
Abstract
Background:
Patient preferences pertaining to surgical options for thyroid cancer management are not well studied. Our aim was to conduct a discrete choice experiment (DCE) to characterize participants' views on the relative importance of various risks and benefits associated with lobectomy versus total thyroidectomy for low-risk thyroid cancer.
Methods:
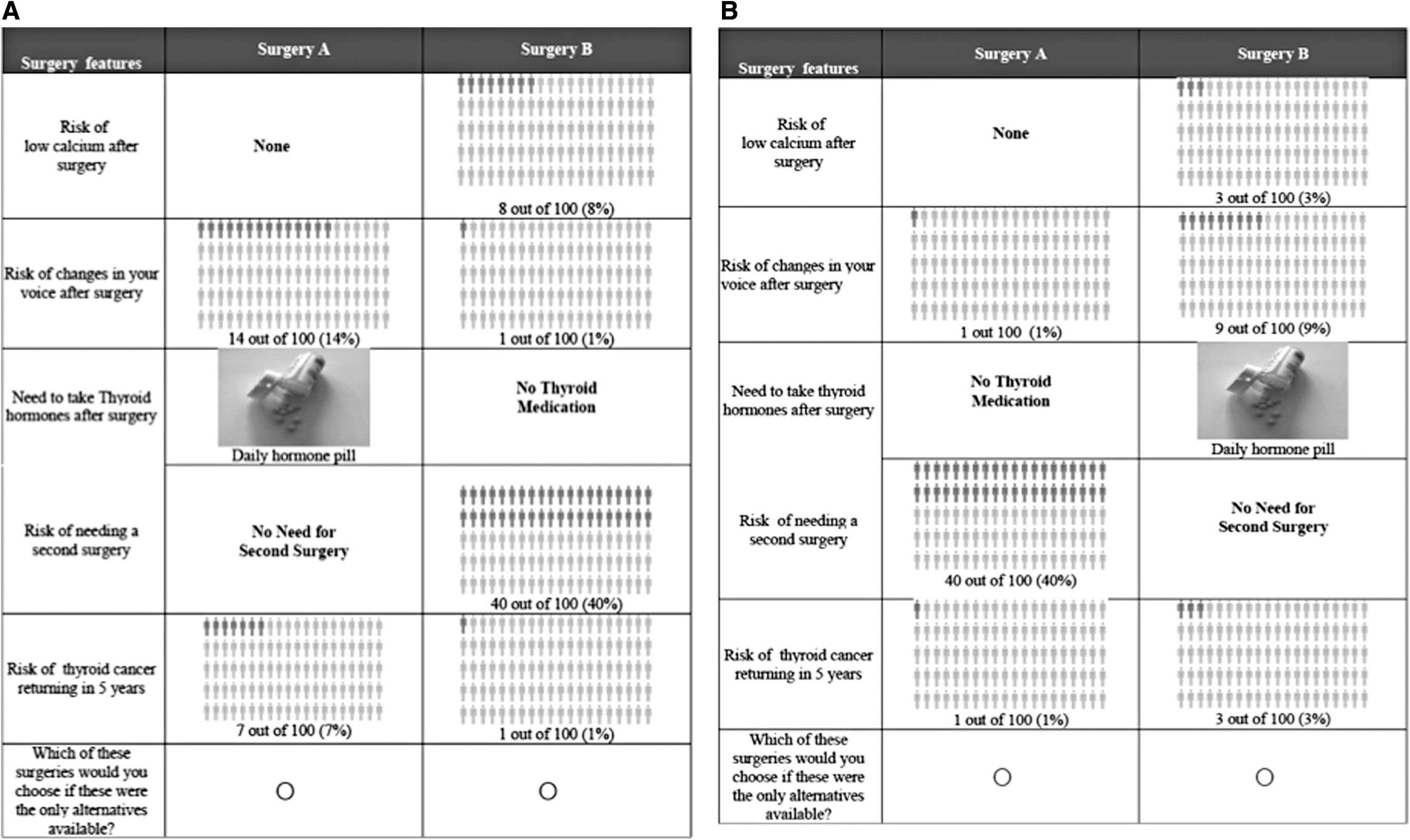
Adult participants with low-risk thyroid cancer or a thyroid nodule requiring surgery were asked to choose between experimentally designed surgical options with varying levels of risk of nerve damage (1%, 9%, 14%), hypocalcemia (0%, 3%, 8%), risk of needing a second surgery (0%, 40%), cancer recurrence (1%, 3%, 5%), and need for daily thyroid hormone supplementation (yes, no). Their choices were analyzed using random-parameters logit regression.
