
Abstract
Background:
Lung metastasis from differentiated thyroid cancer (DTC) in children and young adults (CAYA) is estimated at 25%, which is 3–4 times higher than in adults. Lung metastases may respond to radioactive iodine (RAI) therapy and overall survival is excellent. Associations with lung metastasis include lateral lymph node (LN) disease although CAYA data are limited. We investigated factors associated with lung metastasis in children and adolescents and described their presentation and outcome.
Methods:
A retrospective review of medical records from 1998 to 2017 in patients aged <18 years treated at a tertiary pediatric center was carried out. Data on age, clinical features at diagnosis, histology, biochemistry, imaging, RAI therapy, and outcome were collected.
Results:
Patients treated for DTC totaled 98 and 19 of 98 (19%) patients had lung metastasis; 17 of 19 (89%) patients were identified within 6 months from thyroidectomy. Patients with lung metastasis were younger (p < 0.001)—40% <13 years old had lung metastasis—and had a larger primary tumor diameter (p = 0.01). Absence of LN disease had negative predictive values ≥90% (p < 0.02). Patients with lung metastasis had a higher postoperative thyrotropin-stimulated thyroglobulin (Tg) (p < 0.001), ≥2 ng/mL in 10 of 11 (91%) patients, and 100% had an elevated preoperative Tg (>60 ng/mL). Post-therapy whole body scan (WBS) identified most metastasis (13 of 17 patients), which were mostly diffuse (11 of 19 patients). Discordant findings were found between WBS and computed tomography (CT) at diagnosis (2 patients), WBS and CT during surveillance (3 patients), and diagnostic and post-therapy WBS (2 patients). Final outcome was “excellent” in 3 of 19 (16%) patients, “biochemically persistent” in 1 of 19 (5%) patients, “structurally persistent” in 13 of 19 (68%) patients—including 1 death—and indeterminate in 2 of 19 (11%) patients. Postoperative Tg correlated with response to therapy. Lung metastasis pattern and RAI cumulative activity were not predictive of response to therapy.
Conclusions:
Lung metastases are mostly observed at diagnosis of DTC and higher suspicion should be maintained in CAYA who are younger, have LN disease, and have elevated postoperative Tg. Preoperative Tg shows promise as another predictive marker, but limited sample size precludes generalization. “Excellent” response to therapy is uncommon—multiple RAI courses do not necessarily improve outcome—response appears unrelated to RAI activity or metastasis pattern.
Introduction
Differentiated thyroid cancer (DTC) is rising in incidence and, although less common than in adults, it is the most common endocrine cancer in children (1,2). Recent guidelines recognize that DTC behaves differently in children and provide the first pediatric-focused approach to thyroid cancer management (3). Lung metastases are reported in up to 25% of children and young adults (CAYA) <21 years with DTC (4 –8)—a substantially higher proportion than in adults. Overall, children with DTC have a highly favorable prognosis (9). The prognosis from lung metastasis is better for younger adults and for CAYA; overall survival exceeds 95% at 10 years (5,6,10 –13).
CAYA with lung metastases can be responsive to radioactive iodine (RAI) therapy (5,12,14,15); however, the response varies greatly (anywhere between 0% and 70% achieving a complete response). Individual CAYA cohorts are small and definitions of response to RAI lack uniformity (4,5,15 –17). Locoregional lymph node (LN) metastasis and elevated postoperative thyroglobulin (Tg) are predictors of lung metastasis in CAYA; however, these findings reflect data from a limited number of small cohorts (6,7,12). Outcome of therapy for lung metastasis has been associated with the timing of lung metastasis diagnosis and pattern of metastases on imaging; however, these studies include predominantly adult patients (13,16,18,19).
Cohorts of CAYA with lung metastases from DTC are relatively small compared with adult series and incorporate little data from the most recent decade since new guidelines were introduced (3,4,7,17,20). In this study, we asked what factors are associated with lung metastasis in CAYA, how do they present, and how do they respond to RAI therapy? We report a retrospective analysis of our pediatric patients with DTC for a 20-year period, comparing those with and without lung metastases, and describe the presentation and outcome of those with lung metastases. Our findings identify factors that assist clinicians to distinguish patients in whom to suspect lung metastases, possible discordance between imaging modalities, and considerations for counseling patients with lung metastases in clinic.
