
Abstract
Background:
Maternal subclinical hypothyroidism (SCH) is a risk factor for adverse pregnancy outcomes. However, it is still unclear whether SCH affects male fertility. The aim of this study was to determine the association between paternal SCH and clinical outcomes after in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI).
Methods:
This retrospective study included 2511 couples with paternal euthyroidism (n = 2282) or SCH (n = 229) who visited our clinic for infertility treatment between April 1, 2017, and September 30, 2019. The primary outcomes were the fertilization rate and clinical pregnancy rate; the secondary outcomes were the good-quality embryo rate, blastocyst formation rate, implantation rate, and early miscarriage rate. These outcomes were compared between the euthyroid and the SCH groups after adjusting for various potential confounders.
Results:
The mean paternal ages in the euthyroid and SCH groups were 34.5 and 36.0 years, respectively (p = 0.002). Semen parameters and sperm DNA fragmentation index were similar between the two groups (all p > 0.05). The adjusted fertilization (0.69 vs. 0.71, p = 0.30), good-quality embryo (0.49 vs. 0.52, p = 0.31), blastocyst formation (0.51 vs. 0.53, p = 0.57), and early miscarriage (0.11 vs. 0.10, p = 0.81) rates were also similar between the two groups. There was a significantly decreased adjusted clinical pregnancy rate [confidence interval, CI] and implantation rate [CI] in the paternal SCH group compared with the euthyroid group (0.32 [0.26–0.40] vs. 0.42 [0.40–0.45], p = 0.009 for the clinical pregnancy rate; 0.24 [0.19–0.29] vs. 0.29 [0.27–0.31], p = 0.037 for the implantation rate). Stratified analysis indicated that these differences were only significant in men aged ≥35 years (p = 0.009 and 0.022, respectively) and not in men <35 years (p = 0.39 and 0.45, respectively).
Conclusions:
Paternal SCH was associated with worse clinical outcomes after IVF/ICSI, whereas this detrimental impact was only present in males ≥35 years old. Prospective studies and basic research are warranted to confirm these results and to clarify the mechanisms underlying these associations, respectively.
Introduction
Subclinical hypothyroidism (SCH) is defined as an elevated serum thyrotropin (TSH) concentration coexisting with a normal serum thyroxine (T4) concentration. In our previous study, we identified an association between maternal SCH and decreased ovarian reserve (1). Others have also described associations between maternal SCH and adverse pregnancy outcomes, such as a decreased good-quality embryo rate or clinical pregnancy rate, or an increased risk of miscarriage (2 –5). Women with SCH might therefore benefit from levothyroxine (LT4) supplementation before or during their attempt to conceive (6). However, the effect of LT4 supplementation on naturally conceived pregnancies and pregnancies achieved by assisted reproductive technology (ART) is different: LT4 supplementation significantly decreases the odds of pregnancy loss in pregnancies achieved by ART, but not in naturally conceived pregnancies, among women with SCH. By contrast, LT4 seems to reduce the risks of pregnancy loss and preterm birth in naturally conceived pregnancies, but not in pregnancies achieved by ART, among patients with thyroid autoimmunity (TAI), as indicated by our previously published study (6). These different effects suggest that SCH may influence the fertility of infertile women in a different way from fertile women. Although thyroid hormones (THs) are important in regulating fertility in women, their effects on fertility in men are largely unknown (7).
In the male reproductive system, germ cells, Sertoli cells, and Leydig cells express TH receptors (THRs) (8 –11). THs regulate testis function and spermatogenesis by binding to these THRs to form hormone–receptor complexes, which subsequently activate gene transcription and protein synthesis (8,10). THs also enhance cyclic adenosine monophosphate synthesis and Ca2+ release in spermatozoa. This process enhances flagellar movement and ultimately improves sperm motility (11,12).
SCH represents a subtle deficiency in thyroid function despite the fact that TH concentrations remain within the normal range. Whether such mild thyroid dysfunction in men can affect the clinical outcomes of assisted reproduction is unclear. Here we aimed to investigate the potential effects of paternal SCH on the clinical outcomes of in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI).
Methods
Study approval and informed patient consent
This study was approved by the First Affiliated Hospital of Kunming Medical University, China. All patients provided signed informed consent for the use of personal clinical data in this study before enrolling in an ART treatment cycle.
Study design
This retrospective study was conducted at the Reproductive Medical Center of the First Affiliated Hospital of Kunming Medical University between April 1, 2017, and September 30, 2019. All patients who were evaluated at this fertility clinic were offered screening examinations on the first visit to determine whether further ART treatments were suitable. For men, these examinations were of semen, sperm morphology, sperm DNA fragmentation, and thyroid function. For women, these examinations included transvaginal ultrasonography to determine the antral follicle count (AFC) and biochemical analyses to determine the anti-Müllerian hormone (AMH) concentration, reproductive hormone concentrations on days 2–4 of the menstrual cycle, and thyroid function. All participants were screened for hepatitis, human immunodeficiency virus, and syphilis infection. The demographic and clinical data pertaining to each patient who underwent ART were recorded in a database.
