
Abstract
Background:
Anaplastic thyroid carcinoma (ATC) is nearly always fatal. Large studies on ATC are exceedingly rare. We aimed to study the clinical, genotypic, and histologic characteristics of ATC in the largest retrospective cohort of ATC to date.
Methods:
Three hundred sixty patients with ATC from two tertiary centers were studied. Molecular testing was performed in 126 cases including 107 using next-generation sequencing.
Results:
The median patients' age was 68 years. Differentiated thyroid carcinoma (DTC) was present in 208 cases (58%), the most common being papillary carcinoma (n = 150). The 1-, 2-, 3-, and 5-year overall survival (OS) was 36%, 17%, 13%, and 11%, respectively. On univariate analysis, age, resectability, chemotherapy, radiotherapy, margin status, encapsulation, gross residual disease, gross extrathyroidal extension, percentage, and size of ATC in the primary tumor predicted OS (p < 0.05). Age, resectability, chemotherapy, and gross residual disease were independent prognostic factors in the entire cohort, while gross residual disease was the only independent predictor of OS in patients who had resection of their tumor. BRAF, RAS, TERT promoter, TP53, PIK3CA, E1F1AX, and PTEN mutations were detected in 45%, 24%, 75%, 63%, 18%, 14%, and 14% of ATC, respectively. Concomitant BRAF/RAS and TERT mutations were associated with worse outcome than mutation in only one of the genes. BRAF-mutated and RAS-mutated ATCs had similar frequency of nodal and distant metastasis. Twelve cases were pure squamous cell carcinoma, 60% of which carried BRAFV600E mutation and showed a similar OS to other ATCs.
Conclusions:
(i) Gross residual disease remains the most crucial indicator of outcome in ATC. (ii) Encapsulation, margin status, percentage, and size of ATC in the primary were prognostically relevant. (iii) Pure thyroid squamous cell carcinoma may be considered as ATC given a BRAFV600E genotype and similar outcome. (iv) In contrast to DTC, BRAF-mutated and RAS-mutated ATCs have similar metastatic spread. (v) Concomitant mutations of BRAF or RAS with TERT confer a worse prognosis.
Introduction
Anaplastic thyroid carcinoma (ATC) is a rare but lethal form of thyroid cancer with an incidence of 0.9 to 1.2 cases per 1,000,000 population and a median survival of 3–4 months based on the Surveillance, Epidemiology, and End Results (SEER) data (1,2).
Significant advances have been made in recent years in understanding the molecular pathogenesis of ATC. While BRAF and RAS mutations remain the main drivers in ATC similar to differentiated thyroid carcinoma (DTC), ATCs commonly contain additional molecular events, including high frequency of TERT promoter and TP53 mutations, as well as frequent alterations in gene encoding effectors in the PIK3CA-PTEN-AKT-mTOR pathway, SWI-SNF complex, histone methyltransferases, and mismatch repair (MMR) (3 –6). The identification of these targetable molecular alterations in ATC led to incorporation of targeted therapies into the traditional multimodality treatment of ATC (7,8). For example, combination of dabrafenib (BRAF inhibitor) and trametinib (MEK inhibitor) treatment demonstrates robust responses in BRAFV600E -mutated ATCs (9).
Little is known about the prognostic factors in this cohort of patients. Population/registration-based studies (1,2,10,11) have reported distant metastasis, lymph node metastasis, age, surgical resectability, surgical margin status, tumor size, radiation therapy, and/or chemotherapy as independent prognostic factors in ATC. However, a contemporary large-scale clinicopathologic and molecular study with meticulous histopathologic review to identify possible prognostic factors is lacking.
Aiming to understand the clinical–pathologic–molecular correlation and the prognostic factors of ATC, we herein present the largest comprehensive retrospective cohort of 360 ATC patients from 2 tertiary centers, including 178 primary thyroidal ATCs, which underwent surgical resection, and 126 analyzed at the molecular level.
Methods
Characteristics of the study cohort and clinicopathologic review
The study was approved by the Institutional Review Board of Memorial Sloan Kettering Cancer Center (MSKCC, New York, NY) and Royal North Shore Hospital (RNSH, Sydney, Australia). Pathology database at MSKCC was searched for “anaplastic carcinoma” or “dedifferentiated carcinoma.” All ATC cases with slides available for review diagnosed between 1985 and 2019 were included in this study. The slides of all patients were reviewed by at least one of four endocrine pathologists (B.X., A.J.G., T.F., and R.G.) to confirm the ATC diagnosis and to gather detailed pathologic features. A total of 360 patients with ATC were included in this retrospective study (MSKCC n = 289, RNSH n = 71).
The following clinical and pathologic characteristics were collected for each case: sex, age at first ATC diagnosis, site of ATC (thyroid primary, nodal metastasis, distant metastasis, and/or locoregional recurrence), type of procedure (cytology/core biopsy, incisional/excisional biopsy, and resection), the presence and type of prior or concurrent DTC, the predominant cytologic features of ATC, mitotic index (per 10 high-power fields within the most mitotically active area, field diameter 0.55 mm), atypical mitoses, true tumor necrosis (rather than infract-type necrosis secondary to prior procedure), immunophenotype (PAX8 polyclonal, TTF-1, thyroglobulin, cytokeratin AE1/AE3, and CAM5.2), and treatment (attempted surgical resection, chemotherapy, radiation therapy, targeted therapy, and immunotherapy).