Methods
This was a retrospective chart review of all patients, under the age of 18 years, who were treated at our institution for DTC between 1998 and 2017. Data were available for 98 patients whose treatment was either initiated at our institution or who were referred for second opinion after treatment had been initiated elsewhere. Five patients with incomplete staging were excluded. This study was approved by the institutional research ethics board and consent was waived due to the retrospective design.
Clinical, biochemistry, imaging, and pathology data were extracted from patients' electronic medical records.
Assays and imaging
Tg and antithyroglobulin (anti-Tg) were measured using the Roche Modular Analytics E170 system between 2015 and 2018; before this time, alternative assays were used. Six to 8 weeks postoperatively, a diagnostic whole body scan (WBS) was performed 20–24 hours after oral administration of 123I (maximum 0.3 mCi). Post-therapy WBS was performed seven days after therapeutic 131I was administered orally. Subsequent surveillance WBS was performed 48 hours after 1–4 mCi 131I was administered orally. Scintigraphy was performed using a dual-head Millennium MG camera (Milwaukee, WI) as described previously (21).
Clinical management
Over the study period, the approach to managing DTC has evolved (22,23); 7 of 98 patients (4 of 19 patients with lung metastases) were diagnosed before the first protocol for managing DTC in 2006 was consolidated at our institution (22), and 65 of 98 patients were diagnosed with DTC (14 of 19 patients with lung metastasis) before 2015 when the first international guidelines for managing thyroid nodules in children were published (3). In general, before the 2015 guidelines, a more conservative approach to DTC management was employed at our institution, with a greater reliance on nuclear imaging and near-universal application of RAI therapy (24). During this period (2006–2015), routine surveillance for all patients included semiannual basal Tg, anti-Tg, and cervical ultrasonography, and annual diagnostic WBS.
Outcome definitions
All nuclear imaging was reviewed by a single nuclear medicine physician (R.V.) and the pattern of lung metastasis was categorized as diffuse, focal, or multifocal. The primary tumor (T), LN (N), and distant metastasis (M) classifications were documented according to the American Joint Committee on Cancer Staging Manual, seventh edition (23). Response to therapy was defined as “excellent,” with basal (unstimulated) Tg <1 ng/mL or thyrotropin-stimulated Tg (sTg) <2 ng/mL (with normal anti-Tg titers) and no structural disease on imaging; biochemical persistence, with abnormal biochemistry and no structural disease; structural persistence, with disease seen on imaging (regardless of Tg and anti-Tg levels); or indeterminate, wherein anti-Tg was elevated or data were missing (24 –26).
Genotyping
From 2012, tumors were snap frozen in liquid nitrogen within 30 minutes of excision. Samples were maintained at −80°C until future use. Nucleic acids were isolated after homogenization using QIAGEN All-Prep Universal (QIAGEN, Hilden, Germany). Quantitative-polymerase chain reaction (PCR) genotyping for single-nucleotide variants in BRAF, HRAS, and NRAS and for chimeric transcripts RET/PTC1 and RET/PTC3 and PAX8/PPARg was performed according to the manufacturer's directions using Thyroid Cancer Mutation Panel and Thyroid Cancer Fusion Gene Detection Kit (Entrogen, Woodland Hills, CA) and analyzed on a BioRad CF96 Touch real-time PCR detection system. Immunohistochemistry for the BRAFV600E variant was performed using the BRAF VE1 antibody (Ventana Medical Systems, Tucson, AZ) and showed complete concordance with molecular genotyping (positive in 1 of 1 sample and negative in the remainder). Samples for which no pathogenic variant was identified by genotyping were analyzed by whole-transcriptome (RNASeq) analysis, as described previously (27). Archival formalin-fixed paraffin-embedded specimens from surgery before 2012 were not analyzed due to technical limitations related to degraded RNA quality.
Statistics
Descriptive statistics and measures of diagnostic accuracy—sensitivity, specificity, positive and negative predictive values, and receiver operator characteristic (ROC) curve analysis—were used to characterize the cohort and establish the utility of the collected data variables in predicting lung metastasis. Fisher's exact test was used for comparing categorical variables. t-Test assuming unequal variances and Mann–Whitney U test were used for comparing parametric and nonparametric continuous data, respectively. Statistical significance was defined as p < 0.05.