Inclusion and exclusion criteria
Potentially eligible couples (cycles) were included if (i) they were undergoing the first IVF or ICSI cycle with autologous sperm and oocytes; (ii) the male partner had either normal thyroid function or SCH; and (iii) the female partner had normal thyroid function. Couples were excluded if (i) either partner had a history of thyroid disease (treated or not); (ii) either partner had a tumor or a systematic disease, such as hypertension, diabetes, or another endocrine disease; (iii) either partner had chromosomal abnormalities; (iv) the female partner had a uterine abnormality; or (v) no oocytes were aspirated during oocyte retrieval. Finally, 2511 couples were enrolled in the study and their demographic and clinical data were collected for analysis. These couples comprised 2282 clinically euthyroid men and 229 men diagnosed with SCH (Fig. 1).
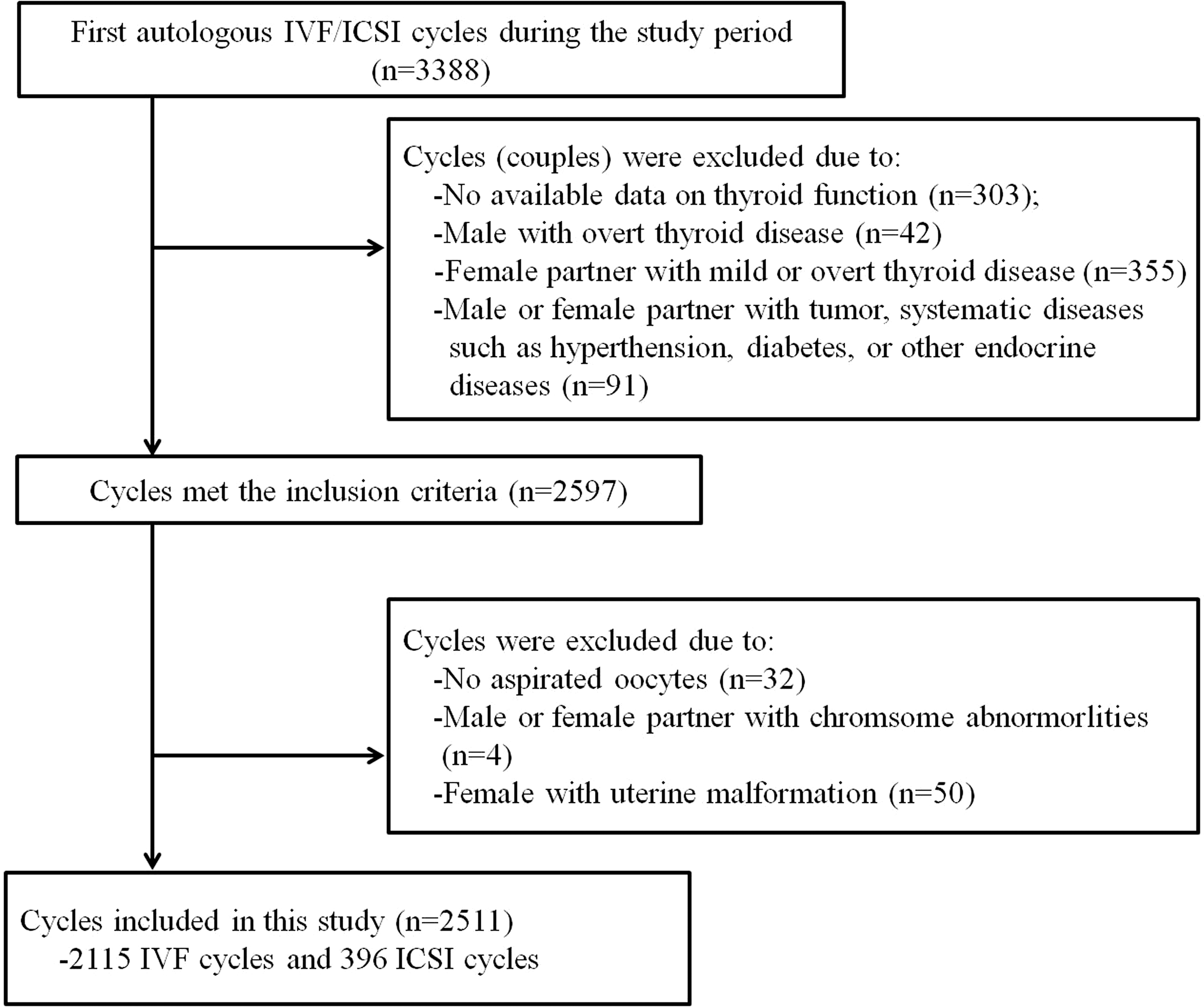
Flowchart for final study population selection.
