. The best cutoff point was 61.40 with an AUC of 0.9344. The sensitivity was 85.00% (CI, 62.11–96.79%), and the specificity was 90.63% (CI, 74.98–98.02%) (Supplementary Fig. S3) for diagnosing a TSHoma.
Validation of the short-term SSA test
With 44.46% as cutoff, eight microadenomas were defined as having a positive response, while three individuals, including one with a microadenoma and two RTHβ patients, were defined as having a negative response (Table 2, Supplementary Fig. S4). The PPV was 8/8 (100%), and the NPV was 2/3 (66.67%).
Clinical Characteristics of Patients with TSHoma and RTHβ in Validation Group
Application of short-term SSA test in IST cases with undetermined diagnosis
We finally applied the short-term SSA test in 12 prospectively enrolled patients with IST. Among the 10 patients with double negative findings, three were defined as having a positive response and all developed pituitary microadenomas during follow-up of 61, 25, and 15 months, respectively (Table 3, Fig. 4). One patient with a 8.3 mm microadenoma underwent surgery and achieved biochemical cure. The removed tumor showed positive staining for TSH. The other two patients refused surgery and are still being followed. Among the seven patients with a negative response in the SSA test, a pathogenic mutation in the ALB gene (p.R242H) was identified in two of them, thus establishing the diagnosis of familial dysalbuminemic hyperthyroxinemia (FDH).
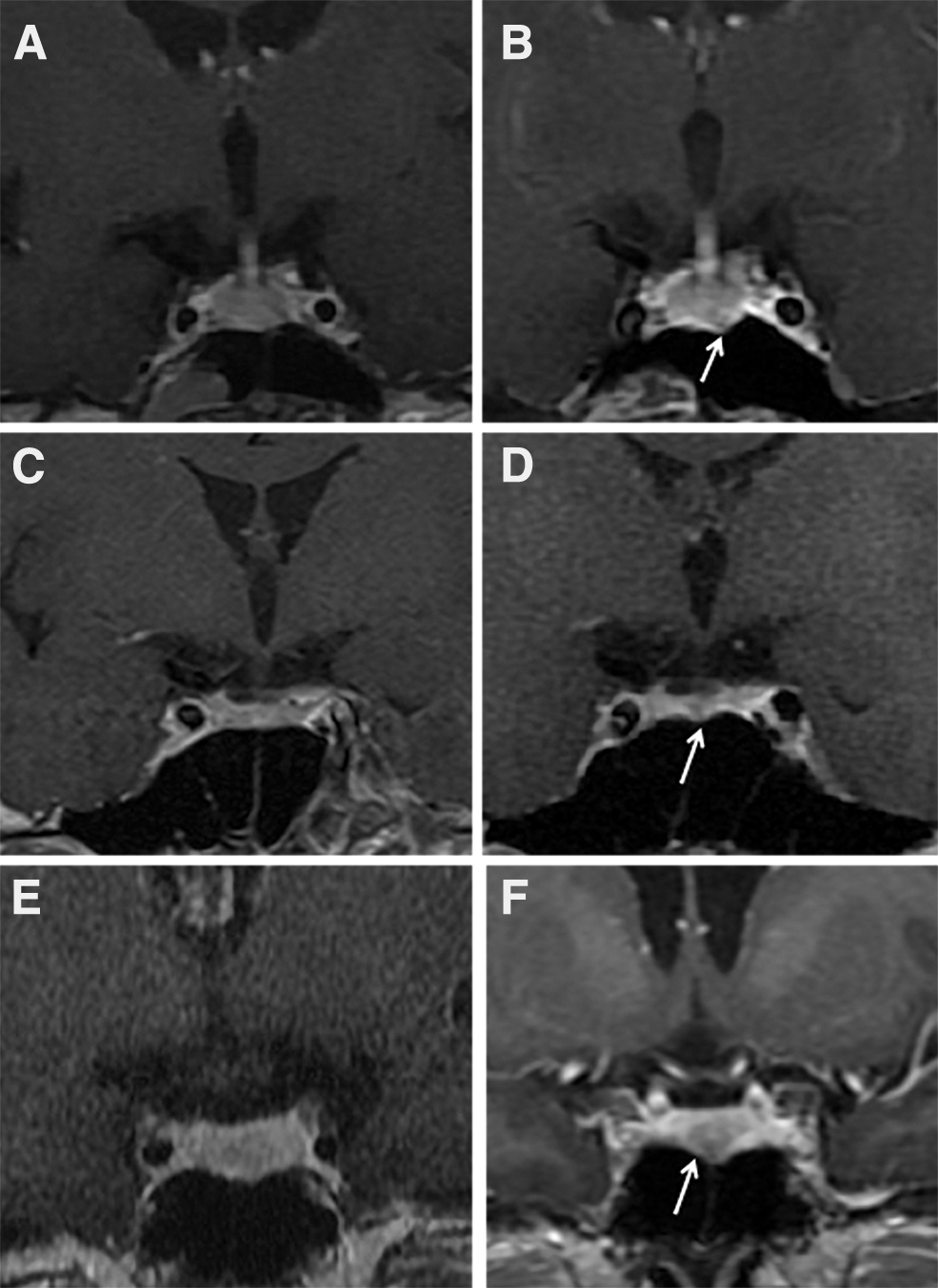
MRI follow-up showed positive findings in three patients with double negative IST (white arrow). (
Application in Special Cases in Inappropriate Secretion of Thyrotropin Patients with Negative Image Finding and Thyroid Hormone Receptor Beta Mutation or Mixed Hormone Secreting
GH; mo, months; PRL.