Tumor necrosis was composed of degenerating cytoplasm and punctate karyorrhectic nuclear debris. The presence of fibroblastic stromal reaction, hemorrhage, or an identifiable needle track in the necrotic area was attributable to reaction induced by prior fine-needle aspiration and was therefore not regarded as tumor necrosis.
The cytologic features of ATC were defined as follows: (i) spindle cells with prominent nuclear spindling; (ii) pleomorphic with significant variation in nuclear size; (iii) epithelioid ATC with cohesive nests/sheets of epithelioid cells exhibiting round nuclei and no definite line of differentiation; (iv) squamous cell carcinoma with keratinization and/or intercellular bridges; (v) rhabdoid in which tumor cells contain prominent round cytoplasmic inclusion and eccentrically located nuclei; (vi) osteoclast giant cell-rich; and (vii) tumor giant cells defined as ATC tumor cells with multinucleation (Fig. 1).

Histologic features of ATC. ATC may show spindle (
The antibodies utilized for immunohistochemistry included PAX8 (polyclonal, dilution 1:100; Proteintech), TTF-1 (8G7G3/1, monoclonal, ready-to-use [RTU]; Ventana), thyroglobulin (2H11 + 6E1, RTU; Cell Marque), cytokeratin AE1/AE3 (1:1600; Dako), CAM5.2 (1:75; Becton & Dickinson), CK 5/6 (D5/16B4, RTU; Ventana), and BRAFV600E (VE1, 1:400; Abcam).
Additionally, for the resected primary thyroidal ATC with or without gross residual disease, the following pathologic features were collected: the size of the entire carcinoma, the size and percentage of the ATC component, infiltration versus encapsulation, capsular invasion, vascular invasion, the presence and extent of microscopic extrathyroidal extension (ETE), gross ETE observed intraoperatively or radiologically, margin status, gross residual disease documented in the operative reports by the surgeons, nodal status, size and histotype of nodal metastasis, size and percentage of ATC within the lymph node, and extranodal extension.
Three hundred twenty-seven patients had clinical follow-up data available. The primary outcome was overall survival (OS). Disease-specific survival (DSS) was also calculated.
Molecular analysis
Molecular analysis using various platforms was conducted in a subset of 126 cases on formalin-fixed paraffin-embedded tissue blocks, including Sanger sequencing for BRAF mutation and/or NRAS mutations (BRAF: n = 9, NRAS: n = 5) (12), Sequenom (n = 10) (12,13), and next-generation sequencing (NGS, n = 107). Among the 107 cases that were subjected to NGS, 101 were tested using MSK-IMPACT™ (Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets) platform (14,15), 3 using FoundationOne™ (16), and 3 using a customized panel covering mutation hot spots in 14 genes (AKT1, BRAF, CTNNB1, GNAS, HRAS, KRAS, NRAS, PIK3CA, PTEN, RET, TP53, TSHR, TERT, and EIF1AX) and 76 fusions (including the most common fusions in thyroid carcinoma, RET, NTRK, PAX8-PPARG, and ALK; full list provided in Supplementary Table S1).
Twenty-nine cases that were subjected to MSK-IMPACT platform were previously reported (3,4). Among the 101 cases tested using MSK-IMPACT platform, 35 (35%) were biopsies or cytology cell blocks, 9 (9%) were incision or excision, and 57 (56%) were resection specimens.
The details of all molecular platforms were previously described. In brief, MSK-IMPACT is a Food and Drug Administration (FDA)-approved deep-coverage, targeted NGS assay detecting single nucleotide variants (SNVs), small insertions/deletion (indels), copy number variants, and fusion/structural variants in 468 oncogenes, using custom DNA probes designed for targeted sequencing of all exons and selected introns, including canonical and selected noncanonical transcripts (14,15). FoundationOne is a commercially available FDA-approved NGS platform detecting SNV, indels, copy number alterations, and rearrangement in 324 genes (16).
Sequenom is a MassARRAY system based on matrix-assisted laser desorption/ionization time-to-flight mass spectrometry that was used to interrogate the presence of single nucleotide variation in 91 hot spots of 8 oncogenes: BRAF, NRAS, KRAS, EGFR, PIK3CA, AKT1, MEK1, and ERBB2 (13). Only the 101 cases with MSK-IMPACT were subsequently plotted using cBioPortal Oncoprint (17). For the remaining 25 cases, alterations in BRAF, RAS, TERT promoter, and TP53 mutations were documented when available and were incorporated into our statistical analysis.
Statistical analyses
All statistical analyses were performed using the SPSS software 24.0 (IBM Corporation, New York, NY). The prognostic significance of each parameter on OS was calculated using log-rank test or univariate Cox proportional hazard model. All clinical and pathologic parameters collected were subjected to univariate survival analysis. Factors significant on univariate analysis were subsequently subjected to multivariate analysis using Cox proportional hazards model. Additionally, the clinicopathologic features of ATC subgroups, BRAF-mutated versus RAS-mutated ATC, and ATC with pure squamous cell carcinoma phenotype versus other ATCs were compared using chi-square test or Fisher's exact test. p-Values less than 0.05 were considered to be statistically significant.