AFC measurements
The ovarian AFCs were determined on days 2–4 of an unstimulated menstrual cycle. The AFC was defined as the sum of the antral follicles (2–9 mm in diameter) in both ovaries as measured by transvaginal ultrasound during the early follicular phase. All AFC evaluations were performed by the same two highly trained reproductive endocrinologists, as previously described (13).
Thyroid function and AMH concentration measurements
The serum concentrations of TSH, free triiodothyronine (fT3), free thyroxine (fT4), thyroperoxidase antibody (TPO-Ab), and thyroglobulin antibody (Tg-Ab) were measured by automated chemiluminescent immunoassay using a Cobas E601 analyzer (Roche Diagnostics GmbH, Mannheim, Germany), as previously described (14,15). Commercial analytic kits were also purchased from Roche Diagnostics GmbH. The serum AMH concentration was assayed using a commercially available ELISA kit (Kangrun Biotech, Guangzhou, China) with a sensitivity of 0.06 ng/mL, and the data were read on a plate reader (DS2; Dynex Technologies, Chantilly, VA), as previously described (16). The following reference ranges were recommended by the manufacturer: 0.27–4.20 IU/mL for TSH, 3.1–6.8 pmol/L for fT3, 12–22 pmol/L for fT4, <115.0 IU/mL for Tg-Ab, and <34 IU/mL for TPO-Ab. A diagnosis of SCH was made if the TSH concentration was >4.2 mIU/mL, but the fT4 concentration remained within the reference range. A diagnosis of TAI was made if either the TPO-Ab concentration was >34 IU/mL or the Tg-Ab concentration was >115 IU/mL.
Semen analysis
Semen samples were collected by masturbation after two to seven days of sexual abstinence. After liquefaction at 37°C, the samples were examined for the semen volume and the sperm concentration, motility, and morphology. The semen volume was determined from the semen weight, assuming a density of 1.0 g/mL.
To assess the sperm concentration and motility, a 10-μL sample of well-mixed semen was placed in a clean Makler chamber (prewarmed to 37°C), and the sample was covered with a coverslip and immediately examined using a Sperm Class Analyzer (SCA-P-H-02; Microptic S.L., Spain), as previously described (17).
Sperm morphology was evaluated according to the World Health Organization (WHO) criteria, Fifth Edition (18). Briefly, a 10-μL sample of well-mixed semen was placed on a slide to prepare a smear. The sperm were fixed and stained by the Diff-Quick method. All steps were performed using a commercial kit, according to the manufacturer's instructions (Huakang Biomed Ltd., Shenzhen, China). The morphologies of 200 spermatozoa were evaluated under a microscope (CX23; Olympus, Tokyo, Japan) and the proportion of morphologically normal sperm was calculated, as previously described (17). All semen sample analyses were performed by the same highly trained laboratory technician using the same apparatus. According to the WHO criteria (18), semen samples with the following parameters were classified as normal: semen volume ≥1.5 mL, pH ≥7.2, sperm concentration ≥15 × 106/mL, progressive motility ≥32%, and normal morphology rate ≥4%.
Sperm DNA fragmentation determination
Sperm DNA fragmentation was evaluated using a sperm chromatin dispersion test, according to the manufacturer's instructions (Huakang Biomed Ltd.) and as previously described (19). Briefly, a 60-μL diluted semen sample (5–10 × 106/mL) was added to 1% low-melting-point aqueous agarose that had been prewarmed for 5 minutes in a 90–100°C water bath. After careful mixing, 30 μL of this mixture was placed onto a super-coated slide (provided with the kit) and incubated at 4°C for 4 minutes. The slide was then successively immersed in solution A and solution B, and then dehydrated using an ethanol gradient. Finally, the slide was treated with Wright staining solution and air dried. A minimum of 400 spermatozoa were observed under a microscope and scored according to the patterns established by Fernandez et al. (20). The proportion of spermatozoa with DNA fragmentation was defined as the DNA fragmentation index (DFI).
Ovarian stimulation, oocyte aspiration, and embryo transfer
Women were subjected to different ovarian stimulation protocols, including the long GnRH agonist (long protocol, n = 1280), GnRH antagonist (antagonist protocol, n = 762), and mild stimulation protocols (n = 441), as well as other protocols, including 25 natural cycles and 28 progestin-primed ovarian stimulation cycles. The stimulation protocol was selected based on the health condition of the patient, as previously described (21 –23). The long agonist protocol: An adjusted dose (1.00–3.75 mg) of triptorelin (Decapeptyl®; Ipsen Pharma Biotech, Paris, France) was administered according to the patient's weight and body mass index (BMI). The antagonist protocol: A GnRH antagonist (Cetrotide®; Serono, Geneva, Switzerland) was used at a dosage of 0.25 mg/day. The progestin-primed ovarian stimulation protocol: Medroxyprogesterone acetate or dihydrogesterone was used to suppress a premature luteinizing hormone surge during the follicular phase, as previously described (24). The clinician determined the optimal timing and dosage of gonadotropin (Gonal-F®; Merck Serono, Geneva, Switzerland) based on B-ultrasound images and serum hormone concentrations. Recombinant human chorionic gonadotropin (HCG, 250 mg, Ovidrel; Serono) was administered when the two leading follicles reached a mean diameter of 18 mm.
