
Abstract
Background:
Several studies have investigated the factors affecting the effects of radioactive iodine (131I) treatment (RAIT) in patients with Graves' disease. However, the influence of dietary or therapeutic iodine on the effect of RAIT has not been fully elucidated yet. The aim of this study was to investigate whether dietary or therapeutic iodine before RAIT influences the therapeutic effects of RAIT with a fixed-dose regimen and a short-term restriction of iodine intake in an iodine-sufficient area.
Materials and Methods:
We retrospectively analyzed 81 Japanese patients with Graves' disease treated with the following RAIT regimen: dietary iodine restriction for 7 days as well as discontinuation of antithyroid drugs (ATDs), potassium iodine (KI), or both for 5 days before RAIT. On the day of RAIT, we measured urinary iodine content to estimate daily iodine intake. After RAIT, we adjusted the dose of ATDs, KI, or both according to serum thyroid hormone levels every 1–2 months. Using the data from these patients, we investigated the effect of dietary and therapeutic iodine on the therapeutic effects of RAIT. The therapeutic effects at 1 year after RAIT were evaluated based on the necessity of ATDs, KI, or both.
Results:
Dietary iodine intake was weakly correlated with 131I uptake (RAIU), but the dose of therapeutic iodine was not correlated with RAIU. The therapeutic effects of RAIT were strongly negatively associated with estimated thyroid volume before RAIT. Neither dietary iodine intake nor therapeutic iodine before RAIT affected this association.
Conclusion:
This study did not find an association between short-term dietary or therapeutic iodine restriction before RAIT and the therapeutic effects of RAIT in an iodine-sufficient area.
Introduction
Radioactive iodine treatment (RAIT) is an optional treatment for Graves' disease that involves the destruction of thyroid epithelial cells via absorption of an inorganic iodine (131I) radioisotope. Thus, the effect of this treatment could be theoretically influenced by the cells' ability to take up iodine. Several previous studies that have investigated prognostic factors for the therapeutic effects of RAIT in a fixed-dose regimen found that thyroid volume (TV) predicts treatment efficacy (1 –3). However, none of these studies elucidated the effect of iodine intake, which may interfere with 131I uptake (RAIU), on the therapeutic effects of RAIT. One reason may be the relatively lower importance of dietary iodine intake restriction in patients with Graves' disease because they have a larger pool of iodine, which requires more thyroid hormone synthesis, than patients with nontoxic goiter or thyroid cancer (4).
In the late 1990s, iodine fortification (universal salt iodization) in many countries contributed to dramatically improve iodine intake status (5). Since iodine intake is a major determinant of RAIU, dietary iodine restriction before RAIT should theoretically be recommended. However, the influence of pre-RAIT iodine intake, including therapeutic iodine, on the therapeutic effects of RAIT has not been elucidated yet in iodine-sufficient areas such as Japan. Based on this background, we retrospectively analyzed 81 consecutive patients with Graves' disease who received RAIT in a fixed single dose (13.0 mCi) to investigate the influence of dietary or therapeutic iodine on the therapeutic effects of RAIT.
Materials and Methods
Patients
Between December 1, 2014, and July 31, 2018, there were 86 consecutive patients (22 male, 64 female) with Graves' disease who received RAIT at the Diabetes and Endocrine Clinics of Juntendo University Hospital. Among the 86 patients, 5 patients who were lost to follow-up at 1 year after RAIT were excluded from the study. Thus, 81 patients were included in this study. RAIT was performed for unresolved hyperthyroidism with medical treatment alone in 41 patients, recurrence of Graves' disease in 12 patients, and antithyroid drug (ATD)-related side effects in 28 patients. Side effects consisted of agranulocytosis in 12 patients, severe liver dysfunction in 7 patients, severe skin rashes in 7 patients, and myeloperoxidase-antineutrophil cytoplasmic antibodies-associated vasculitis in 2 patients. The study protocol was approved by the Ethics Committee of Juntendo University.