Results
Clinical features of the study cohort
The clinicopathologic characteristics of the study cohort are summarized in Table 1. The median age of patients during ATC diagnosis was 68 years (range 29–99 years). Only seven patients (2%) were diagnosed with ATC when they were younger 40 years. There was a slight female predominance with a female:male ratio of 1.2:1. The diagnosis of ATC was most frequently rendered on surgical resection specimen (n = 227, 63%), including 178 resections of the primary ATC in the thyroid gland proper. A pathologic diagnosis of ATC was pathologically confirmed in the thyroid gland (n = 271, 75%), lymph node metastasis (n = 94, 26%), distant metastasis (n = 41, 11%), and/or locoregional recurrence (n = 27, 8%).
Clinical and Pathologic Characteristics of Anaplastic Thyroid Carcinoma in the Entire Cohort (n = 360) and in Primarily Resected Specimens (n = 178)
Data are expressed as n (%) for categorical variables and median (range) for continuous variables.
Predominant cytologic feature is defined as the cytologic feature that accounts for the largest percentage within an ATC.
ATC, anaplastic thyroid carcinoma; DM, distant metastasis; DTC, differentiated thyroid carcinoma; ETE, extrathyroidal extension; HPFs, high power fields; LN, lymph node; LRR, locoregional recurrence.
A history of DTC and/or concurrent DTC was noted in 208 patients (58%), including papillary thyroid carcinoma (n = 150), poorly DTC defined using MSKCC criteria (n = 68) (18), Hürthle cell carcinoma (n = 21), and follicular thyroid carcinoma (n = 10). In 41 cases, the DTC contained multiple histotypes, a poorly differentiated and a well-differentiated component (being papillary carcinoma, follicular carcinoma, or Hürthle cell carcinoma). Among papillary thyroid carcinoma, tall cell variant was the most common subtype (n = 68), followed by classic variant (n = 37) and follicular variant (n = 24). Other variants of papillary thyroid carcinoma documented in our cohort included solid (n = 2), hobnail (n = 1), and diffuse sclerosing variant (n = 1). In 17 cases, the variants of papillary carcinoma were not available.
Histologic and immunophenotypic characteristics of ATC
Histologically, ATC demonstrated various cytomorphologic features, including pleomorphic (n = 184), spindle cell (n = 167), epithelioid (n = 127), squamous cell carcinoma (n = 109), rhabdoid (n = 71), osteoclast giant cell-rich (n = 45), and tumor giant cells (n = 17). It was not uncommon for an ATC to exhibit multiple cytomorphologic features (Supplementary Table S2).
The predominant feature of each tumor defined as the cytologic features comprising the highest percentage of tumor volume within the ATC component was available in 354 cases, and it was: spindle cell (n = 92, 26%), pleomorphic (n = 80, 23%), squamous cell carcinoma (n = 76, 21%), epithelioid (n = 66, 19%), rhabdoid (n = 28, 8%), and osteoclast giant cell-rich (n = 12, 3%, Fig. 1).
Other uncommon histologic features that may be noted focally within the ATC included heterologous differentiation (n = 5, including 3 osteosarcomatous and 2 chondrosarcomatous differentiation); myxoid stroma (n = 4), focal glandular differentiation (n = 3), and focal clear cell changes (n = 2). Two cases in our cohort met the description of paucicellular variant of ATC (19).
The mitotic activity noted within the ATC component varied with a median mitotic index of 8 per 10 high-power fields (range 0–78). Notably, 91 (31%) cases of ATC had a mitotic index of 5 or less per 10 high-power fields, including 5 cases with no mitotic activity. In the absence of prominent mitotic activity, especially in small (biopsy) material, other histologic features, such as marked nuclear pleomorphism and loss of thyroid differentiation demonstrated by histology and immunohistochemistry, were required to render the ATC diagnosis. Atypical mitoses, tumor necrosis, and prominent neutrophil infiltrate within the tumors were common features of ATC, being observed in 85%, 77%, and 71% of tumors, respectively.
Our cohort contained 178 resected primary thyroid ATC, and their features are summarized in Table 1. The median size of the entire primary carcinoma and the ATC component was 5.0 cm (range 2.1–15.0 cm) and 3.0 cm (range 0.4–14.0 cm), respectively. Although the majority (92%) of the cohort was composed of infiltrative tumors, 14 ATCs (8%) were entirely encapsulated. The frequency of various parameters was: vascular invasion 79%, microscopic ETE 87%, gross ETE 92%, microscopic positive resection margin 78%, gross residual disease documented intraoperatively 34%, and nodal metastasis 47%.
The immunohistochemical profile of ATC is shown in Table 2. ATCs were frequently positive for PAX8 polyclonal (126/179, 70%) and cytokeratins, cytokeratin AE1/AE3 (130/195, 67%), CAM5.2 (90/133, 68%), 34βE12 (35/75, 68%), CK18 (34/52, 65%), and CK5/6 (18/33, 55%), occasionally positive for TTF-1 (78/256, 30%), whereas nearly always negative for thyroglobulin (238/248, 96%). Abnormal p53 immunoexpression was observed in seven of nine cases tested (78%), being overexpressed in five and absence of any nuclear staining (null type) in two.
Immunohistochemical Profile of Anaplastic Thyroid Carcinoma
For p53 immunostain, the absence of abnormal expression is considered as negative, whereas abnormal expression defined as overexpression (n = 5) or absence of any nuclear stain (n = 2) is regarded as positive.
+, immunopositivity in rare cells; ++, focal and/or weak immunopositivity, +++, multifocal or diffuse immunopositivity.