Oocytes were retrieved transvaginally, 34–36 hours after HCG administration, and the follicles were aspirated under transvaginal ultrasound guidance using a single lumen needle attached to a syringe. Semen was prepared by density gradient centrifugation technique, and insemination was carried out by conventional IVF or ICSI. Oocyte fertilization was assessed 18–20 hours after insemination by confirming the presence and location of two pronuclei. The embryos were graded on a scale from 1 to 4 according to the number, size, and shape of the blastomeres and the degree of fragmentation (25). Grade I and II embryos were defined as being of good quality; these embryos were prioritized for transfer. Grade III embryos were only transferred if no grade I or II embryos were available. Blastocyst development was assessed on day 5–6 after considering the degree of expansion and the appearance of an inner cell mass and trophectoderm. Up to three fresh or frozen embryos were transferred, depending on the patient's condition.
Outcome measures
The primary outcome measures in this study were the fertilization rate and the clinical pregnancy rate. The secondary outcome measures were the good-quality embryo rate, blastocyst formation rate, implantation rate, and early miscarriage rate. The fertilization rate was calculated as the number of normally fertilized oocytes (two pronuclei) divided by the total number of oocytes inseminated (IVF cycle) or as per the total number of oocytes injected (ICSI cycle). The good-quality embryo rate was calculated as the proportion of grade I and II embryos among all embryos evaluated on day 3. The blastocyst formation rate was calculated as the number of blastocysts divided by the number of embryos that underwent blastocyst culture. Clinical pregnancy was defined as the identification of a gestational sac with fetal heart activity on ultrasound examination four to five weeks after embryo transfer. The implantation rate was calculated as the number of gestational sacs (observed four weeks after transfer) divided by the number of embryos transferred. The early miscarriage rate was calculated as the number of cycles with pregnancy loss before 12 weeks of gestation divided by the number of cycles resulting in clinical pregnancy.
Sample size calculation
According to previous data analysis, the prevalence of SCH in men attending the Reproductive Medical Center was ∼9% and the proportion of paternal SCH to paternal euthyroidism was ∼1:10. Based on these data, a sample size of 2511 couples (2282 with euthyroidism and 229 SCH) was determined to be sufficient to demonstrate a 10% difference in the clinical pregnancy rate between the two groups, with 85% power and a 5% significance concentration (α). The sample size calculation was performed using PASS 11 software (NCSS, UT).
Statistical analyses
Continuous variables are presented as the means ± standard deviations when normally distributed or as medians (interquartile ranges). A Mann–Whitney U test (continuous variables) or chi-square test (categorical variables) was used to identify differences in the demographic and clinical data between euthyroid men and men with SCH.
The influence of SCH on semen parameters and IVF/ICSI outcomes was analyzed using generalized linear models. To analyze the semen parameters, the model was adjusted for the following confounders in men: age (continuous), BMI (continuous), TAI (categorical), smoking status (categorical), alcohol consumption (categorical), and the duration of abstinence (continuous). To analyze the laboratory outcomes (i.e., the fertilization rate, good-quality embryo rate, and blastocyst formation rate), the models were adjusted for male age, BMI, TAI, smoking status, and alcohol consumption; female age, BMI, and TAI; and primary/secondary infertility (categorical), an infertility diagnosis (categorical), the number of aspirated oocytes (continuous), the ovarian stimulation protocol (categorical), and IVF or ICSI cycles (categorical). To analyze clinical outcomes (i.e., the clinical pregnancy rate, implantation rate, and early miscarriage rate), the models were additionally adjusted for fresh/frozen cycles (categorical), the number of transferred embryos (categorical), and the day of embryo transfer (day 3 or 5–6) (categorical).
A regression analysis stratified by age (<35 and ≥35 years) was performed to investigate whether the association between SCH and IVF/ICSI outcomes differed between younger and older men. To evaluate whether paternal TAI affected the IVF outcome, the patients were further subdivided into four groups: euthyroidism, isolated SCH, isolated TAI, and SCH complicated with TAI (SCH+TAI). The clinical outcomes between these groups were also compared and the potential confounders were adjusted to the above models.
All statistical tests were two sided and a p-value <0.05 was considered statistically significant. SPSS 25.0 (SPSS, Inc., Chicago, IL) was used for the data analysis.