Results
Cohort characteristics
We reviewed 98 consecutive patients and excluded 5 due to incomplete data. The median age at diagnosis was 13.8 years (range 5.3–17.6 years) and 58 of 93 (62%) patients were female. Lung metastases were identified in 19 of 93 (20%) patients. Table 1 compares the characteristics of those with and without lung metastasis. Those with lung metastases were younger (p < 0.001), and had more advanced T and N staging (p = 0.002 and p < 0.001, respectively). There was no statistical difference in the histological variant of DTC, but there was a trend toward an increased rate of lung metastasis among those with the diffuse sclerosing variant of papillary thyroid cancer (DSV-PTC) (Table 1).
Characteristics of Patients With and Without Lung Metastasis
Percentages are of column.
Fisher's exact test for categorical and Mann-Whitney U test for continuous variables.
Denominator 18; missing data n = 1.
FTC, follicular thyroid carcinoma; M0, no lung metastasis; M1, lung metastasis; PTC, papillary thyroid cancer.
Predictors of lung metastasis
Younger age at diagnosis was associated with lung metastasis; 16 of 40 (40%) patients <13 years old had lung metastases, whereas 3 of 53 (6%) patients 13–18 years old had lung metastases (Table 1). Larger primary tumor diameter was associated with lung metastases (p = 0.01; Table 1) and ROC curve analysis (Fig. 1) showed an area under the curve of 0.68 (95% confidence interval [CI 0.55–0.81], p = 0.02). When maximizing overall accuracy, a tumor diameter ≥3.25 cm had a sensitivity of 66.7% and specificity of 71.2% for patients with lung metastases.

Receiver operating characteristic curve analysis of tumor diameter and lung metastases. Area under the curve 0.68 [CI 0.55–0.81], p = 0.02. CI, 95% confidence interval.
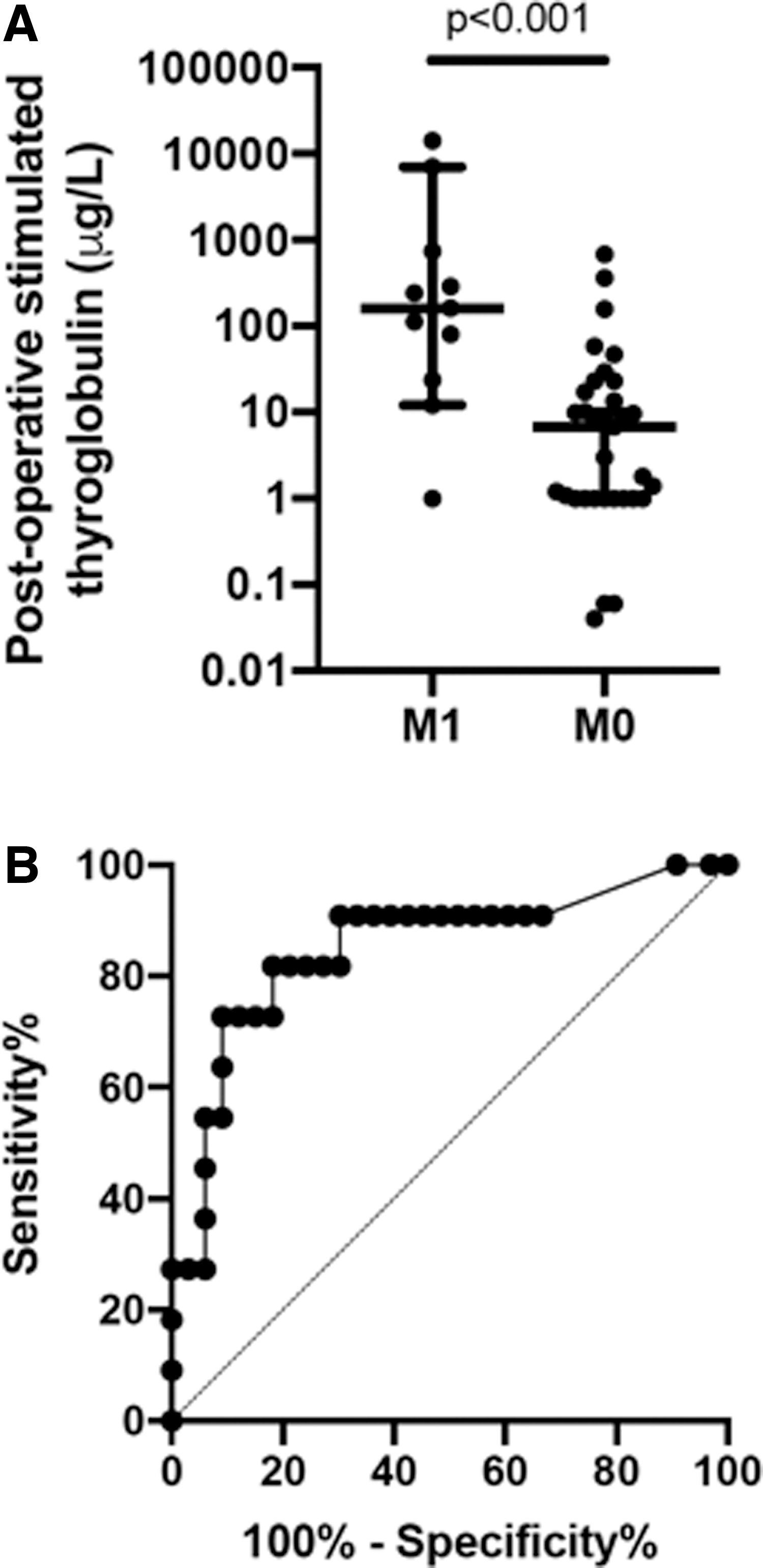