RAIT protocol
Our RAIT protocol for a fixed-dose regimen is shown in Supplementary Figure S1. We examined TV using ultrasonography within 3 months before RAIT. We instructed patients not to consume seaweed for 7 days before RAIT to restrict dietary iodine consumption to <50 μg/day, according to the recommendations of the Japan Thyroid Association (Appendix A1). Starting 5 days before RAIT, we instructed patients to discontinue any ATDs, which included methimazole (MMI) and propylthiouracil (PTU), and potassium iodine (KI). The specific drug used for each patient was based on the clinical judgment of the treating physician. All patients were initially treated with ATDs, KI, or both. However, in general, most patients were treated with only ATDs. Patients who were considered to have severe Graves' thyrotoxicosis at the initial visit were treated with MMI and KI to avoid the risk of adverse effects with high doses of ATDs. Patients who experienced adverse effects with ATDs were switched to KI. Patients were instructed to continue taking β blockers and lithium carbonate. On the day of RAIT, we measured urinary iodine and creatinine in the first morning sample and estimated daily iodine intake using the following formula (6):

We treated each patient with a single fixed dose of 131I (480 MBq, equivalent to 13.0 mCi). We resumed ATDs and KI at 48 hours after RAIT, one day earlier than the protocol recommended by the American Thyroid Association in 2016 (7). At 72 hours after RAIT, we measured RAIU and instructed patients to discontinue dietary iodine restriction. We examined serum thyroid hormone levels in the treated patients every 1–2 months and adjusted the doses of ATDs or KI according to serum thyroid hormone levels. ATD discontinuation was based on the clinical judgment of the treating physician. In general, physicians gradually decreased doses of the ATD and KI to the minimum dose (MMI 5 mg/day, PTU 50 mg/day, and KI 25 mg/day). When patients were continuously hypothyroid while taking the minimum ATD or KI dose, we instructed them to discontinue the drugs without considering thyrotropin receptor antibody (TRAb) values. At 1 year after RAIT, we examined TV using ultrasonography again and determined the therapeutic effects of RAIT according to the definitions described below.
Definition of the therapeutic effects of RAIT
Patients who discontinued ATDs, KI, or both within 1 year after RAIT and maintained normal thyroid function with or without levothyroxine (LT4) were defined as patients in remission. On the contrary, patients who needed to continue ATDs, KI, or both to treat persistent Graves' thyrotoxicosis despite RAIT were defined as not being in remission (nonremission).
Measurement of laboratory makers
Blood samples were collected from all patients during clinic visits. Free thyroxine (fT4), free triiodothyronine (fT3), and thyrotropin (TSH) values were measured using commercially available electrochemiluminescence immunoassays (Roche Diagnostics, Tokyo, Japan) with the following normal ranges: fT4, 1.00 − 1.70 ng/dL; fT3, 2.40–4.50 pg/mL; TSH, 0.56–4.30 μIU/mL. Serum TRAb levels were measured using the ECLusys two-step radioreceptor assay (Roche Diagnostics) with a normal range of <2.0 IU/L and a detectable level of ≥0.3 IU/L. Urinary iodine was measured using a chemical assay based on the Sandell–Kolthoff reaction with the microplate method (Hitachi Chemical, Tokyo, Japan) with a measurable range of 25–500 μg/L.
Measurement of TV and RAIU
Estimated TV was computed using the ellipsoid model [(width × length × thickness × π/6) for each lobe + (width × length × thickness) for the isthmus] with ultrasonography. RAIU was performed as follows. A gamma camera (Symbia E; Siemens, Munich, Germany) equipped with a parallel hole collimator was centered over the thyroid at 10 cm. Images were recorded for 60 seconds, with a matrix size 256 × 256 and 2 × zoom. To calculate thyroid uptake based on a standard method, a region of interest (ROI) was drawn around the borders of the thyroid gland. Another ROI in the supraclavicular area was used for background subtraction.