Molecular profile of ATC
Among the 126 cases tested, the frequency of BRAF, RAS, TP53, and TERT promoter mutations was 45% (57/126, BRAFV600E 56 cases and BRAF deletion 1 case), 24% (29/122, including NRAS n = 21, KRAS n = 3, and HRAS n = 5), 63% (66/105), and 75% (78/104), respectively. The most common RAS mutations were NRAS Q61R (n = 13), NRAS Q61K (n = 7), and HRAS G13R (n = 3). Other alterations in the MAPK pathway included CCDC6-RET fusion in two cases, NTRK1-IRF2BP2 fusion in one case, NTRK2-CRNDE fusion in one case, and NTRK3 R630W mutation in one case. The significance of NTRK3 R630W in ATC is unclear at present.
BRAF-mutated ATC was associated with a high frequency of pure squamous cell carcinoma histotype and a high rate of associated DTC, in particular papillary thyroid carcinoma (Fisher's exact test, p = 0.002 and 0.001, respectively, Table 3). Other pathologic features, such as predominant cytomorphologic features of ATC, vascular invasion, and risk of nodal and distant metastasis, did not differ between BRAF-mutated and RAS-mutated ATCs (Fisher's exact test, p > 0.05). Additionally, BRAF-mutated and RAS-mutated ATCs had similar OS (log rank test, p = 0.945).
Genotype–Phenotype Correlation in Anaplastic Thyroid Carcinoma
Bold values indicate significant p-values.
p-Values were obtained using Fisher's exact test comparing BRAF-mutated and RAS-mutated tumors.
PDTC, poorly differentiated thyroid carcinoma.
The Oncoprint of the molecular profile of 101 ATCs tested using MSK-IMPACT platform is shown in Figure 2A. The median mutation count per tumor was 5 (range 0–34). Common alterations detected included CDKN2A/2B alteration in 25%, E1F1AX in 14%, PTEN in 14%, NF2 in 12%, NF1 in 12%, KMT2D in 9%, RB1 in 9%, ARID2 in 9%, MMR genes (MLH1, PMS2, MSH2, and MSH6) in 8%, ATM in 7%, KMT2A in 6%, MTOR in 5%, PBRM1 in 5%, and IL7R in 5%.
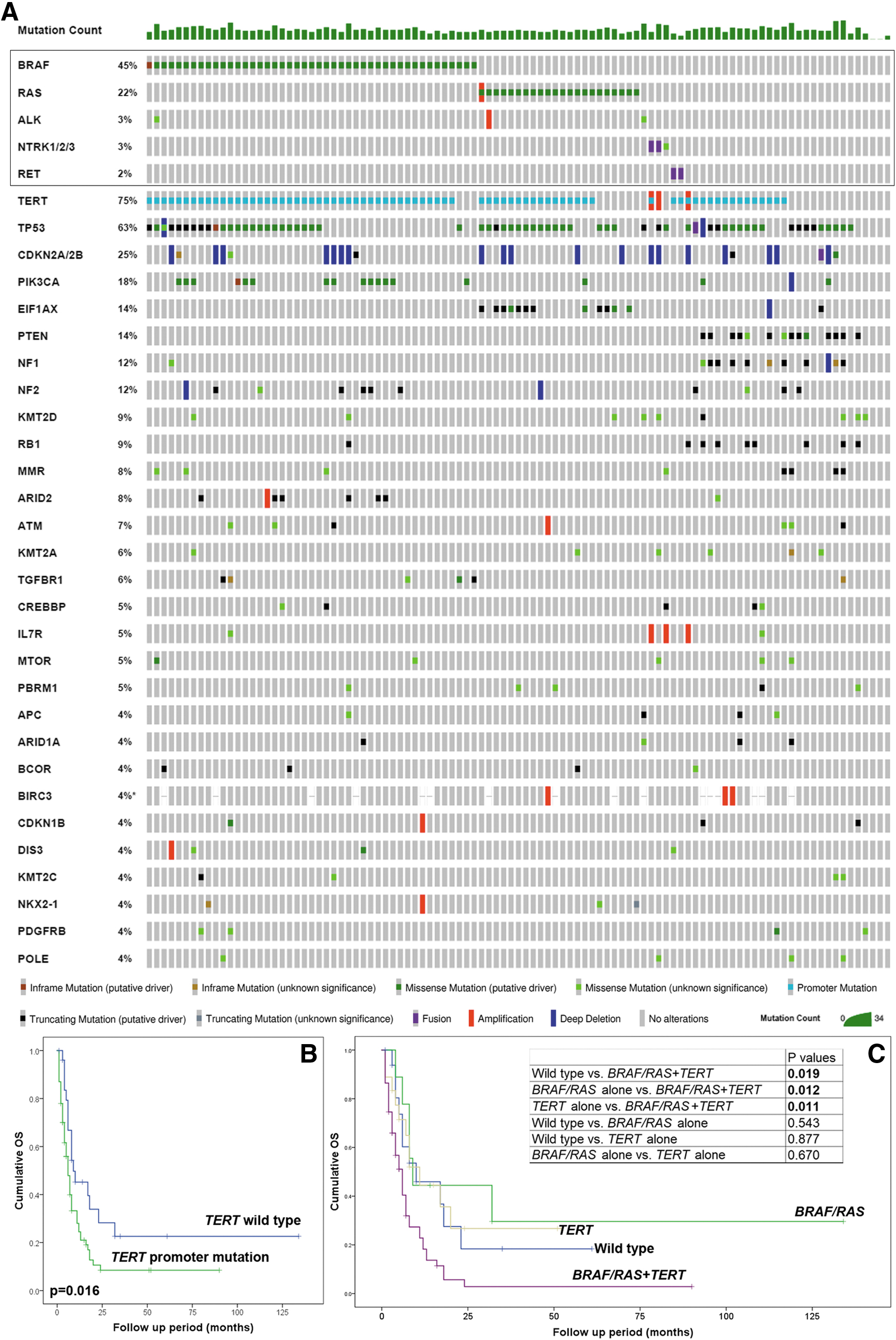
Molecular profile of ATC. (
The presence of TERT promoter mutations in ATC was associated with shorter OS (log-rank test, p = 0.016, 1-year OS was 36% and 46% in ATC with and without TERT promoter mutation, respectively, Fig. 2B). Furthermore, ATC with both BRAF/RAS mutation and TERT promoter mutation (BRAF and TERT or RAS and TERT) was associated with worse clinical outcome compared with ATC without any of these three mutations or with BRAF, RAS mutation, or TERT promoter mutation alone (log-rank pairwise comparison, p < 0.05, 1-year OS was 25%, 45%, 44%, and 47% in BRAF/RAS and TERT double mutant, TERT, BRAF/RAS, and wild-type group, respectively, Fig. 2C). Mutation count and other molecular alterations, TP53, E1F1AX, PTEN, and PIK3CA mutations, did not impact OS (log-rank test, p > 0.05).