Table 2 illustrates the association between other variables and lung metastasis. T-stage below T3, absent clinical LN disease, and absent pathological LNs had negative predictive values ≥90%. An elevated postoperative sTg (≥2 ng/mL) was seen in 10 of 11 (91%) of those with lung metastases (p = 0.036). One patient's postoperative sTg was 1 ng/mL (with undetectable Tg antibodies); however, a previously abnormal computed tomography (CT) suggested lung metastases and prompted 131I therapy, and the patient's follow-up sTg after 1 year was 5.7 ng/mL. Postoperative sTg levels were significantly higher in those with lung metastases (p < 0.001; Fig. 2A) and it was shown to be an accurate predictor of lung metastasis by ROC curve analysis (Fig. 2B). Preoperative basal Tg >60 ng/mL was 100% sensitive for lung metastasis ([CI 57–100]; p = 0.007), but few data were available (n = 15; Table 2) as this is not a standard component of preoperative evaluation of children and adolescents with thyroid nodules at our institution.
(
Clinical, Biochemical and Pathological Variables Associated with Lung Metastasis
Fisher's exact test.
Excluded data when anti-Tg raised or missing
cN1, clinical lymphadenopathy by examination or ultrasound; LN, lymph node; M1, distal (lung) metastasis; NPV, negative predictive value; pN1, lymph node disease confirmed on pathology; PPV, positive predictive value; Sens, sensitivity; Spec, specificity; Tg, thyroglobulin (ng/mL).
Molecular alterations were assessed in 9 of 19 specimens. Of these, 9 of 9 specimens were positive for a genomic alteration associated with PTC (1 BRAFV600E , 1 NRASQ61R , 1 oncogenic NTRK3 fusion, and 6 oncogenic RET fusions), as summarized in Table 3.
Patient Characteristics with Lung Metastasis: Initial Imaging
Diagnosis defined as time of thyroidectomy
Time in months from diagnosis by nuclear imaging or CT
Findings on nuclear imaging
Single focal lesion
Primarily CV with features of follicular, solid and sclerosing variants.
—, molecular testing not performed; CV, classical variant; DSV, diffuse sclerosing variant; FV, follicular variant; iFV, invasive follicular variant; NS, not specified; PD, poorly differentiated.