Statistical analyses
Results are presented as medians with interquartile range (IQR) for parameters with skewed distributions. The baseline clinical features of patients in the two groups were compared using the Mann–Whitney U test. The following variables were studied: sex, age, BMI, smoking status, estimated TV before RAIT (pre-RAIT TV), estimated dietary iodine intake, TSH, thyroid hormones, and TRAb on the day of RAIT, daily MMI dose, KI treatment (single use and combination with ATDs), lithium carbonate treatment, and RAIU. Since the potency of MMI is at least 20 times higher than the potency of PTU (8), we considered a PTU dose of 100 mg daily to be equal to an MMI dose of 5 mg daily in this study for statistical analyses. The assumption of multicollinearity was assessed based on correlation coefficients among independent variables. To elucidate factors affecting the therapeutic effect of RAIT at 1 year after RAIT, independent variables were entered into a logistic regression model. All statistical analyses were computed using the Statistical Package for Social Sciences (SPSS, Inc., Chicago, IL) with p-values <0.05 considered to indicate the presence of a significant difference.
Results
Eight-six consecutive patients with Graves' disease were treated with a fixed-dose RAIT regimen. Since 5 patients dropped out during the year after treatment, 81 patients (20 male, 61 female) were included in the final analysis. Table 1 shows the clinical characteristics of the 81 patients with Graves' disease. The mean pre-RAIT TV was 37.2 cm3, and the mean estimated dietary iodine intake was 72.8 μg/day. Among the 81 patients, 48 patients were treated with ATDs only, 25 patients were treated with KI only, and 6 patients were treated with both KI and ATDs before RAIT. The mean absorbed 131I dose, which was calculated at 72 hours after RAIT, was 172 Gy. The mean estimated TV at 1 year after RAIT (post-RAIT TV) was 9.9 cm3.
Characteristics of Patients with Graves' Thyrotoxicosis Who Received 131I (n = 81)
ATD, antithyroid drug; BMI, body mass index; CV, coefficient of variation; fT3, free triiodothyronine; fT4, free thyroxine; IQR, interquartile range; KI, potassium iodine; MMI, methimazole; PTU, propylthiouracil; RAIT, radioactive iodine treatment; RAIU, radioactive iodine uptake; TRAb, thyrotropin receptor antibody; TSH, thyrotropin; TV, thyroid volume.
Among 81 patients, 46 patients (56.8%) became euthyroid or hypothyroid (remission group) and 35 patients (43.2%) remained hyperthyroid (nonremission group). Of note, in the nonremission group, three patients treated with low-dose ATD or block and replacement therapy were very likely able to discontinue ATDs. The nonremission group had a larger pre-RAIT TV than the remission group. The remission group had a higher absorbed dose and a smaller post-RAIT TV than the nonremission group. On the contrary, there were no significant differences in estimated dietary iodine intake, thyroid function, TRAb titers, frequency and therapeutic dose of KI treatment before RAIT, and RAIU between the two groups. The estimated dietary iodine intake in each patient is shown in Supplementary Figure S2. As shown in Supplementary Figure S2, estimated dietary iodine intake in most patients was <350 μg/day, the median estimated dietary iodine intake among the Japanese population (9). Although mean estimated dietary iodine intake was comparable between the groups, three patients in the nonremission group had a markedly higher estimated dietary iodine intake, over 600 μg/day. These three patients had smaller pre-RAIT TV and milder thyrotoxicosis than the 32 other patients in the nonremission group (Supplementary Table S1). Among the three patients, two patients (Patients 1 and 2) who had excess iodine intake (662.7 and 683.5 μg, respectively) had higher RAIU. Thus, excess iodine intake did not appear to prevent RAIU. On the contrary, Patient 3, who had the highest iodine intake (877.9 μg), was treated with high-dose MMI and had lower RAIU.
Next, we investigated the influence of dietary iodine intake and therapeutic dose of inorganic iodine before RAIT on RAIU. Figure 1A shows the relationship between RAIU and estimated dietary iodine intake. RAIU was very weakly and negatively correlated with the estimated dietary iodine intake (R = −0.298, p = 0.007). Furthermore, as shown in Figure 1B, the therapeutic dose of KI treatment was not significantly correlated with RAIU (R = −0.031, p = 0.884).