Mutations in MMR genes were detected in eight cases: including four with MSH6, two with MSH2, one with MLH1, and one with MSH6 and MSH2 mutations. Among them, four tumors also contained alteration in genes involved in the MAPK pathway, including three BRAFV600E and one NTRK3 R630W mutation. The OS did not differ significantly from those without MMR gene defects (log-rank test, p = 0.182, 1-year OS was 47%).
BRAFV600E immunohistochemistry was a sensitive and specific screening tool for BRAFV600E mutations in ATC
In our cohort, 32 cases were tested for both BRAFV600E immunostain and BRAF mutation molecular testing. Among them, 19 ATCs were positive for BRAFV600E mutation, 1 showed BRAF deletion, whereas the remaining 12 did not have BRAF alteration. BRAFV600E immunostain was positive in 18 of 19 BRAFV600E -mutated ATC, whereas negative in all 13 ATCs without BRAFV600E mutations. The case with BRAF deletion was negative for BRAFV600E by immunostain. The sensitivity and specificity of BRAFV600E immunohistochemistry in detecting the underlying BRAFV600E mutation in ATC were 95% and 100%, respectively.
Clinical outcome and prognostic factors of ATC
Follow-up data were available in 327 patients, including 163 patients who underwent resection of their primary thyroid ATC. The 1-, 2-, 3-, and 5-year OS and DSS were 36%, 17%, 13%, and 11%; and 36%, 17%, 14%, and 14%, respectively. The median OS was nine months in the entire cohort. Sixty-one percent (189/310) of our cohort had distant metastasis, including 83 patients with distant metastasis at first ATC diagnosis.
On univariate analysis, younger age at ATC diagnosis, the presence of DTC, resection of ATC, chemotherapy, and radiation therapy were associated with longer OS in the entire cohort (Cox proportional model, p < 0.05, Table 4 and Fig. 3). Other features, such as site of ATC, cytomorphologic features, tumor necrosis, atypical mitoses, mitotic index and distant metastasis, were not associated with outcome (Supplementary Table S3). Multivariate analysis using Cox proportional model showed that age at ATC diagnosis, resection, and chemotherapy were independent prognostic factors in ATC (hazard ratio 1.671 [CI 1.276–2.188]; 0.510 [CI 0.389–0.670]; and 0.697 [CI 0.493–0.985], respectively).
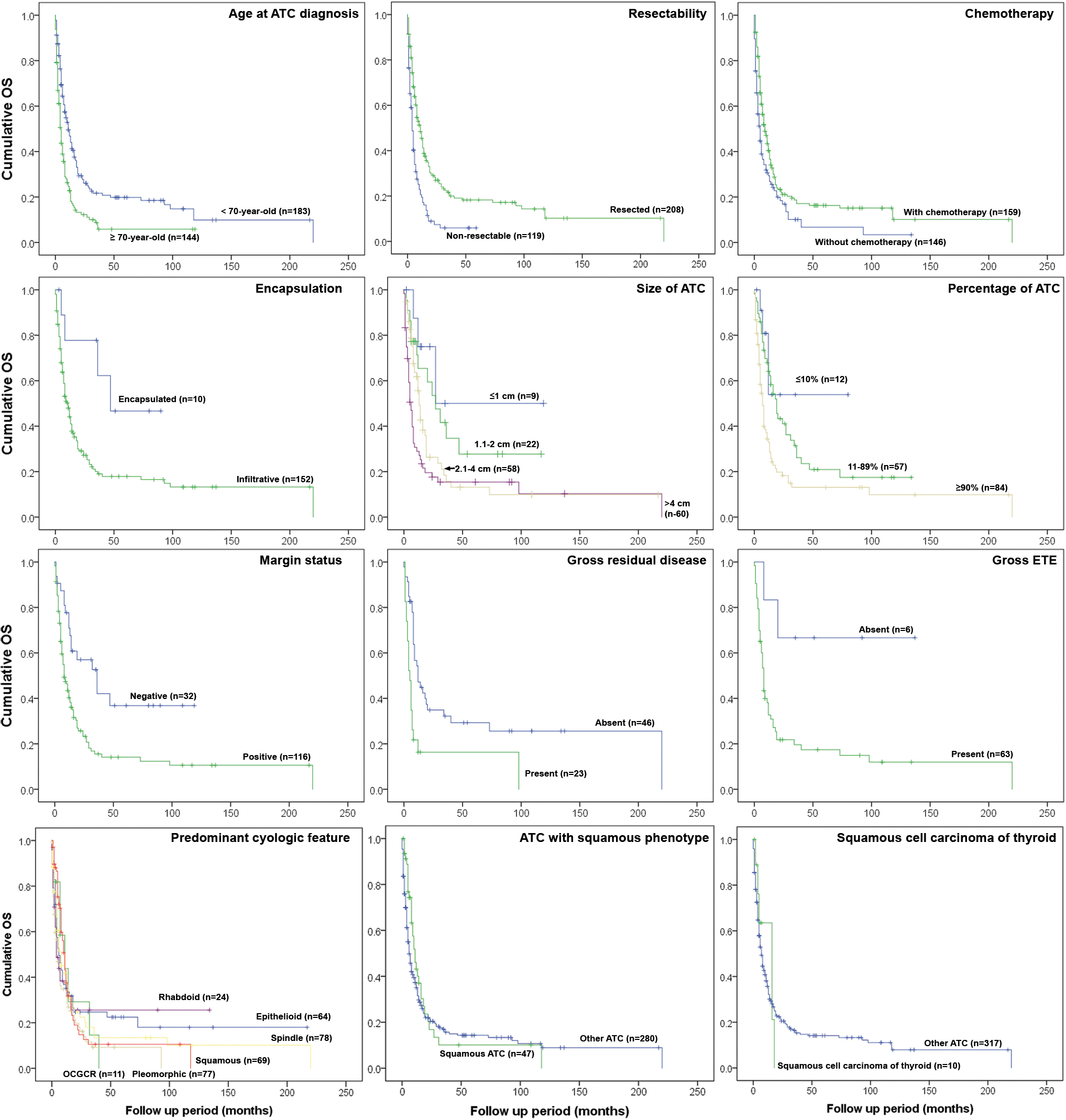
Kaplan–Meier plots of overall survival. OCGCR, osteoclast giant cell rich.
Clinical and Pathologic Prognostic Parameters in Anaplastic Thyroid Carcinoma
Bold values indicate significant p-values.
CI, 95% confidence interval; HR, hazard ratio.