Detection of lung metastases
Most lung metastases were identified within the course of initial staging. Lung metastases were first diagnosed >6 months postoperatively in 2 of 19 (11%) patients (patients 2 and 16). Patient 2 had a normal diagnostic 131I WBS after 1 and 2 years, developed new cervical disease after 5 years, and was subsequently diagnosed by WBS that demonstrated lung metastasis after 8 years, despite a negative scan 2 years prior. Although Tg measurements were “normal,” there was a concurrent rise in anti-Tg titers. Patient 16 had a negative post-therapy 131I WBS after 1 month and subsequently normal annual diagnostic 131I WBSs over 3 years of surveillance; an elevated Tg and new findings on ultrasonography and positron emission tomography/CT suggested recurrent cervical disease. Despite the normal WBS, a preoperative cervical CT four years after initial treatment identified apical lung lesions and a subsequent chest CT showed diffuse distribution of disease.
Lung metastases were diagnosed by pre-operative CT in 2 patients (patient 3, in whom pre-ablation 123I WBS was negative, but post-therapy WBS was positive with diffuse uptake; and patient 13 in whom pre-ablation 123I WBS was positive with diffuse uptake); by pre-ablation 123I in 1 patient (patient 7, with diffuse uptake); by post-therapy WBS in 13 patients; and by diagnostic (surveillance) 131I WBS in 1 patient (patient 2, described above). Data were missing for two patients. In total, 11 patients underwent CT and 12 patients had pre-ablation 123I results available.
The patterns of lung metastases (Table 3) were diffuse in 11 of 19 patients (Fig. 3A, B), multifocal in 4 of 19 patients (Fig. 3C, D), diffuse with a solitary focal lesion in 1 patient (Fig. 3E, F), and there were missing data for 3 patients.

Representative images of lung metastasis uptake patterns on 131I whole body scan: diffuse [anterior (
Lung metastasis treatment and outcome
The median initial RAI activity administered to children and adolescents with lung metastases was 100 mCi (range 58–200), the median cumulative RAI activity was 246 mCi (range 100–650), and the median total number of RAI courses was 2 (range 1–4; Table 4).
Patient Characteristics with Lung Metastasis: Treatment and Outcome
mCi.
Based on latest WBS or CT.
Either baseline Tg >1 ng/mL or stimulated Tg >2 ng/mL, and normal anti-Tg.
Persistence on CT and NED on WBS.
CT+, CT positive for lung metastasis and WBS data not available; NED, no evidence of disease; RAI, radioactive iodine; WBS, whole body scan; WBS+, whole body scan positive for lung metastasis and CT data not available.
Approximately 1 year after treatment—median 11.5 months (range 5–33 months)—8 of 19 (42%) patients had a normal diagnostic WBS, and in 6 of 19 (31%) patients, there was persistent lung uptake; data were missing for 5 patients. Response to therapy at the most recent visit was “excellent” in 3 of 19 (16%) patients, “biochemically persistent” in 1 of 19 (5%) patients, “structurally persistent” in 13 of 19 (68%) patients—of which 1 patient died as a consequence of lung metastasis—and indeterminate in 2 of 19 (11%) patients. The median follow-up duration was 5 years (range 1–8 years; Table 4). Of those with “structurally persistent” disease, 12 of 13 patients also had biochemical persistence; 1 patient had missing data.
The initial lung metastasis pattern (focal or diffuse), number of RAI courses, and cumulative RAI activity were not associated with structural outcome. Lung metastasis pattern was not associated with structural outcome one year after RAI therapy. Elevated postoperative sTg (≥2 ng/mL) was associated with both biochemical persistence (with or without structural persistence, p = 0.02) and structural persistence (p = 0.017).
Imaging modality discordance
At the time of diagnosis with lung metastasis, 11 of 19 individuals had concurrent WBS and CT imaging; in 9 of 11 cases, the WBS and CT findings were concordant; in patient 1 the post-therapy WBS scan was positive and CT negative for lung metastases; and in patient 3, preoperative CT was suggestive of lung metastases, although the preablation 123I WBS 5 months later did not demonstrate appreciable iodine uptake (despite a raised sTg). Subsequent post-therapy WBS demonstrated diffuse lung uptake.