Results
The characteristics of the study cohort
This study included 2511 couples who underwent their first IVF/ICSI cycle and met the defined study inclusion and exclusion criteria. Of these couples, 2282 and 229 were classified into the paternal euthyroid and SCH groups, respectively. The mean age of the men (and their respective partners) in the SCH group was greater than the mean age of the men in the euthyroidism group (male age: 36.0 years vs. 34.5 years, p = 0.002; female age: 33.6 years vs. 32.5 years, p = 0.01, respectively). The mean BMI for the men (and their respective partners) was similar between both groups (p = 0.17 and 0.89, respectively). Men with SCH had a significantly lower fT4 concentration than euthyroid men (median value: 17.35 pmol/L vs. 18.00 pmol/L, p < 0.001). One hundred thirty-two of the 2282 (5.78%) men in the euthyroidism group had TAI, whereas 32 of the 229 men (13.97%) with SCH had TAI (p < 0.001). The frequency of alcohol consumption and smoking in men was similar between the two groups. We observed no significant intergroup differences in the duration of abstinence, semen volume, sperm concentration, sperm morphology, or DFI apart from a slight but significantly lower progressive sperm motility in the paternal SCH group compared with the paternal euthyroid group (35.0% vs. 37.6%, p = 0.04; Table 1).
Characteristics of Study Cohort
Bold p-values indicate a significant difference.
AFC, antral follicle count; AMH, anti-Müllerian hormone; BMI, body mass index; DFI, DNA fragmentation index; fT3, free triiodothyronine; fT4, free thyroxine; IQR, interquartile range; SCH, subclinical hypothyroidism; SD, standard deviation; TAI, thyroid autoimmunity; TSH, thyrotropin.
No association between SCH and semen parameters
After adjusting for potential confounders, we found no significant differences in the semen volume, sperm concentration, progressive sperm motility, sperm morphology, or DFI between the paternal euthyroid and SCH groups (all p > 0.05) (Table 2).
Associations Between Subclinical Hypothyroidism and Semen Parameters (Presented as Adjusted Mean [Confidence Interval])
Adjusted for male age, BMI, TAI, smoking status, alcohol consumption, and duration of abstinence.
The associations between paternal SCH and ART outcomes in couples
The adjusted fertilization rate [confidence interval, CI] in the paternal SCH group was similar to that in the paternal euthyroidism group (0.69 [0.66–0.73] vs. 0.71 [0.70–0.72], p = 0.30). The adjusted good-quality embryo (0.49 [0.45–0.54] vs. 0.52 [0.50–0.53], p = 0.31) and blastocyst formation (0.51 [0.46–0.56] vs. 0.53 [0.51–0.54], p = 0.57) rates were also similar between these two groups. Nevertheless, the adjusted clinical pregnancy rate in the paternal SCH group was significantly lower than that in the paternal euthyroidism group (0.32 [0.26–0.40] vs. 0.42 [0.40–0.45], p = 0.009). The implantation rate in the paternal SCH group was also significantly lower than that in the paternal euthyroidism group (0.24 [0.19–0.29] vs. 0.29 [0.27–0.31], p = 0.037). We observed no significant difference in the early miscarriage rate between these two groups (p = 0.81) (Table 3).
Associations Between Male Subclinical Hypothyroidism and In Vitro Fertilization Outcomes (Presented as Adjusted Value [Confidence Interval])
Bold p-values indicate a significant difference.
Adjusted for male age, BMI, TAI, smoking status, alcohol consumption, female age, BMI, TAI, primary/secondary infertility, infertility diagnosis, no. of aspirated oocytes, ovarian stimulation protocol, and IVF/ICSI insemination.
Adjusted for male age, BMI, TAI, smoking status, alcohol consumption, female age, BMI, TAI, primary/secondary infertility, infertility diagnosis, ovarian stimulation protocol, IVF/ICSI cycles, fresh/frozen cycles, no. of transferred embryos, and day of embryo transfer (day 3 or 5/6).
ICSI, intracytoplasmic sperm injection; IVF, in vitro fertilization.
The associations between paternal SCH and ART outcomes stratified by paternal age
To investigate whether paternal age affects the association between paternal SCH and ART outcomes, we performed a subgroup analysis after stratifying the patients by male age (<35 and ≥35 years). Among men aged <35 years, we found a slight but nonsignificant decrease in the fertilization rate, good-quality embryo rate, blastocyst formation rate, clinical pregnancy rate, and implantation rate in the paternal SCH group compared with the paternal euthyroidism group (all p > 0.05). Among men aged ≥35 years, we also found a slight but nonsignificant decrease in the fertilization rate, good-quality embryo rate, and blastocyst formation rate in the paternal SCH group compared with the paternal euthyroidism group (all p > 0.05). However, the clinical pregnancy and implantation rates in the paternal SCH group were significantly lower than the equivalent rates in the paternal euthyroidism group (adjusted value [CI] 0.18 [0.11–0.29] vs. 0.31 [0.27–0.35], p = 0.009 for the clinical pregnancy rate; 0.13 [0.08–0.21] vs. 0.21 [0.18–0.23], p = 0.022 for the implantation rate). The early miscarriage rate showed a slight but nonsignificant increase in the paternal SCH group compared with the paternal euthyroidism group (0.18 [0.05–0.46] vs. 0.15 [0.11–0.21], p = 0.81) (Table 4).