Results:
One hundred fifty participants completed an online DCE survey. Median age was 58 years; 82% were female. Twenty-four participants (16%) had a diagnosis of thyroid cancer at the time of completing the survey, and 126 (84%) had a thyroid nodule necessitating surgery. On average, 35% of participants' choices were explained by differences in the risk of cancer recurrence; 28% by the chance of needing a second surgery; 19% by the risk of nerve damage; and 9% by differences in risks of hypocalcemia and the need for thyroid hormone supplementation. When accounting for differences in postoperative risks, the average patient favored lobectomy over total thyroidectomy as long as the chance of needing a second (i.e., completion) surgery after initial lobectomy remained below 30%. Participants would accept a 4.1% risk of cancer recurrence if the risk of a second surgery could be reduced from 40% to 10%.
Conclusions:
While patients with thyroid cancer may have clear preferences for extent of surgery, common themes moderating preferences for surgical interventions were identified in the DCE. Adequate preoperative evaluation to decrease the chance of a second surgery and providing patients with a good understanding of risks and benefits associated with extent of surgery can lead to better treatment decision-making.
Introduction
Thyroid nodules and thyroid cancer are common clinical problems. High-resolution ultrasound can detect thyroid nodules in 19–68% of randomly selected individuals, with higher frequencies in women and older adults (1,2). Thyroid cancer occurs in 7–15% of cases of thyroid nodules, depending on patient age, sex, radiation exposure history, family history, and other factors (3,4). In the United States, the yearly incidence of thyroid cancer has nearly tripled, from 4.9 per 100,000 in 1975 to 14.3 per 100,000 in 2009. One study predicted that by 2019, papillary thyroid carcinoma (PTC) would become the third most common cancer in women, at a cost of $19–21 billion in the United States (5). Another study has predicted that thyroid cancer will replace colorectal cancer as the fourth leading cancer diagnosis by 2030 in the United States (6).
Surgery represents the mainstay of initial treatment for thyroid cancer. The extent of surgery for low-risk thyroid cancer includes thyroid lobectomy or total thyroidectomy. The American Thyroid Association (ATA) practice guidelines in 2009 endorsed total thyroidectomy as the primary initial surgical treatment option for all patients with differentiated thyroid cancer >1 cm, with or without evidence of locoregional or distant metastases (7). This recommendation was largely based on a single study by Bilimoria et al. published in 2007, which suggested that a survival benefit was afforded by total thyroidectomy compared with lobectomy (8). This finding was surprising since outcomes following standard treatment for most differentiated thyroid cancer are almost uniformly excellent, and long-term disease-specific survival among most differentiated thyroid cancer patients is 98%. However, more recent studies have demonstrated noninferior survival when comparing total thyroidectomy versus thyroid lobectomy in properly selected patients with thyroid cancer (9 –13).
Thyroid lobectomy is associated with fewer complications (hypoparathyroidism, recurrent laryngeal nerve injury resulting in hoarseness, or tracheostomy), less use of thyroid hormone, and superior health-related quality of life (14 –16). This has raised the concern that in patients with low-risk differentiated thyroid cancer, traditional treatment with total thyroidectomy might result in harm without added benefit. The revised ATA guidelines in 2016 recommended that thyroid lobectomy alone may be sufficient treatment for patients with low-risk papillary and follicular thyroid cancers with a negative family history of thyroid cancer and negative personal history of radiation exposure (5). In the end, there is clinical equipoise between thyroid lobectomy and total thyroidectomy for the indication of low-risk differentiated thyroid cancer based on the scientific evidence.
In the case of differentiated thyroid cancer, many patients may overestimate the mortality implications of thyroid cancer (17). These misperceptions may drive patients' willingness to undergo more invasive treatments. However, it is unknown to what extent patients with thyroid cancer may favor the benefit–risk trade-offs that are representative of thyroid lobectomy (less aggressive) versus total thyroidectomy (more aggressive).
To date, few studies have investigated patient preferences for thyroid cancer treatment options despite their relevance for a disease with <5% mortality. To the best of our knowledge, there are only three published studies using a discrete choice experiment (DCE) approach to quantify patients' trade-offs around thyroid cancer management (17 –19), but those studies did not focus on outcomes related to trade-offs between partial and total thyroidectomy.
