
Abstract
Background:
The overall changes of ocular motility in Graves' orbitopathy (GO) are not easily quantifiable with the methods currently available, especially in clinical studies. The aim of the present study was to calculate parameters that quantify the changes of ocular motility in GO in relation to the Gorman score for diplopia.
Methods:
We studied 100 GO patients (Group 1) and 100 controls (Group 2). We also included 30 patients treated with intravenous methylprednisolone (iv-MP), assessed at baseline and after 12 and 24 weeks (Group 3), and 66 patients submitted to squint surgery, assessed at baseline and after 12 weeks (Group 4). Ocular ductions were measured in four gaze directions by a perimeter arc and were used to calculate a total motility score (TMS) as the sum of ductions in each direction; a biocular TMS (b-TMS) as the sum of the TMS of two eyes; and an asymmetry ratio (AR) as the sum of the differences of the corresponding ductions between the two fellow eyes divided by the mean difference found in controls. Quality of life was accessed by a specific questionnaire (Graves' orbitopathy quality of life [GO-QoL] questionnaire).
Results:
TMS and b-TMS were lower, while AR was higher, in Group 1 compared with controls (p < 0.001). In Group 1, TMS and b-TMS were inversely correlated with the Gorman score (p < 0.001) and AR was higher in patients with constant diplopia compared with the others (p < 0.001). In Group 3, TMS and b-TMS increased after treatment in responders to iv-MP (p < 0.001). In Group 4, TMS and b-TMS improved in all patients after surgery (p < 0.01), while AR and GO-QoL score improved only in those without residual constant diplopia (p < 0.001).
Conclusion:
We describe a quantitative method to assess eye motility dysfunction in any stage of GO to be used as an outcome measure in clinical studies.
Introduction
Graves' orbitopathy (GO) has a very heterogeneous presentation and its impact on patients' quality of life is universally recognized, especially when extraocular motility is affected (1,2). The assessment of extraocular motility is of paramount importance when grading the severity of GO and when assessing the outcomes of treatment, but, unfortunately, the overall modifications of eye muscle function are not easily quantifiable with the methods currently available, especially in clinical studies.
The precise measurement of ocular ductions (movements of one eye while the contralateral eye is occluded) is recommended when assessing motility, but this approach has some limitations. For example, the improvement of ductions in one direction of gaze after immunosuppression, if accompanied by deterioration in other gaze directions, may result in worse subjective diplopia and a decrease of the patient's quality of life, even if therapy has successfully inactivated GO.
When evaluating the effectiveness of medical treatment or surgical procedures, the primary endpoint should ideally be measurable as a continuous parameter to allow accurate and reliable statistical analysis. In common clinical practice, such measures may, however, be difficult to obtain, and the outcomes are often reported as dichotomous or discrete parameters, such as active/inactive disease and presence/absence of diplopia. As an example, the Gorman score for diplopia has been the most commonly used parameter in randomized clinical trials studying GO (3,4). This score grades diplopia into four classes according to its severity (absent, intermittent, gaze evoked, or constant), but its categorical nature implies some statistical limitations.
In the present study, we measured parameters derived from ocular ductions in a series of patients with different grades of subjective diplopia. We have subsequently applied these parameters as outcome measures in randomized clinical trials with steroid therapy for active GO and after surgical correction of strabismus. These numerical continuous parameters may offer a large variety of statistical analysis options especially valid in small cohort studies, typical of GO, a rare disease. To be reliable, these parameters should meet the following criteria: (a) be significantly different in GO patients with diplopia and controls; (b) correlate with diplopia graded with the Gorman score; and (c) correlate with the patient's quality of life.
Methods
Patients
We studied consecutive GO patients seen at our joint Thyroid Eye Clinic from January 2015 to April 2017 and controls. The research complied with the Declaration of Helsinki and was approved by our Institutional Review Board (November 22, 2018, No. 2260). Patients were divided into four groups according to their clinical presentation.
Group 1
One hundred GO patients, 74 women and 26 men (aged 15–82 years, mean 53 ± 13.5 years), included in the group were the first 25 consecutive patients for each class of the Gorman score. Patients had either inactive (n = 60) or active (n = 40) GO and of the latter, 36 had moderate–severe disease with a mean clinical activity score (CAS) of 4.1 ± 1 (5).
Group 2
One hundred healthy volunteers, 74 women and 26 men (aged 20–79 years, mean 49 ± 16.1 years), were included in the group.
Group 3
Thirty patients, 8 men and 22 women (aged 27–78 years, mean 53 ± 12 years), euthyroid on methimazole treatment, with active moderate–severe GO (mean CAS 4.6 ± 1.2), undergoing treatment with intravenous methylprednisolone (iv-MP), and receiving a cumulative dose of 7.5 g were included in the group. They were studied at baseline, at the end of treatment (12 weeks), and at 24 weeks of follow-up. Patients with a CAS <3 at 24 weeks were considered responders to steroids.
Group 4
Sixty-six euthyroid patients, 24 men and 42 women (aged 24–85 years, mean 58.4 ± 12 years), with inactive GO were included in the group and studied at baseline and 12 weeks after squint surgery for constant diplopia. Patients without diplopia in straight gaze and downgaze at 12 weeks were considered responders to surgery.
None of the patients were previously treated with orbital radiotherapy.
Calculation of the total motility score, biocular total motility score, and asymmetry ratio
We calculated the total motility score (TMS), biocular TMS (b-TMS), and asymmetry ratio (AR) based on the values of ocular ductions, measured (in degrees) in the four main orthogonal gaze directions (upgaze, abduction, downgaze, and adduction) with a Förster perimeter arc (6,7) (Supplementary Fig. S1A). The TMS was calculated for each eye as the sum of values of ductions, as previously reported (5). The b-TMS was calculated as the sum of the TMSs of the right and left eyes of each patient.