Associations Between Male Subclinical Hypothyroidism and In Vitro Fertilization Outcomes Stratified by Age (Presented as Adjusted Value [Confidence Interval])
Bold p-values indicate a significant difference.
Adjusted for male age, BMI, TAI, smoking status, alcohol consumption, female age, BMI, TAI, primary/secondary infertility, infertility diagnosis, no. of aspirated oocytes, ovarian stimulation protocol, and IVF/ICSI insemination.
Adjusted for male age, BMI, TAI, smoking status, alcohol consumption, female age, BMI, TAI, primary/secondary infertility, infertility diagnosis, ovarian stimulation protocol, IVF/ICSI cycles, fresh/frozen cycles, no. of transferred embryos, and day of embryo transfer (day 3 or 5/6).
The associations between paternal SCH and ART outcomes stratified by IVF/ICSI cycles
We also evaluated the effect of paternal SCH on ART outcomes according to IVF and ICSI cycles. Of the 2115 IVF cycles, 1916 and 199 men were characterized by euthyroidism and SCH, respectively. The adjusted clinical pregnancy rate [CI] was significantly lower in the paternal SCH group than the paternal euthyroidism group (0.34 [0.27–0.42] vs. 0.43 [0.40–0.45], p = 0.034) in the IVF cycles. Of the 396 ICSI cycles, 366 and 30 men were characterized by euthyroidism and SCH, respectively. The clinical pregnancy rate stratified by ICSI cycles in the paternal SCH group was 13% lower than in the paternal euthyroidism group, but this decrease was not statistically significant (0.25 vs. 0.38, p = 0.15). Compared with the paternal euthyroidism group, the implantation rates were 5% and 9% lower in the paternal SCH group stratified by IVF and ICSI cycles, respectively (adjusted means: 0.25 vs. 0.30 and 0.14 vs. 0.23); however, these differences were not significant (p = 0.11 and 0.07, respectively). We found no significance differences for any of the other outcome measures, including the fertilization rate, good-embryo rate, blastocyst formation rate, and early miscarriage rate (all p > 0.05) between the paternal SCH and euthyroidism groups (Supplementary Table S1).
Associations between male SCH and/or TAI and ART outcomes
To investigate whether TAI affects the association between paternal SCH and ART outcomes, we divided the couples into four groups based on paternal euthyroidism (n = 2150), isolated SCH (n = 197), isolated TAI (n = 132), and SCH+TAI (n = 32). After adjusting for the potential confounders, we found no significant differences in the fertilization rate, good-embryo rate, or blastocyst formation rate among these four groups (p = 0.08, 0.61, and 0.75, respectively). The clinical outcome measures varied significantly between the groups: we detected the highest adjusted clinical pregnancy rate [CI] in the euthyroidism group (0.43 [0.40–0.45]) and the lowest rate in the SCH+TAI group (0.20 [0.08–0.41]). We also found the highest adjusted implantation rate [CI] in the euthyroidism group (0.30 [0.28–0.31]) and the lowest rate in the SCH+TAI group (0.14 [0.05–0.38]). When taking the euthyroidism group as a reference, the other three groups all had a significantly lower clinical pregnancy rate (p = 0.038, 0.043, and 0.007, respectively). The implantation rate in the isolated SCH group showed a slight but nonsignificant decrease compared with the euthyroidism group (p = 0.06); the implantation rates in the isolated TAI and SCH+TAI groups were all significantly lower compared with the euthyroidism group (p = 0.048 and 0.036, respectively) (Table 5).
In Vitro Fertilization Outcomes Between Euthyroid Men and Men with Subclinical Hypothyroidism and/or Thyroid Autoimmunity (Presented as Adjusted Value [Confidence Interval])
Bold p-values indicate a significant difference.
Adjusted for male age, BMI, smoking status, alcohol consumption, female age, BMI, TAI, primary/secondary infertility, infertility diagnosis, no. of aspirated oocytes, ovarian stimulation protocol, and IVF/ICSI insemination.
Adjusted for male age, BMI, smoking status, alcohol consumption, female age, BMI, TAI, primary/secondary infertility, infertility diagnosis, ovarian stimulation protocol, IVF/ICSI cycles, fresh/frozen cycles, no. of transferred embryos, and day of embryo transfer (day 3 or 5/6).
TPO-Ab, thyroperoxidase antibody.