DCEs have increasingly been used to examine determinants of patients' preferences for aspects of their health care. In a DCE, individuals are asked to consider two or more hypothetical interventions and to choose the one that is preferable to them based on the features of the alternatives. Their selections allow researchers to investigate trade-offs among positive and negative features of the interventions. In oncology, these features may include trade-offs between additional survival afforded by a treatment and its potential risks, side effects, inconveniences, or costs.
Patient–physician communication about thyroid cancer outcomes and available treatment options plays a vital role in the patients' understanding of their diagnosis. We hypothesized that for low-risk thyroid cancer, many patients would be willing to accept less aggressive surgery (lobectomy) in exchange for lower treatment-related risks, such as hypoparathyroidism or nerve injury, and the need for lifelong thyroid hormone replacement or supplementation.
To test this hypothesis, we designed a DCE survey to be administered in a cohort of patients with newly diagnosed differentiated thyroid cancer or thyroid nodules requiring surgery to: (i) determine which trade-offs they would be willing to make to balance the benefits and harms of thyroid lobectomy versus total thyroidectomy and (ii) quantify which trade-offs among side effects, risks of adverse events, and clinical benefit associated with alternative surgical management strategies (total thyroidectomy vs. thyroid lobectomy) are acceptable to them.
Methods
Candidate features (attributes), including key cancer outcomes, treatment-associated risks, and side effects (Table 1), were selected and defined by a review of the literature and discussions with clinical experts. Attribute levels were used to characterize the performance of hypothetical surgical interventions. Levels were selected to represent ranges of treatment-related risks (i.e., surgical complications), need for thyroid hormone replacement, need for a second surgery (i.e., completion thyroidectomy after initial lobectomy, based on surgical pathology), and disease recurrence estimates reported in the literature to evaluate which recurrence risks participants were willing to accept for various levels of reduction in treatment-associated complications.
Candidate Attributes
This study consisted of two phases: (i) survey development and (ii) recruitment (Fig. 1).

Study phases.
After selecting the attributes and drafting the initial version of the survey, we conducted face-to-face pretest interviews with eight participants with thyroid nodules/thyroid cancer, employing a think-aloud protocol to explore the thought processes and reasoning behind participants' responses. An initial five-respondent group completed a paper version of the survey during the pretest interviews and provided verbal feedback on the survey instrument. Based on this feedback, we revised the survey instrument to improve understandability and reduce cognitive burden. We conducted a second round of pretest interviews with three more participants after revising the survey. No significant changes were required after the second set of pretest interviews.
The final version of the survey was programmed and administered by Sawtooth Software (Sawtooth Software, Inc., Provo, UT) (20). The DCE survey queried participants to choose between pairs of hypothetical management options to treat thyroid cancer (Fig. 2A, B). Before asking participants to complete the DCE, the survey instrument provided educational information about management options, including a description of total thyroidectomy and lobectomy. Educational information was provided about the attributes used to characterize treatment and health outcome features associated with thyroid surgery. Following the educational section in the survey instrument, participants completed a series of choice questions. The combinations of attribute levels shown across the choice questions were designed experimentally, so statistical methods could be used to identify participants' relative preferences for changes in attribute levels based on their choices. The combinations of attribute levels followed an orthogonal design with 300 questions prepared using the Sawtooth Software (Sawtooth Software, Inc.) (20). Orthogonality minimized the correlations between attribute levels in the choice questions and balanced the number of levels presented across attributes. To reduce respondent fatigue, each respondent was asked to complete a subset of six choice questions. The specific subset of questions was randomized across participants. Also, baseline patient characteristics, including age at diagnosis, thyroid function, radiation exposure, and family history of cancer, were collected.
(
Study inclusion criteria were adult participants ≥18 years diagnosed with differentiated intrathyroidal thyroid cancer <4 cm with no clinical evidence of locoregional disease and lymphadenopathy or a thyroid nodule requiring surgery due to: (i) compressive symptoms; (ii) indeterminate cytology with worrisome ultrasound features; or (iii) indeterminate cytology with abnormal molecular testing, presenting for surgical consultation at a tertiary/quaternary academic medical center. Participants with a thyroid nodule were asked to imagine that they were recently diagnosed with thyroid cancer for the purpose of the study. The treating team identified participants as being eligible and invited them to participate in the study. We excluded patients with intermediate- and high-risk cancers since total thyroidectomy has been demonstrated to confer benefit over thyroid lobectomy in those clinical scenarios.