Three patients (6, 7,and 10) showed discordance between a normal diagnostic WBS and positive CT imaging on initial follow-up 1 year after RAI treatment. Two patients (patients 3 and 5) showed discordance between a normal diagnostic WBS and positive post-therapy WBS after RAI treatment for metastases based on CT findings.
Eight patients had no detectable disease on diagnostic WBS approximately one year after RAI therapy (Table 4). Although 5 of 8 patients had structurally persistent/recurrent disease at their latest assessment, they also had a persistent biochemical outcome.
Three of 19 patients met criteria for progressive RAI refractory/resistant disease and have initiated systemic therapy with either partial response or stable disease. Ten patients in this series received initial treatment at our institution; however, they were transitioned to adult care before targeted therapy becoming available.
Discussion
We present a relatively large pediatric cohort of children and adolescents with DTC and lung metastasis; 20% of patients with DTC had lung metastases and the majority were diagnosed within 6 months of DTC diagnosis. We found that younger age, larger primary tumor, presence of regional LN metastases, and elevated preoperative basal Tg and postoperative sTg were associated with lung metastasis. There was an excess of males and DSV-PTC in those with lung metastases. There was incomplete concordance between imaging modalities (123I, 131I, and chest CT) for identifying lung lesions.
These data show a low likelihood of complete remission among children and adolescents with lung metastases from DTC. Our findings can help clinicians identify patients in whom to suspect lung metastasis, to appreciate the limitations of imaging modalities, and guide patient expectations regarding outcomes of RAI therapy.
Prevalence and timing of lung metastasis
The prevalence of lung metastasis in our pediatric cohort (20%) is comparable with 2 recent series of CAYA with DTC, which reported 21% and 18% prevalence (4,7). Most lung metastases (17 of 19; 89%) were diagnosed in the context of initial disease staging and 2 of 19 (11%) patients were diagnosed beyond 6 months postoperatively; 1 patient had initially normal scans, which suggests either inadequate imaging sensitivity or true late onset of distant metastasis. Wang et al. (13) showed that 62 of 80 (78%) adults with DTC were diagnosed with lung metastases before 131I therapy in a setting wherein all patients underwent chest CT before RAI. Qutbi et al. (18) showed that 61 of 75 (81%) adult patients were diagnosed “at presentation” of DTC. In a recent systematic review of patients <21 years, 14 of 112 (13%) were diagnosed with lung metastases at follow-up rather than at diagnosis of DTC; the authors propose that lung metastases missed at disease presentation may have been due to the variability in postoperative staging and use of initial RAI therapy (17). Therefore, CAYA with lung metastases are likely to be identified with appropriate initial staging. The rare occurrence of late metastatic disease necessitates ongoing surveillance in CAYA with DTC.
Associations with lung metastasis and outcome
Lung metastasis was more prevalent in younger patients and we found, even among children, lung metastasis was far more prevalent in those <13 years old (40% of children <13 years had lung metastases compared with 6% of adolescents aged 13–18 years). This is also reported in several other pediatric cohorts (28,29), but is not a universal finding (7). These data suggest that lung metastasis is a predominately prepubertal complication of DTC.
Sex was not significantly associated with lung metastasis, which is consistent with another pediatric cohort (7); however, we found a lower female-to-male ratio of patients with lung metastasis. Although DTC is more prevalent in females, the female-to-male ratio is lower in children than in adolescents (30,31). Therefore, the lower female-to-male ratio of patients with lung metastasis may simply be a reflection of the young age in our cohort and the sex distribution of DTC in this age range.
Tumor size was associated with lung metastasis, which is in line with another pediatric study (29), but in contrast to adult data showing lung metastasis to be independent of tumor size (32). The clinical utility of using tumor size in predicting lung metastasis is limited as a smaller tumor size improves sensitivity but reduces specificity. No patient with T1a disease had lung metastases and all patients with T4 disease had lung metastases. This association is inconsistent across other studies (7,28,29), although Livhits et al. (7) reported that 8 of 8 CAYA with lung metastases had greater than T1 disease and Collini et al. (33) reported that 5 of 5 patients had either T2 or T4 disease. Therefore, T-stage could offer clinical utility as a risk factor for lung metastasis and the approach to staging in CAYA with T1 may merit reconsideration.