Among the 163 patients who underwent thyroid resection with follow-up data, factors that were associated with OS on univariate analysis included encapsulation, percentage and size of the ATC component within the primary tumor, microscopic margin status, gross residual disease, and gross ETE (Table 4). Other parameters, such as the presence and extent of microscopic ETE, the presence and extent of vascular invasion, nodal status, and extranodal extension, were not significantly associated with OS. On multivariate analysis, the only factor that predicted OS was gross residual disease (hazard ratio 2.391 [CI 1.141–5.010], p = 0.021).
ATC with squamous cell carcinoma phenotype
In the study cohort, 51 cases demonstrated a pure squamous cell carcinoma phenotype. Compared with other ATCs, tumors with pure squamous cell carcinoma phenotype were associated with a higher frequency of previous/concurrent DTC (76% vs. 55%, p = 0.004), previous/concurrent papillary thyroid carcinoma (95% vs. 67% p < 0.001), and BRAFV600E mutation (87.5% vs. 39%, p < 0.001, Table 5). ATC with a pure squamous phenotype carried a similar dismal outcome compared with all other ATCs (log- rank test, p = 0.190), with a median OS of 12 and 9 months, respectively.
Comparison Between Anaplastic Thyroid Carcinoma with Squamous Cell Carcinoma Phenotype and Other Anaplastic Thyroid Carcinomas
Bold values indicate significant p-values.
NA, not available; PTC, papillary thyroid carcinoma.
Immunophenotypically, ATC with squamous cell carcinoma phenotype was commonly positive for PAX8 (20/22, 91%, focal in 2 and multifocal/diffuse in 18) and BRAFV600E (7/9, 78%), occasionally positive for TTF-1 (13/34, 38%, focal in 9 and multifocal/diffuse in 4), and generally negative for thyroglobulin (negative in 31/32 cases tested, 97%; focally positive in 1 case). Not surprisingly, these tumors showed a squamous immunophenotype, demonstrated by immunopositivity for high-molecular weight cytokeratins 34βE12 (8/8, 100%) and CK5/6 (4/4, 100%), p63 (6/6, 100%), and p40 (4/5, 80%).
Additionally, there were 12 tumors with a pure squamous cell carcinoma phenotype and without any previous/concurrent DTC. In theory, these tumors could be classified as primary thyroid squamous cell carcinoma, an entity recognized by the 2017 World Health Organization (WHO) classification (20). These 12 patients had a similar outcome to all other ATC patients, with a median OS of 14 months (log-rank test, p = 0.784, Table 5). Among them, the molecular signatures of five tumors were examined using MSK-IMPACT platform. Three carried BRAFV600E mutations, and one harbored an NTRK2-CRNDE fusion.
There was no significant difference between squamous cell carcinoma with and without associated DTC in term of genotype and outcome (p > 0.05, data not shown).