Associations between male TSH levels and IVF/ICSI outcomes
To further investigate the associations between TSH levels and IVF/ICSI outcomes, we divided the couples into three groups according to male TSH levels: euthyroidism (n = 2282), TSH 4.2–8.0 mIU/mL (n = 200), and TSH >8.0 mIU/mL (n = 29). The results showed that the adjusted fertilization rate and good-embryo rate among these three groups were not significantly different. However, the blastocyst formation rate in men with TSH >8.0 mIU/mL was significantly lower than that in euthyroid men (adjusted rate: 0.37 vs. 0.53, p = 0.043). Men with TSH 4.2–8.0 mIU/mL and >8.0 mIU/mL had a significantly lower clinical pregnancy rate (0.34 and 0.21, respectively) than that in euthyroid men (0.42) (p = 0.038 and 0.015, respectively). Implantation rate in men with TSH 4.2–8.0 mIU/mL was nonsignificantly lower than that in euthyroid men (adjusted implantation rate 0.26 vs. 0.30, p = 0.16), whereas implantation rate in men with TSH >8.0 mIU/mL was significantly lower than that in euthyroid men (adjusted implantation rate 0.12 vs. 0.30, p = 0.02) (Supplementary Table S2).
Discussion
To date, most studies have focused on the effects of maternal thyroid dysfunction on pregnancy outcomes. In contrast, very few studies have considered the potential effects of paternal thyroid dysfunction, particularly a mild condition such as SCH, on pregnancy outcomes. To the best of our knowledge, this study constitutes the first evaluation of the potential effects of paternal SCH on ART clinical outcomes and the association between thyroid function parameters and ART clinical outcomes. The SCH prevalence in our cohort was 9.1%. We observed nonsignificant decreases in the fertilization rate, good-quality embryo rate, and blastocyst formation rate in cycles involving men with SCH compared with couples involving men with euthyroidism. Nevertheless, paternal SCH was significantly associated with a decreased clinical pregnancy rate and implantation rate, but was not significantly associated with an early miscarriage rate.
Although SCH is only a mild thyroid dysfunction, this condition might reflect a relatively lower thyroid functional capacity that may become apparent in the future. Others have reported on the negative effects of hypothyroidism on male reproductive function (7,26), and particularly on sperm concentration, motility, and morphology (27,28). Similar observations have been made in animal models (29). Very few studies, however, have focused on the effects of SCH on male reproduction. In 2001, Trummer et al. conducted a study based on 305 patients and found no association between thyroid dysfunction and semen parameters (30). Another study published in 2006 showed that the prevalence of thyroid dysfunction and autoimmunity is comparable between men with normal and men with abnormal semen characteristics (31). In 2015, Lotti et al. (32) conducted a study of 145 euthyroid men and 12 men with SCH and found no significant differences in sperm parameters or seminal fructose concentrations. We also found no significant differences in sperm parameters or DFI between euthyroid men and men with SCH. We did observe a slightly higher DFI in men with SCH compared with euthyroid men (19.7% vs. 18.7%).
Our results suggest that paternal SCH confers negative ART outcomes, although some of the differences in the outcome measurements were not statistically significant. As only a few studies have delineated the mechanistic links between thyroid dysfunction and spermatogenesis, we put forward the following proposals that might help explain the issues. First, animal studies have indicated that a hypothyroid state can affect sperm function (29). An increase in reactive oxygen species production was also observed in sperm isolated from hypothyroid animal models (33). As SCH reflects only a subtle deficiency in thyroid function, it is possible that SCH exerts mild effects on sperm function and the subsequent embryo development. Second, DNA damage in sperm might be another critical factor that mediates poor SCH-induced ATR outcomes. Increased amounts of DNA damage were observed in the sperm of hypothyroid animal models (33,34). A higher DFI has also been associated with lower embryo cleavage rates (35), resulting in a reduced potential to develop into blastocysts (36) and a decreased clinical pregnancy rate (37). The slight but nonsignificant increase in DFI in men with SCH included in this study might have contributed to the observed clinical outcomes. In addition, epigenetic alterations in the sperm might affect embryonic development. Indeed, a previous study based on thyroid rat models reported that THs regulated DNA methylation and histone modifications in astrocytes (38). Spermatozoa contain noncoding RNAs (such as microRNAs, small interfering RNAs, and piwi-interacting RNAs) that are transmitted to the oocyte (39 –41). Animal studies have demonstrated that these noncoding RNAs have important roles in the epigenetic regulation of zygote development and the adult outcomes of the offspring (42). Despite these data, a human-based study has been absent from the literature.
We were interested to note that the differences observed in all laboratory outcomes (the fertilization rate, good-quality embryo rate, and blastocyst formation rate) did not significantly differ between the paternal SCH and euthyroidism groups, whereas the clinical outcomes did significantly differ. This observation can be explained by the fact that embryonic genome activation occurs only after the second cell division, that is, the four- to eight-cell stage (43), and thus is bound to affect only the later stages of embryo development.