In the main phase of the project, enrolled participants who consented to participate completed the survey on a tablet in the clinic before or after their visit with the physician. No identifying information linked the passwords to the patients who participated in the survey, and no protected health information was collected in the survey. This study was approved by the Duke University Institutional Review Board.
Statistical analysis
Data on participants' preferences for thyroid surgery were analyzed in StataSE 15 (StataCorp, 2017, Stata Statistical Software: Release 15; StataCorp LLC, College Station, TX) and fitted using a random-parameters logit (RPL) model. In the RPL model, participants' choices were regressed against the characteristics of the treatment alternatives presented (20,21). The dependent variable was binary, with 1 and 0 representing the surgery chosen and not chosen, respectively, in each choice question. The independent variables covered the attribute levels listed in Table 1. These variable were effect-coded so that an omitted category in each attribute was set to be the negative sum of all other attribute levels. Contrary to dummy-coding, effect coding allows the identification of coefficients for all attribute levels. However, effect-coded coefficients indicate deviations from the mean effect of the attribute instead of deviations from an omitted attribute level with dummy coding (22).
We derived three measures of preferences from the RPL model: Preference weights—indicate how each attribute level affects participants' treatment choices (relative to the attribute mean effect), all else being equal (21); Overall attribute importance—indicates the impact that changes in attribute levels have on treatment choices; and Attribute equivalence—indicates changes in two attributes that have the same magnitude of effect on treatment choices.
We characterized preference heterogeneity by leveraging the fact that each respondent answered multiple choice questions. Repeated choices made possible the estimation of a cross-respondent distribution of preference weights. We assumed that the weights were normally distributed across participants and estimated a standard deviation for each distribution.
Preference weights
Coefficients from the RPL model are log-odds indicating the effect that the attribute levels have on treatment choice relative to the attribute mean effect. For this reason, the log-odds are also known as preference weights. Log-odds can be difficult to interpret because they represent relative effects. To facilitate interpretation, rescaling was used to accomplish two things:
Set the attribute levels corresponding to the best clinical outcomes to zero, and
Normalize all preference weights to lie between 0 and −10.
Point number 1 made it possible to interpret the preference weights for all attribute levels relative to the best outcomes. For example, a negatively rescaled preference weight for a given attribute level is interpreted as a reduction in preferences for treatments with that attribute level when compared with a treatment with the best level shown for the attribute. Point number 2 gives the preference weights consistent interpretation across attributes; for example, a preference weight of −6 for one attribute level can be interpreted to be twice as impactful as a preference weight of −3 for a different attribute.
For the rescaling, we first took the difference between the largest and smallest coefficients within attributes in the RPL model. Then, we normalized the differences on a scale between −10 and 0, where −10 was assigned to the worst level of the most important attribute, and 0 was assigned to the best level of each attribute. See attribute-based normalizations in Gonzalez (23) for a detailed description of the steps followed and the rationale for these steps.
Overall attribute importance
Overall attribute importance refers to the maximum difference in preference weights within an attribute given the attribute levels in the study. As with preference weights, we normalized overall attribute importance to facilitate their interpretation. First, we calculated the greatest difference in the normalized preference weights across levels for each attribute. We then added these differences and calculated what proportion of the sum was associated with each attribute (23). With this normalization, overall attribute importance conveys how much of the difference in preferences between two treatments can be attributed to a specific attribute.
We estimated confidence intervals [CIs] around the preference weights and overall importance weights using the Krinsky–Robb procedure with 10,000 draws and then rescaled accordingly (24). If the CIs between attributes do not overlap, the importance weights are statistically significantly different from each other at better than the 95% confidence level.
Attribute equivalence
We used the normalized preference weights to calculate the increase in the 5-year risk of recurrence that would offset changes in treatment choices induced by reductions in the risk of hypocalcemia after surgery, risk of voice changes after surgery, and the risk of needing a second surgery to eliminate the cancer. To obtain these equivalences, we calculated the changes in preference weights associated with all reductions in the risk of hypocalcemia, voice changes, and the need for second surgery included in the study. Then, we determined the increase in the 5-year risk of recurrence (from 1%, the lowest level of recurrence risk in the study) that would exactly offset improvements in the likelihood of choosing a treatment with each risk reduction (25).