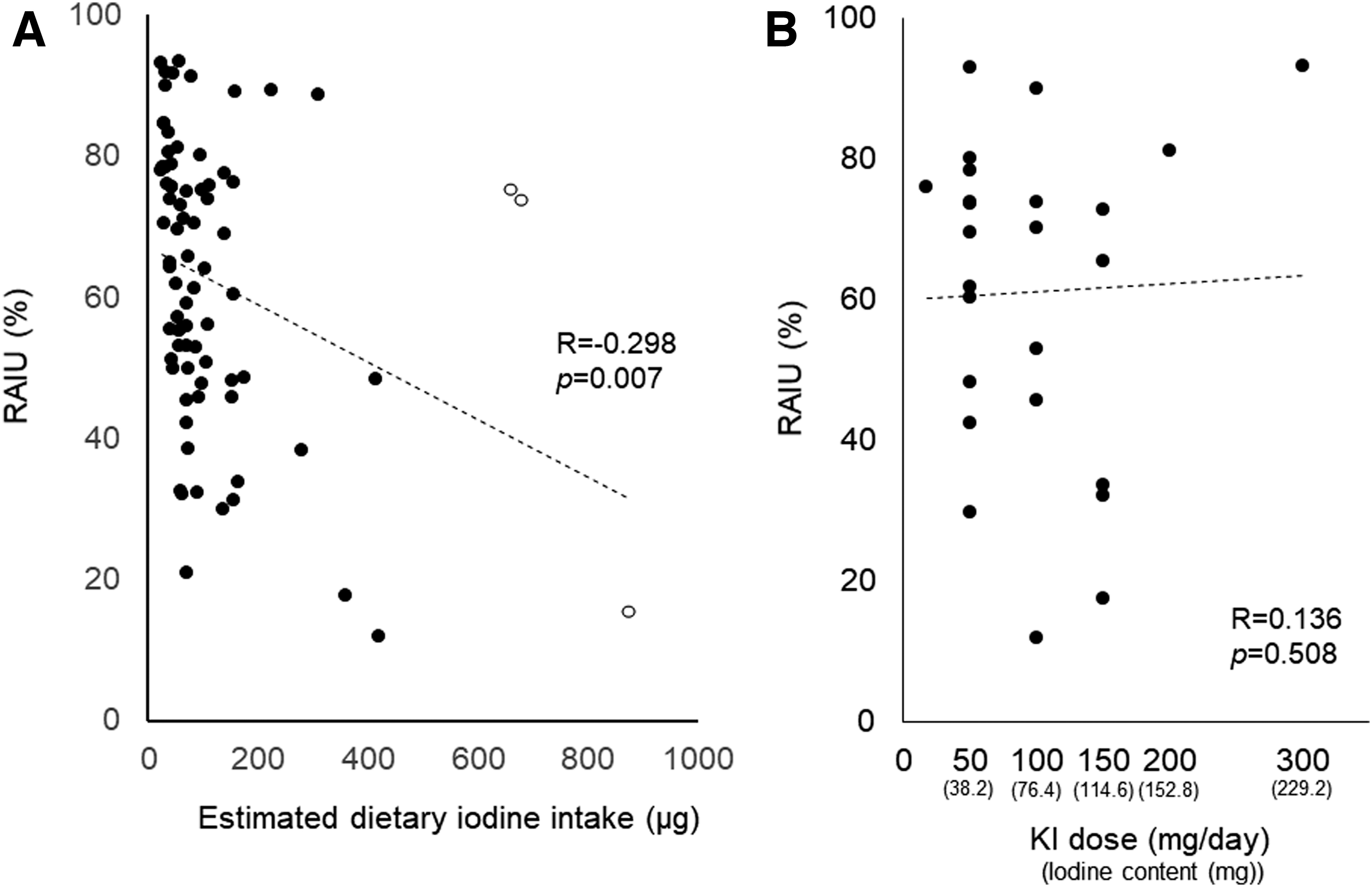
Relationship between RAIU and dietary and therapeutic iodine intake before RAIT. (
Next, we systematically investigated the factors associated with the therapeutic effects of RAIT. Among the clinical factors assessed before RAIT, univariate regression showed that only pre-RAIT TV, not dietary or therapeutic iodine before RAIT, was significantly correlated with the therapeutic effects of RAIT (β = −0.024, p = 0.021) (Supplementary Table S2). Next, we investigated this relationship further using a multivariate logistic regression model. As shown in Table 2, the basic model (model 1) and models that adjusted for KI treatment (model 2), estimated dietary iodine intake (model 3), or both (model 4) showed that pre-RAIT TV is strongly negatively associated with the outcome of RAIT. Model 4 clearly showed that this relationship is independent of dietary and therapeutic iodine (odds ratio = 0.974; 95% confidence interval = 0.956–0.993; p = 0.008).