LN disease has been reported to be strongly associated with lung metastasis (6,7,12,14,32,34,35); similarly, we found a higher N-stage was associated with lung metastasis. In contrast, Ronga et al. (19) reported that 15 of 42 (36%) patients with lung metastasis, <45 years old, had no LN involvement; however, in that series, not all patients underwent neck dissection, therefore, nodal metastasis may have been underestimated. We found that the absence of clinical and histological LN disease had a negative predictive value of 90% and 96%, respectively. One patient with lung metastasis in our series had negative pathology and imaging for LN disease; however, only four LNs were resected, and it is feasible that clinically occult disease, undetectable by imaging, was present.
Molecular alterations were found in all tumors that underwent analysis from this cohort. There was a high proportion of oncogenic fusions involving the RET proto-oncogene, as has been described previously among pediatric tumors.
A postoperative sTg ≥2 ng/mL identified patients with lung metastasis with 91% sensitivity. Current clinical practice guidelines recommend RAI therapy and post-therapy WBS when sTg exceeds 10 ng/mL, or if sTg is 2–10 ng/mL and there is known residual neck disease or thyroid bed uptake and T4 disease (3). An sTg cutoff at 23.5 ng/mL optimizes sensitivity and specificity for lung metastasis—both 82%—and an sTg cutoff at 11 ng/mL optimizes sensitivity to 90.9% (and specificity 69.7%). Livhits et al. (7) found that a post-thyroidectomy (and preablative) sTg of 154 ng/mL was 87.5% sensitive and 91.7% specific for lung metastasis, but when this cutoff is applied to our cohort, the sensitivity is 50%. The variation in reported accuracy of postoperative sTg, to identify patients with lung metastasis, likely reflects the different sample sizes, patient ages, prevalence of metastases, and assays between studies (7,36 –38).
Preoperative basal Tg was assessed in a small subset of our cohort (n = 15), and a level >60 ng/mL without Tg antibodies (n = 7) predicted lung metastasis with 100% sensitivity. This is approximately twice the upper limit of the reference range for this age group [28.5 ng/mL for age 6 to <9 years and 25.6 ng/mL for age 9 to <19 years (39)]. Data are inconsistent as to whether preoperative basal Tg has clinical utility in distinguishing benign from malignant thyroid nodules (40 –43). There are data, however, suggesting it may have a role in predicting distant metastasis (44), which our findings support, and this should prompt further investigation into its utility in pediatrics.
Imaging discordance
We found discordance between 123I preablation and post-therapy WBS, and between WBS and CT in their identification of lung metastasis on a number of occasions. At diagnosis, 13 of 17 cases of lung metastasis were diagnosed by post-therapy WBS, while only 1 of 17 by 123I diagnostic WBS. Two pediatric cohorts reported identification rates of lung metastasis by diagnostic WBS of 19 of 28 (68%) and 17 of 27 (74%) patients (6,34) as compared with 1 of 17 (6%) patients in our cohort, which is more comparable with the study by Alzahrani et al. (4) who identified 3 of 21 (15%) patients by preablation WBS. The use of 131I instead of 123I could explain these contrasting results. Although 123I has a shorter half-life and a supposedly diminished stunning effect when compared with 131I (45), lung metastases may be missed on a 123I diagnostic WBS compared with post-therapy WBS (46 –48). The sensitivity of 123I identifying lung metastases may be further diminished by our institution's protocol that uses a relatively lower dose of 123I and, in recognition of this potential pitfall, higher doses of 123I have more recently been used for diagnostic scans (49).
Our data emphasize the importance of multi-modality imaging when an increased risk or suspicion of lung metastasis exists, particularly when other clinical or biochemical indicators do not correlate with imaging findings of an isolated modality.
Treatment and outcome
At the time of most recent follow-up (median five years), the rate of “excellent response” to RAI was low in our study. A similarly low rate (0 of 20 patients) was reported in a similar cohort that used slightly higher cumulative RAI activities—median 317.5 mCi (range 109–682 mCi) versus 246 mCi (range 100–650 mCi) (4). Another cohort of patients under 20 years experienced a “complete response” in 3 of 14 cases (6%) (10). A systematic review found a “complete response” in 47% of CAYA with lung metastases; however, the studies employed different outcome criteria (“complete response” was defined as sTg <10 ng/mL) when compared with current recommendations and those referenced previously, so a direct comparison is challenging (17,50). Despite a high rate of persistent disease, overall survival is excellent—18 of 19 (95%) individuals were alive at their most recent follow-up visit.