Comparing thyroid lobectomy and total thyroidectomy
Finally, coefficients from the RPL model were used to examine to what extent the average patient would prefer a thyroid lobectomy over a total thyroidectomy. For this exercise, the thyroid lobectomy profile was described as a 0% of risk of hypocalcemia after surgery; a 1% risk of voice change after surgery; a 50% risk of requiring daily thyroid hormone supplementation; and a 3% risk of thyroid cancer recurrence in 5 years. The total thyroidectomy profile was defined as: a 3% risk of low calcium after surgery; a 9% risk of voice change after surgery; a 100% chance of daily thyroid hormone therapy; and a 3% risk of thyroid cancer recurrence in 5 years. Using the preference weights that corresponded to each of these attribute levels, we then proceeded to calculate the risk of additional surgery that would make lobectomy and thyroidectomy equally acceptable to patients.
Results
One hundred fifty adult participants completed the DCE; median age was 58 years, and 82% were female. Twenty-four participants (16%) had a diagnosis of thyroid cancer at the time of completing the survey, and 126 (84%) had a thyroid nodule necessitating surgery. One hundred six (71%) participants completed the survey before their visit with the clinical team; 64 (43%) had a positive family history of cancer in their first-degree family, 14 (9%) had a history of head and neck radiation, 25 (17%) reported a history of hyperthyroidism, 23 (15%) a history of hypothyroidism, and 32 (21.0%) reported to be on thyroid medication at the time of the study (Table 2).
Patient Characteristics (N = 150)
Figure 3 represents the rescaled preference weights from the RPL model (Supplementary Table S2). Following the aforementioned normalization, the best clinical levels in each attribute were significantly more preferred to all other attribute levels (i.e., the highest preference weight in each attribute is zero). All other levels in each attribute were well ordered; that is, better clinical outcomes were preferred to worse outcomes. Specifically, participants preferred lower risks associated with surgical complications, no need for thyroid hormone therapy, and lower risks of a second surgery and cancer recurrence. Within each attribute, adjacent levels were statistically significantly different (p < 0.05).

Preference weights (N = 150). The dots represent the estimated preference weights for the attribute levels. The vertical bars around the preference weights indicate the 95% confidence intervals for the estimates.
Given the attributes and attribute levels considered in the study, 35% of participants' choices were explained by the difference in the risk of thyroid cancer recurrence between the two surgical options, 28% by the risk of requiring a second surgery, 19% by the risk of recurrent laryngeal nerve damage, and 9% by the risk of hypocalcemia or the need for thyroid hormone supplementation/replacement (Fig. 4).