Increasing evidence shows that advanced paternal age is associated with dysfunction of reproductive hormone synthesis and sperm production, decreased fecundability, adverse clinical pregnancy outcomes, and increased incidence of some birth defects (44). A recent study showed that paternal age had a 3% decrease in the odds of clinical pregnancy, a 4% decrease in the odds of live birth, a 3.1% decrease in the odds of embryo implantation, and a 5% increase in the odds of miscarriage with each year of age, in IVF/ICSI cycles, independent of female age (45). Increased DFI may be one of the explanations for the adverse clinical outcomes. The DFI increases with age (46,47). In this study, the mean DFI in men aged <35 and ≥35 years was 17.7% and 20.5%, respectively. The percentages of men with a DFI ≥30% were 11.5% and 5.7% in men with SCH and men with euthyroidism, respectively. Aging is also recognized to be associated with more frequent germ cell and sperm DNA mutations (44) and excess reactive oxygen species (48); these pathologic alterations may affect male fertility. Interestingly, SCH was also reported to be associated with these above alterations, as reported in both human and animal models (33,49), indicating that aging may play an additive effect on SCH. This effect could account for the observed phenomenon that only differences in clinical outcomes (clinical pregnancy rate and implantation rate) in older men (≥35 years) were statistically significant. Therefore, this study demonstrates that aging might amplify the impact of paternal SCH on pregnancy outcomes.
Our subgroup analysis showed that paternal SCH significantly affected the clinical pregnancy rate in IVF cycles, whereas for couples who had ICSI treatment, the influence of paternal SCH on clinical outcomes was not significant, although a lower clinical pregnancy rate and implantation rate were observed in the SCH group. Due to the very limited number of patients with SCH receiving ICSI treatment, the impact of paternal SCH on ICSI outcomes is uncertain, and future larger cohort studies are needed.
Like SCH, TAI is also recognized as a mild thyroid dysfunction and might reflect a relatively low thyroid functional capacity that can become apparent in the future (6). This finding could account for the significant decrease in the clinical pregnancy rate and implantation rate in both paternal SCH and TAI groups compared with the euthyroidism group. Our findings suggest that SCH+TAI might further deteriorate thyroid function, thus leading to a further decrease in the probability to achieve clinical pregnancy (Table 5). The impact of paternal TAI on IVF/ICSI outcomes was different from maternal TAI. Busnelli et al. conducted a meta-analysis and showed that maternal TAI did not impact IVF/ICSI outcomes in terms of the likelihood of fertilization, implantation, and clinical pregnancy, whereas TAI may increase the risk of miscarriage and preterm birth and decrease the live birth rate (50). However, for couples receiving ICSI treatment, maternal TAI did not impact laboratory or clinical outcomes, as shown in another recently published meta-analysis by Poppe et al. (51). These results indicated that the impact of TAI on pregnancy outcomes may differ between patients who receive IVF and ICSI treatment. However, further studies are needed before drawing a firm conclusion.
Our study constitutes the first to investigate the association between paternal SCH and ART outcomes, and has several strengths. First, the application of strict inclusion and exclusion criteria ensures the reliability of our results. Second, thyroid function testing was conducted by only two highly trained technicians, to minimize the effects of interassay variability. Third, all embryos were cultured under the same conditions in the same laboratory; the embryologists graded the embryos using standard morphologic criteria and were blinded to the different conditions. Fourth, we adjusted for a series of potential confounders in the data analysis (including lifestyle habits and clinical characteristics) to avoid bias. Despite these strengths, however, some limitations should also be acknowledged. First, this study was based on a retrospective design; therefore, we could not establish a causal relationship. Second, female age in the SCH and euthyroidism groups was not well matched in this study, which may inevitably introduce a selection bias on clinical outcomes, although age was adjusted as a continuous variable in all regression models. It is recognized that female age is one of the most critical factors affecting ART outcomes (52), and therefore, age-matched patients in the SCH and euthyroidism groups may help eliminate the selection bias. Finally, the study participants were patients seeking fertility treatment; therefore, the results of this study might only reflect the effect of paternal SCH on ART outcomes. It remains unclear whether paternal SCH is associated with pregnancy outcomes in couples who conceive naturally.
In conclusion, we found that SCH affected 9.1% of men in our cohort. Paternal SCH was associated with significantly worse clinical outcomes in couples receiving ART treatment who had a male partner ≥35 years old. We also identified a negative effect of TAI on clinical outcomes. Given the retrospective nature of this study, prospective studies and basic research are warranted to confirm our results and clarify the mechanisms underlying these associations, respectively. Randomized clinical trials might also provide high-quality evidence regarding the effects of LT4 supplementation on clinical outcomes following ART in couples with paternal SCH.
Footnotes
Acknowledgments
We are grateful for the patients who participated in this study. We acknowledge the professional article editing services of Armstrong-Hilton Ltd.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (No. 81801416, 81760269), the Technology & Innovation Team of Reproduction and Genetics from Kunming Medical University (No. CXTD201708), the Scientific Funding from the First Affiliated Hospital of Kunming Medical University (No. 2017BS008), the Joint Fund of Science and Technology Department of Yunnan Province and Kunming Medical University under Grant (2017FE467-137); Yunnan Applied Basic Research Project under grant (2018FB126); and Personnel Training Program of Young and Middle-age Academic and Technical Leaders of Yunnan Province under grant (2017HB046).
Supplementary Material
Supplementary Table S1
Supplementary Table S2