Multiple Regression Results for the Efficacy of RAIT
Model 1 included sex, age, BMI, pre-RAIT TV, RAIU, TSH, and MMI dose.
Model 2 included the variables in Model 1 and KI treatment.
Model 3 included the variables in Model 1 and estimated iodine dietary intake.
Model 4 included the variables in Model 1, KI treatment, and estimated iodine dietary intake.
The odds ratio in each model indicates the relative fold change in odds for the efficacy of RAIT in 1-g increments of pre-RAIT TV when other variables are held constant.
Based on pre-RAIT treatment, we divided the subjects into the ATD, KI, and ATD + KI groups. We compared the basic characteristics of the patients and treatment effect across groups. As shown in Table 3, the number of patients in the ATD + KI group was small. Thus, we statistically compared several parameters between the ATD and KI groups only. Although the KI group had a smaller pre-RAIT TV than the ATD group, the remission ratio of the two groups was comparable. The ATD + KI group had a numerically higher pre-RAIT TV and lower remission ratio, possibly suggesting that they were resistant to treatment.
Characteristics of Patients with Graves' Thyrotoxicosis Who Received 131I Before RAIT
Only the ATD and KI groups were compared because of the small number of patients in the ATD + KI group.
n.a., not applicable.
We next investigated the effect of discontinuing KI, ATDs, or ATDs and KI 5 days before RAIT on changes in fT3 and fT4 levels. After discontinuation of each drug, both fT3 and fT4 levels significantly increased. However, the degree of change in fT3 and fT4 levels was comparable among the KI, ATD, and ATD + KI treatment groups (Supplementary Fig. S3).
Discussion
In this study, we evaluated the therapeutic effect of RAIT under a general protocol in Japanese patients with Graves' disease. We found that 56.8% of patients with Graves' disease achieved remission at 1 year after RAIT. In terms of factors associated with the therapeutic effect of RAIT, we found that pre-RAIT TV is strongly correlated with therapeutic effects. However, we did not observe an association between dietary or inorganic iodine intake before RAIT and the therapeutic effects of RAIT.
The remission rate observed in this study was similar to rates in previous studies [57.8% (10) and 50.0% (11)] in Japanese patients with Graves' disease (Supplementary Table S3). On the contrary, previous reports from Western countries (1 –3,12,13) showed a higher remission rate for RAIT. In particular, Isgoren et al. (12) reported a higher remission rate for Graves' disease treated with RAIT than the present study, although the duration of ATD discontinuation before RAIT was shorter and the therapeutic dose of 131I used was smaller. Since different therapeutic protocols were used in different studies, it is difficult to assess the precise reasons for the observed differences in the therapeutic effects of RAIT (1 –3,10–12,14). However, these differences could be due to racial differences in response to therapy. Another possibility is the difference in TV before RAIT (Isgoren et al., 32.3 g vs. present study, 37.2 g). However, patients for whom RAIT was unsuccessful at 1 year had a large TV. Previous studies have already demonstrated that an effective absorbed dose of 200–250 Gy is needed to achieve hypothyroidism (15,16) and the therapeutic effects of RAIT depend on the absorbed dose (1). Administered dose and RAIU are positively associated with absorbed dose, whereas TV is negatively associated with absorbed dose. We had to increase the dose administered based on RAIU before RAIT for large thyroids, but we only could use a single fixed dose of 131I to treat all patients in the present study.