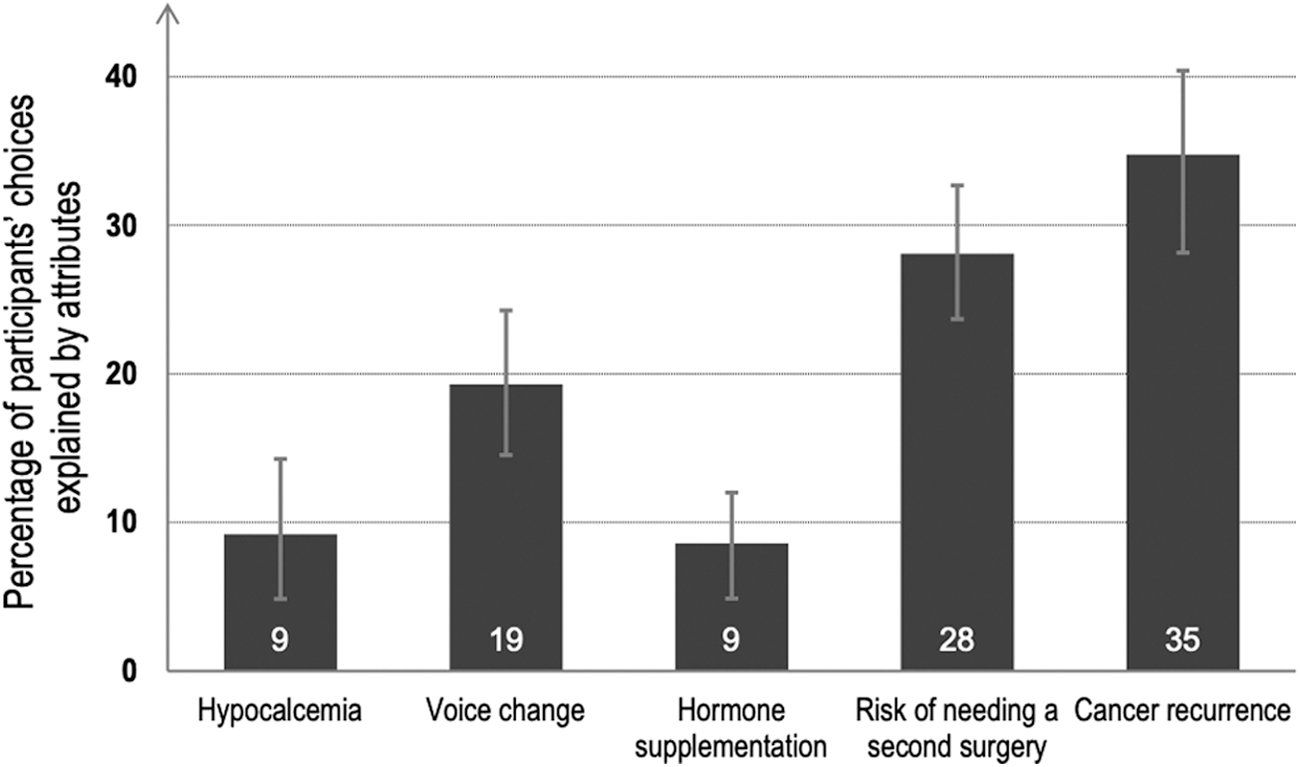
Overall attribute importance in treatment choices.
Attribute equivalence was calculated as the willingness to accept an increase above 1% in the 5-year risk of thyroid cancer recurrence. Participants would accept a 4.1% risk of thyroid cancer recurrence if the risk of a second surgery could be reduced from 40% to 10%. Participants would accept a 1.6% risk of thyroid cancer recurrence if the risk of hypocalcemia could be reduced from 3% to 0%, and a 2.6% risk of thyroid cancer recurrence if the risk of change in voice could be lowered from 9% to 1% (Table 3).
Risk–Risk Trade-off
CI, 95% confidence interval.
After accounting for differences in postoperative risks and the expected differences in the outcomes associated with thyroid lobectomy and total thyroidectomy, our results suggest that the average patient would be indifferent between a thyroid lobectomy and total thyroidectomy if the risk of needing a second surgery after lobectomy could be reduced to 30%. Thus, participants in our sample would be expected to start favoring a thyroid lobectomy over total thyroidectomy if the chance of necessitating a completion thyroidectomy was <30% (or about less than 1 in 3 patients).
Discussion
We designed a DCE survey for a cohort of patients with newly diagnosed differentiated thyroid cancer or thyroid nodules necessitating surgery to determine which trade-offs they would be willing to accept among the benefits and harms of thyroid lobectomy versus total thyroidectomy. We were able to quantify the impact that clinical benefits, treatment side effects, and risks of adverse events have on patient preferences that pertain to surgical management strategies for thyroid cancer.
On average, given the risk levels shown across DCE choice questions, the risk of thyroid cancer recurrence impacted participants' preference for treatment options the most, followed by the risk of needing a second surgery, and the risk of voice change due to damage to the recurrent laryngeal nerves during surgery. Risk of hypocalcemia and the need for thyroid hormone replacement had the least impact on participants' preference for treatment options. After accounting for specified differences in postoperative risks for lobectomy and total thyroidectomy, the average patient would prefer a total thyroidectomy over thyroid lobectomy unless the chance of needing a second surgery after a lobectomy could be reduced to 30% or less. When trading benefits against harms, participants were willing to accept on average a 4.1% risk of thyroid cancer recurrence if the risk of a second surgery after a thyroid lobectomy could be reduced from 40% to 10%. On average, participants also were willing to accept up to 3.7% risk of thyroid cancer recurrence to eliminate the risk of voice changes and up to 2.2% to eliminate the chance of hypocalcemia.