Discussion
In concordance with previous reports (1,2,10,11,21), we show that ATC commonly affect elderly patients and is exceedingly rare in patients younger than 40 years. In our cohort, the median survival was 9 months and the 1-year OS was 36%. Although dismal, the survival of ATC patients in our cohort appears to be better than the 3–4 months median survival and ∼20% 1-year survival reported from the SEER database (1,2) and/or cancer registry studies (10,11,21). This improved survival may be in part due to a referral bias and/or treatment differences as all our cases were collected from tertiary referral centers that regularly treat ATC with multimodality therapies. Indeed, a retrospective cohort study from the Mayo clinic, another tertiary center, also reported a median survival of 9 months and a 1-year survival of 42% in ATC patients treated with multimodality therapy (22).
The prognostic factors in ATC, especially the pathologic ones, have not been comprehensively studied. To date, only several registry-based studies have identified lack of distant metastasis (at presentation), lack of lymph node metastasis, smaller tumor size, younger age, surgical resection, a negative margin status, radiation therapy, and chemotherapy as independent prognostic factors that are associated with improved survival (1,2,10,11,21). For example, Sugitani et al. studied 677 ATCs using a Japanese ATC Research Consortium with careful annotation of clinicopathologic parameters and reported age, primary tumor size, T4b stage, presence of acute symptoms, leukocytosis, and distant metastasis as independent prognostic factors for ATC (21).
In this study, we have performed a detailed clinicopathologic review to investigate the prognostic significance of multiple pathologic parameters. In addition of confirming the prognostic role of patient age, surgical resection, chemotherapy, radiation therapy, margin status, and gross residual disease, we have found that several pathologic parameters, such as pre-existing/co-existing DTC, encapsulation, percentage of ATC within the primary tumor, and the actual size of ATC (rather than size of entire tumor), are prognostically significant on univariate survival analysis. Therefore, in primary resection of ATC, assessing the actual amount of ATC (percentage and size) as well as the encapsulation status may provide additional prognostic information for patients' follow-up and treatment.
Interestingly, Sugitani et al. reported that incidentally detected ATC was associated with improved survival on univariate analysis. It is plausible that small ATC detected incidentally are associated with improved outcome (21). Other histopathologic features, such as cytomorphologic features, mitotic index, and tumor necrosis, which play a role in the prognosis of DTC (18,23), do not affect the outcome of ATC. As the current study and registry-based studies were retrospective in nature, it is unclear whether the survival advantage observed in patients having surgical resection, radiation therapy, and/or chemotherapy is related to a true benefit of such therapies or to confounding factors, such as selection bias.
In this study, we also provide a comprehensive histopathologic description of ATC. Similar to what have been previously described (24,25), we demonstrate that ATC may exhibit various histologic features including spindle (tumor), giant cells, pleomorphic, osteoclast giant cell-rich, epithelioid and squamous morphology, with spindle cells being the most common histotype. Heterologous sarcomatoid component, although rare, may be present in <2% of cases. Immunophenotypically, ATCs are frequently positive for various cytokeratins (75%) and PAX8 (70%), whereas close to a third of cases may show TTF-1 immunopositivity. In contrast, thyroglobulin is nearly always negative in ATC. This immunohistochemical profile is consistent with what has been previously reported (26 –28). A combination of cytokeratins, PAX8, TTF-1, thyroglobulin, and mutation-specific markers (such as BRAFV600E as described below) may serve as a useful ancillary tool to distinguish ATC from its mimickers.
Interestingly, we did not detect any association between certain histologic characteristics (e.g., mitotic index, atypical mitoses, necrosis, and cytologic features) and genotype or prognosis. Even vascular invasion, a key prognostic factor and key component of risk stratification in DTC (29), was not associated with outcome of ATC. Understanding these pathologic features may be important in rendering a correct diagnosis of ATC, but it is the ATC diagnosis by itself rather than these histologic features that drives outcome. Of note, a proportion (31%) of ATC may have a mitotic index of ≤5/10 high-power fields. Therefore, a low mitotic count does not necessarily exclude a diagnosis of ATC.
In the current WHO classification (fourth edition, 2017), primary squamous cell carcinoma of the thyroid gland (defined as a tumor purely composed of squamous cells) is considered as a separate tumor entity from ATC (20). Herein, we demonstrate that the squamous phenotype is a common histotype of ATC and may coexist with other cytohistologic features. ATC with pure squamous cell carcinoma phenotype is often associated with BRAFV600E mutations and DTC, particularly papillary thyroid carcinoma. Additionally, de novo squamous cell carcinoma of the thyroid gland, that is squamous cell carcinoma without any associated DTC, frequently harbors gene alterations in the MAPK pathway resembling thyroid follicular cell-derived carcinomas.
More importantly, we confirm that squamous cell carcinoma, with or without an associated DTC component, has a comparable dismal outcome as ATC. Similarly, an epidemiologic study based on the National Cancer Database also reported a poor prognosis of thyroid squamous cell carcinoma akin to ATC with a 5-year OS of 18% (30). Together, these findings suggest that squamous cell carcinoma of the thyroid gland may be regarded as ATC, rather than a separate pathologic entity. Immunophenotypically, these tumors are commonly positive for PAX8 (31) and BRAFV600E, which may be used as ancillary tools to differentiate them from squamous cell carcinoma of adjacent mucosal sites (e.g., larynx) and metastases from other organs.