We did not identify an association between cumulative RAI activity or number of RAI courses and structural outcome. The prognosis from lung metastases has not previously been positively associated with cumulative RAI activity (18). In CAYA, those with no response to treatment (perhaps suggesting RAI-resistant disease) nonetheless receive higher RAI activities (17). The median cumulative activity in our cohort, 246 mCi (range 100–650 mCi), and median number of RAI courses, 2 (range 1–4), were lower than previous reports, yet we found an overall survival rate and response rate similar to comparable case series (4,17,18). These findings suggest that treating nonresponsive disease with cumulatively higher RAI activities might not improve outcome and could increase the risk of side effects from RAI therapy.
The pattern of lung metastasis (diffuse or focal) was not associated with response to RAI treatment; this was also found in a CAYA study and several adult series (13,16,18,19). We found that a raised postoperative sTg was associated with worse biochemical and structural outcome in patients with lung metastasis. A similar association has been shown in adults with DTC (51), in adults with lung metastasis from DTC (13,16), and in children and adolescents with DTC (52). These studies were predominately adult cohorts and there are few studies investigating factors associated with the treatment response of CAYA with lung metastasis.
The majority of children with lung metastases do not achieve a complete response to therapy. Multiple effective systemic therapies now exist for those with symptomatic or progressive disease. In comparison with adults, pediatric tumors are primarily driven by oncogenic fusions involving RET, NTRK1,2,3, and other receptor tyrosine kinases, and, less commonly than in adults, the BRAFV600E mutation (53 –55). A knowledge of tumor genomics is, therefore, essential to fully describe these tumors and potentially to identify adjunct therapies. Targeted therapeutics have been shown to be effective (56 –59) or are the subject of active clinical trials (60,61), although systemic treatment should only be undertaken in consultation with a high-volume center familiar with its use in childhood-onset DTC. Nonetheless, the high prevalence of RET-fusion tumors in this cohort (5 of 9 (56%)) raises the future possibility of RET-targeted therapy, either before RAI (as cytoreductive therapy) or subsequently to reduce overall tumor burden. Further clinical evidence, however, including long-term effectiveness and safety data, as well as a better understanding of where these agents fit along the therapeutic odyssey, is needed before moving forward with such approaches.
Limitations
Our patients' data were collected retrospectively for 20 years; during this time, treatment approaches evolved (3,22) and practice between clinicians varied. Not all patients started and completed their care at our institution, thus some data were incomplete. Although far more common in children and adolescents, the absolute number of patients with lung metastasis at a single institution remains small and limits the statistical power of the cohort, thus larger multi-center studies are needed to allow for more rigorous statistical modeling. Despite this, we identified several statistically significant results that may impact evidence-based clinical care.
Conclusions
In this cohort of children and adolescents, lung metastases from DTC were associated with younger age, larger tumor size, LN disease, preoperative Tg, and postoperative stimulated Tg with a trend toward an association with DSV-PTC. Preoperative Tg has a potential role in predicting those with lung metastasis as we found 100% sensitivity; however, our small numbers mean further study is required before making clinical recommendations.
A lower threshold for suspecting lung metastasis should be maintained in younger patients with LN disease and elevated postoperative stimulated Tg—in the context of these risk factors, a normal preablative WBS may be falsely reassuring and post-therapy WBS or CT is an important additional imaging modality to consider.
An excellent response to therapy is uncommon and multiple RAI courses do not necessarily improve outcome; however, overall survival is excellent. The aim for complete remission must be balanced against the potential harms of cumulative radiation exposure. These are important concepts to explain to young people and their families at diagnosis and for physicians to consider when discussing their management and treatment goals.
Footnotes
Author Disclosure Statement
J.D.W. participated on an advisory board for Bayer pharmaceuticals. For all other authors, no competing financial interests exist.
Funding Information
A.D.C. was the recipient of a Canadian Paediatric Endocrine Group fellowship, which supported, in part, the preparation of this article.