DCEs have been applied in other cancers, including ovarian, melanoma, lung, colon, and breast cancers (26 –30), to evaluate benefit–risk trade-offs with various treatments. To the best of our knowledge, there are only three studies using a DCE approach to quantify patients' trade-offs in thyroid cancer. Mohamed et al. designed a DCE to identify patients' preferences for different adjuvant cancer treatments for radioactive iodine-refractory thyroid cancers (18). Nickel et al. designed an online DCE survey to study patients' preferences with regard to available treatment options of thyroid neoplasms based on the actual terminology used (PTC or papillary thyroid lesion). In this study, when the condition was described as cancer, participants were more willing to accept potential treatment risks with more aggressive treatments. This demonstrated that the terminology used to describe papillary thyroid cancer in conversations with patients can impact their treatment decision-making (19). Similarly, Dixon et al. designed a DCE to determine whether disease “labels,” such as cancer, tumor, or nodule, would impact patient's decision-making in the treatment of low-risk PTC. This study also showed that the cancer label profoundly impacted the participants' treatment choices (17).
The most recent ATA guidelines recommended either thyroid lobectomy or total thyroidectomy for patients with low-risk thyroid cancer (unifocal differentiated thyroid cancer <4 cm, with no evidence of extrathyroidal extension or lymph node metastases), given that multiple studies have found noninferior overall survival for patients undergoing thyroid lobectomy versus total thyroidectomy (11 –13,31). A more selective use of radioactive iodine, greater reliance on neck ultrasound, and serial serum thyroglobulin level measurement for detection of thyroid cancer recurrence have decreased the necessity for total thyroidectomy in low-risk thyroid cancer patients. This has led to a change in clinical practice since the publication of these guidelines (32,33). A study of 35,291 patients using the National Surgery Quality Improvement Program data showed a 10-fold increase in the rate of thyroid lobectomy after the publication of the 2016 ATA guidelines (32). However, no study has examined patients' preferences concerning surgical treatment options. Our study is the first study to examine patients' preferences pertaining to the extent of surgery for low-risk thyroid cancer.
The study presented here shows that after accounting for differences in postoperative risks, the average patient would prefer total thyroidectomy over lobectomy unless the chance of needing a second surgery following a lobectomy is 30% or less. This emphasizes the importance of proper selection of patients for thyroid lobectomy and appropriate preoperative evaluation aimed to decrease the chance of necessitating a completion thyroidectomy.
Some limitations of this study should be acknowledged. While the study used an orthogonal experimental design to populate the alternatives in the DCE, it was not powered to test for variations in preferences between subgroups of participants. Nevertheless, to rule out distinct differences in preference patterns between subgroups, we performed post hoc likelihood ratio tests. These tests failed to show significantly different preferences between participants with cancer versus without a cancer diagnosis; between participants who completed the DCE survey before or after their consultation; and between participants who were taking versus not taking daily thyroid hormone (Supplementary Table S1).
Another limitation is that participants were evaluating hypothetical scenarios, and it is possible that their actual treatment decisions would have differed. Potential reasons could include intentional or unintentional influence of a clinician's presentation of treatment options, or a patient's clinical characteristics that impacted their personal risks of disease recurrence or adverse events. Also, participants may answer hypothetical treatment questions differently than if they were facing a decision with real consequences. However, we attempted to minimize issues associated with the hypothetical nature of the experiment by developing an instrument that used a realistic clinical decision context and attribute descriptions that simulate the same level of information that clinicians provide to patients in this situation. The rigorous qualitative pretesting of the instrument indicated that participants understood the attributes and choice questions and made treatment selections that were consistent with their personal preferences. To the extent that a small proportion of patients considering lobectomy or total thyroidectomy already have experience taking daily thyroid hormone and this experience influences their preferences, our findings may well be reflective of the target population.
In conclusion, patients' preferences for thyroid lobectomy or total thyroidectomy will vary depending on the combinations of risks and benefits of both procedures that apply to the individual patient. Excellent patient–physician communication is important for providing patients with a good understanding of the risks and benefits associated with the extent of surgery. There have been significant changes in clinical practice since the publication of the 2016 ATA guidelines, and these warrant understanding and consideration of each patient's preferences on the relative benefits and risks of alternative treatment options. The physician consultation coupled with educational decision aids can help to ensure that patient's preferences are grounded with accurate information and to facilitate shared decision-making. Additional studies should include testing patients' preferences before and after their initial surgical consultation, as well as more diverse patient populations across different types of institutions.
Footnotes
Author Disclosure Statement
J.A.S. is a member of the Data Monitoring Committee of the Medullary Thyroid Cancer Consortium Registry supported by Novo Nordisk, GlaxoSmithKline, Astra Zeneca, and Eli Lilly.
Funding Information
This study was funded by the Duke Cancer Institute.
Supplementary Material
Supplementary Table S1
Supplementary Table S2