Within the past few years, several groups have published genomic profiles of ATC using NGS techniques (3,4,6,32 –37). Collectively (including the current study), close to 500 ATCs have been sequenced and the most frequent alterations are summarized in Supplementary Table S4. The findings of the current study confirm several findings that have been previously reported, including: (i) BRAF and RAS alterations are mutually exclusive and remain the key oncogenic drivers in ATC, together accounting for 65% of cases (BRAF 38%, RAS 27%) (4,6,32 –36); (ii) TP53 and TERT promoter mutations are highly recurrent events, being present in 62% (range 25–73%) and 50% (range 36–78%) of ATC, respectively; (iii) E1F1AX occurs in ∼10–15% of ATC. It frequently co-exists with RAS mutation and is absent in BRAF-altered ATC (3,4,32); (iv) cumulatively, PIK3CA and PTEN mutations occur in 13% (range 0–18%) and 11% (range 7–18%) of ATC, respectively; (v) PTEN and NF1 mutations often co-exist and are commonly seen in ATCs lacking BRAF or RAS mutations (3,4); and (vi) the frequent co-existence of BRAF and PIK3CA mutations. Similar to prior studies, we have reported rare cases of ATC with CCDC6-RET fusion (3,4,32).
Additionally, we are the first to report ATCs with NTRK fusions: one being NTRK1-IRF2BP2, the other with NTRK2-CRNDE, which may render the patients eligible for TRK-inhibitor targeted therapy. The finding that a large proportion of ATCs have a concurrent DTC component (58% of cases) and harbor the same MAPK pathway driver mutations that are found in DTC further support a stepwise oncogenic process of thyroid carcinoma from DTC to ATC (4,5).
More importantly, our study is the first to report a strong genotype–pathologic phenotype correlation in ATC. BRAF-mutated ATC is associated with a high frequency of DTC (particularly papillary thyroid carcinoma) and a significant higher percentage of squamous cell carcinoma histotype. Although previous studies have demonstrated a correlation between BRAF/RAS mutation status with route of spread in DTC, namely BRAF-mutated tumors tend to spread to regional lymph nodes, whereas RAS-related tumors travel to distant sites (4,13), such difference in tumor spread according to genotype appears to be lost in ATC. Indeed, tumors with either mutations are capable to spread lymphatically (BRAF-mutant: 65%, RAS-mutant: 57%) and hematogenously (BRAF-mutant: 75%, RAS-mutant: 79%). The difference between RAS-mutated and BRAF-mutated ATCs seem to be also blurred at the mRNA expression level. Indeed, Landa et al. did not find difference in the BRAF-RAS-like score (a score based on mRNA expression) between RAS-mutated and BRAF-mutated ATCs (4).
In this study, we demonstrate that BRAFV600E immunohistochemistry is a highly sensitive and specific marker for underlying BRAFV600E mutations in ATC. Two previous smaller studies have reported similar findings, supporting the utility of BRAFV600E immunostain as a rapid screening tool for underlying BRAFV600E mutations in ATC patients (38,39). Recently, clinical trials have shown a dramatic response of BRAF-mutated ATC to combined MEK and BRAF-inhibitor therapy (9), Therefore, recognizing a link between squamous phenotype and BRAF-mutation status and the utility of BRAFV600E immunostain in ATC may expedite the turnaround time for molecular testing and the selection of appropriate patients for FDA-approved dabrafenib and trametinib therapy.
Recently, it was reported that MMR protein deficiency can be seen in up to 14% of ATC and is associated with improved survival (40). In our cohort, eight cases (8%) contain somatic mutations in MMR machinery, including four affecting MSH6, two MSH2, one MLH1, and one MSH6 and MSH2. All 8 tumors appear to be hypermutated with a mutation count of 9–34 (median 16). MMR deficiency does not correlate with any specific ATC phenotype and does not convey a survival advantage: the median survival was 10 months in this group (p = 0.182 comparing ATC with and without MMR gene mutations).
Landa et al. have previously reported that co-occurrence of BRAF/RAS mutation and TERT promoter mutations is associated with a nonsignificant trend toward worse outcome compared with ATCs with TERT mutation alone, BRAF/RAS mutation alone, or neither mutation in 33 ATCs (4). Here, we demonstrate that ATCs with TERT mutations, in particular the BRAF/RAS and TERT double-mutants, are associated with a significantly worse outcome. It is postulated that TERT mutation generates binding motif of ETS families of transcription factors, a downstream effector of BRAF/RAS MAPK pathway, which in turn enhances TERT expression and results in the synergistic effects of TERT and BRAF/RAS mutations in ATC tumorigenesis (4).
In conclusion, based on the data from this large retrospective cohort of ATC with comprehensive clinical, pathologic, and molecular data, resectability and gross residual disease remain the most crucial indicators of outcome in ATC. It is important for pathologists to report encapsulation, margin, percentage, and size of ATC in a primary resection as they seem to provide prognostic information. The co-existence of BRAF/RAS and TERT promoter mutations is indicative of worse prognosis in ATC. The metastatic spread of BRAF-mutated and RAS-mutated ATCs is similar in contrast to its DTC counterparts. BRAFV600E immunostain is a reliable and rapid tool to stratify ATC patient for BRAFV600E -targeted therapy. Finally, pure squamous cell carcinoma of thyroid may be considered as ATC given its frequent association with DTC, its underlying mutations affecting MAPK pathway, and its similar dismal outcome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was supported in part by the Cancer Center Support Grant of the National Institutes of Health/National Cancer Institute under award number P30CA008748. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4