Two patients were found to have microadenomas with mixed hormone imbalance. The SSA test showed a negative response. One patient became euthyroid after surgery and the histology findings confirmed a mixed PRL/TSH adenoma. The other patient had persistent IST after surgery and only GH stained positively in the removed tumor (Supplementary Table S3).
Comparison of the short-term SSA and TRH test
A total of 25 patients in the training group underwent both a TRH and a short-term SSA test. The TRH test detected 16/19 patients with a TSHoma, while the SSA test detected 17/19 patients with a TSHoma. All RTHβ patients were detected by both tests (Supplementary Table S4). Five TSHoma patients showed inconsistent results: three patients (two macroTSHomas and one microTSHoma) were only detected by the SSA test; two patients (one macroTSHoma and one microTSHoma) were only detected by the TRH test.
Discussion
In the present study, we established a short-term SSA test to accurately and efficiently diagnose TSHomas and differentiate them from other causes of IST. The test requires three injections of Sandostatin within 24 hours. Most importantly, the test could identify TSHomas even before positive findings on pituitary imaging were apparent.
Physiologically, SSA inhibits TSH and TRH release through SSTRs, especially SSTR2 and 5, which are expressed in TSH- and TRH-producing cells (14,15). TSHomas have a higher SSTR expression than normal thyrotrophs (16 –18). SSAs are being used to treat, but rarely to diagnose TSHomas. A long-term SSA test has been proposed by Mannavola et al. in 2005 (8), which was based on a marked decrease of TH but not TSH levels in patients with TSHomas. Other studies showed a similar TSH decrease in patients with TSHomas and RTHβ after a single dose of SSA injection (7,8,19). In the present study, we determined serial TSH levels after injection of an SSA and noticed that the 2-hour time point was informative: The TSH level in TSHoma patients decreased consistently and showed a near linear relationship with the SSA dose, but it barely changed in RTHβ patients after 2 hours (16). Generally, hormone secretion by exocytosis can be blocked acutely, while hormone synthesis can be blocked chronically by inhibiting mRNA transcription, protein synthesis, as well as secondary protein modifications (20). It has been reported that the dominant effect of SSAs on pituitary function is due to acute inhibition of hormone exocytosis. We believe that the decrease in the TSH level observed at 2 hours in the SSA test reflects a rapid decrease in exocytosis in patients with TSHomas and RTHβ. Chronically, SSA can bind SSTR2/5 and regulate TSH synthesis by the adenylyl cyclase-cAMP-PKA pathway. TSHomas have a higher expression of SSTR2/5 than normal thyrotrophs. Therefore, repeated SSA injections may suppress the cAMP levels to a greater extent and thereby result in a sustained TSH reduction in TSHoma patients, whereas this effect is less significant in RTHβ patients. Other possibilities may involve SSTR phosphorylation, internalization, and desensitization, which are crucial mechanisms that prevent persistent stimulation in normal thyrotrophs. In TSHomas, these regulatory mechanisms may be compromised.
Based on the results presented here, we propose a diagnostic test based on the suppression ratio of TSH at 24 versus 2 hours instead of using the absolute TSH level at 24 hours or the suppression ratio of TSH at 24 versus 0 hours. The diagnosis of a TSHoma requires a suppression ratio that is greater than 44.46%. This diagnostic test achieved a sensitivity of 95.00% and specificity of 93.75% in the training cohort. More importantly, the PPV of histologically confirmed microTSHoma was 100% in the validation cohort.
Distinguishing microTSHomas from other causes of IST has become more challenging because of the increasing use of ultrasensitive immunometric TFT assays and pituitary imaging (21). An increasing number of TSHomas have been diagnosed in the last three decades, 39.3% as microTSHomas (22). Moreover, a previous study showed that 18.7% of patients with IST without THRB mutations developed TSHomas during follow-up (5). Differentiating between TSHomas and RTHβ can be challenging (23 –25). The PPV was 100% in our validation cohort of microTSHomas. Interestingly, for IST patients with negative pituitary findings and negative for germ line mutations in the THRB gene, three showed a positive response and all developed microTSHomas during follow-up. Our short-term SSA test therefore appears to be an accessible method to diagnose microTSHomas, and to identify them at a very early stage when imaging findings were still negative.
There are limitations to the SSA test presented here. It seems that the SSA test performed poorly in TSHomas with mixed hormone secretion. One patient with a mixed PRL/TSH adenoma showed a negative response to the short-term SSA test. This may probably be explained by the unbalanced expression of different receptors in these tumors. It has been reported that mixed pituitary adenomas show a poor response to SSA treatment (17,26,27) due to high expression of dopamine receptors and low expression of SSTRs (17). It should be noted that only patients with an intact thyroid were recruited in our study and antithyroid drugs should be withdrawn for at least 1 month before performing the SSA test. Moreover, the diagnostic cut point of the SSA test needs to be optimized because of the limited number of participants, especially those with microTSHomas. Long-term follow-up is required for IST patients with negative pituitary findings and absent germ line mutations in the THRB gene.
In summary, the present study successfully established a short-term SSA test to distinguish TSHomas from other entities with IST, which is especially helpful when diagnosing microTSHomas or undetectable TSHomas. For patients with a positive SSA response, we suggest pituitary surgery if the patient has an adenoma and close follow-up if the patient has negative imaging findings. However, due to the limited number of patients with RTHβ in the validation group, studies including a larger number of patients with RTHβ are needed to confirm our findings.
Footnotes
Acknowledgments
We thank all the patients who participated in this study, and all the health care professionals who treated these patients.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was sponsored by grants from the National Key Research and Development Program of China (2016YFC0901503), the National Science Foundation of China (81570702, 81400772, 81700686), the Foundation of Health and Family planning Commission of Shanghai (20174Y0204), and the National International Science Cooperation Foundation (2015DFA30560). The sponsor of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the article. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4