In this study, we did not find any evidence that the pre-RAIT dietary iodine intake, KI treatment, or both affected the therapeutic effects of RAIT. Only a few studies have assessed the effect of dietary iodine intake and KI treatment on the therapeutic effect of RAIT. Santarosaet al. conducted a randomized control study to assess the effect of dietary iodine intake restriction before RAIT. The patients included in their study had Graves' disease and >80% of subjects had sufficient or excessive iodine intake at baseline. They randomly allocated these patients into two groups. In one group, the patients were instructed to restrict dietary iodine intake for 2 weeks before RAIT. In the other group, the patients were not instructed to restrict dietary iodine intake. When they compared the therapeutic effects after 6 months between the iodine intake-restricted and nonrestricted groups, they found that dietary iodine was not associated with the therapeutic effects (13). Accordingly, their study suggests that dietary iodine restriction may not be necessary. Overall, our data also suggest that dietary iodine restriction may not be necessary before RAIT. However, as shown in Supplementary Table S1, among the patients who failed to restrict dietary iodine intake, we observed one case in which failure to restrict dietary iodine intake could be linked to poor treatment effect. Thus, we cannot deny the possibility that unlimited intake of dietary iodine may lower the efficacy of RAIT in some patients, although it is also possible that high-dose MMI therapy may reduce the efficacy of RAIT.
Sternthal et al. conducted a key study on the effects of inorganic iodine treatment before RAIT and the therapeutic effects of RAIT in healthy euthyroid subjects without TRAb. Their study investigated the effects of inorganic iodine on RAIU with serial administration of various doses of inorganic iodine (0, 15, 30, 50, and 100 mg/day) for 12 days and RAIU at 12 days after discontinuation of inorganic iodine (17) in healthy subjects. As expected, serial administration of inorganic iodine for 12 days at all doses suppressed RAIU. At 12 days after discontinuation of inorganic iodine, 15 and 30 mg/day of inorganic iodine did not influence RAIU, but ≥50 mg/day of inorganic iodine negatively influenced RAIU. In this study, we also investigated the effect of inorganic iodine treatment with only 7 days of inorganic iodine intake discontinuation, which was shorter than in the study by Sternthal et al. We could not find any differences in RAIU between treatments with KI <50 mg (38.2 mg as inorganic iodine) versus KI ≥50 mg (76.4–229.3 mg). Iodine metabolism within the thyroid could be different between healthy subjects and patients with Graves' disease based on TSH receptor stimulation (17); so it is possible that KI treatment does not significantly affect the treatment effect of RAIT.
This study has several limitations. First, it was a small, single-center observational study. Second, estimated dietary iodine intake was calculated based on a single measurement on the day of RAIT and the formula has not been validated in the Japanese population yet. However, we estimated dietary iodine intake using a standardized approach. Third, we defined remission as normal thyroid function with or without LT4 after discontinuation of ATDs, KI, or both within 1 year after RAIT. However, among the nonremission groups, there could be patients treated with low doses of ATDs who might have been able to discontinue ATDs. However, there were only three patients in this scenario, and so, the impact on the results would not be large. Fourth, the study subjects were patients for whom RAIT was chosen to treat Graves' disease by multiple endocrinologists, which might have resulted in selection bias.
In conclusion, we showed that pre-RAIT TV is a prognostic factor at 1 year after RAIT, and that short-term dietary and therapeutic iodine restriction before RAIT does not appear to affect the therapeutic effects of RAIT. Our data suggest that strict dietary iodine and long-term KI treatment restriction before RAIT may not be necessary. This information may be useful for simplifying RAIT protocols.
Footnotes
Acknowledgments
The authors thank Wataru Miyanaga and Shinichi Arimura for excellent technical assistance.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors did not receive any funding.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Appendix A1. Dietary Iodine Restriction Instructions for Patients Undergoing Radioactive Iodine Therapy