The AR, which is an estimate of the misalignment of the two fellow eyes, was calculated as the sum of the differences of corresponding ductions of the two fellow eyes in each gaze direction divided by the mean difference of ductions found in controls ( = 5.2°). A physiological asymmetry of motility between the two eyes was found in normal individuals (Group 2) as the mean difference of corresponding ductions in these subjects was 5.2° (Supplementary Fig. S1A). Consequently, the AR is expressed as a ratio of the mean physiological asymmetry and is expected to be 0 in few individuals with perfect symmetrical motility between the right and left eyes and around 1 in the majority of controls (Group 2) (Supplementary Fig. S1B). Conversely, GO patients with diplopia are expected to have an AR >1 (Supplementary Fig. S1C, D).
The presence of subjective diplopia was recorded according to the Gorman score for diplopia (0 = no diplopia; 1 = intermittent diplopia; 2 = inconstant or gaze-evoked diplopia; and 3 = constant diplopia). The CAS (8) was assessed in all patients of Group 3, throughout the follow-up. We first studied the relationship of TMS, b-TMS, and AR with the Gorman score and with patients' quality of life to validate the measures in different grades of the disease and subsequently their changes in response to both medical and surgical treatments.
Quality of life
The GO quality of life questionnaire (GO-QoL) (8) was administered to all patients of Group 1, 2, and 3 and was returned by 82/100 (82%), 26/30 (86%), and 27/66 (41%) patients, respectively. Both the visual functioning and appearance scores, as previously reported by Terwee et al. (9), were calculated and correlated with b-TMS and AR.
Statistical considerations
According to results of previous studies by Haggerty et al. (6), Gerling et al. (7), and Mourits et al. (10), the mean reduction of TMS between GO patients with diplopia and controls can be estimated to be between 19% and 27% (Supplementary Table S1).
Assuming that patients with GO without muscle involvement may have TMS values comparable with that of controls, we tested the hypothesis that GO patients with constant diplopia may have a 20% reduction of TMS compared with those without diplopia. To detect this difference with 80% power and a significance level of 0.05, the sample size should be at least 19 subjects for each group.
Thus, we included in the study 100 patients, divided into 4 groups of 25 patients for each class of diplopia, and compared them with a group of 100 healthy controls.
All values are expressed as mean ± standard deviation (SD). The limits of normal values of TMS and b-TMS were calculated as the mean ± 2 SD of the values of normal controls. Analyses by one-way and repeated-measures analysis of variance (with Bonferroni correction), Friedman test or chi-square test, Wilcoxon signed rank or Mann–Whitney test, and the Spearman correlation test were applied, as appropriate. Receiver operating characteristic (ROC) analysis was used to determine cutoff values for the AR, chosen to maximize specificity.
Results
Assessment of TMS, b-TMS, and AR
In GO patients (Group 1) and controls (Group 2), the mean values of ductions and TMS measured in the right eye were not significantly different from those measured in the left eye, in any of the gazes analyzed. As expected, GO patients had mean duction values in all, but downgaze was significantly reduced when compared with controls (p < 0.001) (Table 1). Mean TMS and b-TMS values in GO patients were 14% lower than those of normal subjects (p < 0.001). The range of normal values (mean ±2 SD) for TMS and b-TMS was calculated as 192–232° and 388–456°, respectively. By ROC curve analysis, we determined a cutoff value of 198° and 396° for the TMS and b-TMS, respectively, which best differentiated patients with GO from normal subjects (65% sensitivity and 90% specificity, for both values, data not shown).
Clinical Characteristics and Values of Ductions (in Degrees) Measured in 100 Patients with Graves' Orbitopathy (Group 1) and 100 Normal Controls (Group 2)
Values are presented as mean ± SD, unless otherwise noted.
Chi-square test.
Mann–Whitney test.
AR, asymmetry ratio; b-TMS, biocular total motility score; F, female; LE, left eye; M, male; NS, not significant; RE, right eye; SD, standard deviation; TMS, total motility score.
In contrast, mean AR in GO patients was three times as high as in controls. (Table 1; p < 0.001). This parameter had large variability due to the different degrees of diplopia in Group 1, ranging from absent to constant diplopia. By ROC curve analysis, the optimal cutoff value was 2.64 for AR in patients with diplopia compared with normal subjects. This value had 100% specificity.
Relationship between b-TMS, AR, and diplopia and GO-QoL score
To determine the relationship between b-TMS, AR, and diplopia, we calculated these parameters in patients with GO with different classes of diplopia according to the Gorman score. The values of ductions, TMS, and b-TMS of GO patients without diplopia were not significantly different from those of controls (Table 2). The values of ductions in all, but downgaze, were found to be significantly lower with higher Gorman score grading (Table 2).
Relationship Between Duction Values (in Degrees) and Diplopia in 100 Graves' Orbitopathy Patients Selected According to Their Gorman Score (Group 1) and Normal Controls (Group 2)
The number of patients for each group is indicated in parentheses. p = NS. Tests: one-way ANOVA and post-test Bonferroni's multiple comparison test. All values are expressed as mean ± SD.
No significant differences found between controls and patients without diplopia (Gorman score 0).
No significant differences found between Gorman scores 1 and 2.
No significant differences found between Gorman scores 0 and 1.
Significant differences found only between class 3 and any other class of diplopia and controls.
ANOVA, analysis of variance; GO, Graves' orbitopathy.
Mean b-TMS was 34° (7%), 66° (15%), and 116° (27%) lower in patients with intermittent, inconstant, and constant diplopia, respectively, when compared with the b-TMS of patients without diplopia (Fig. 1A, p < 0.05).
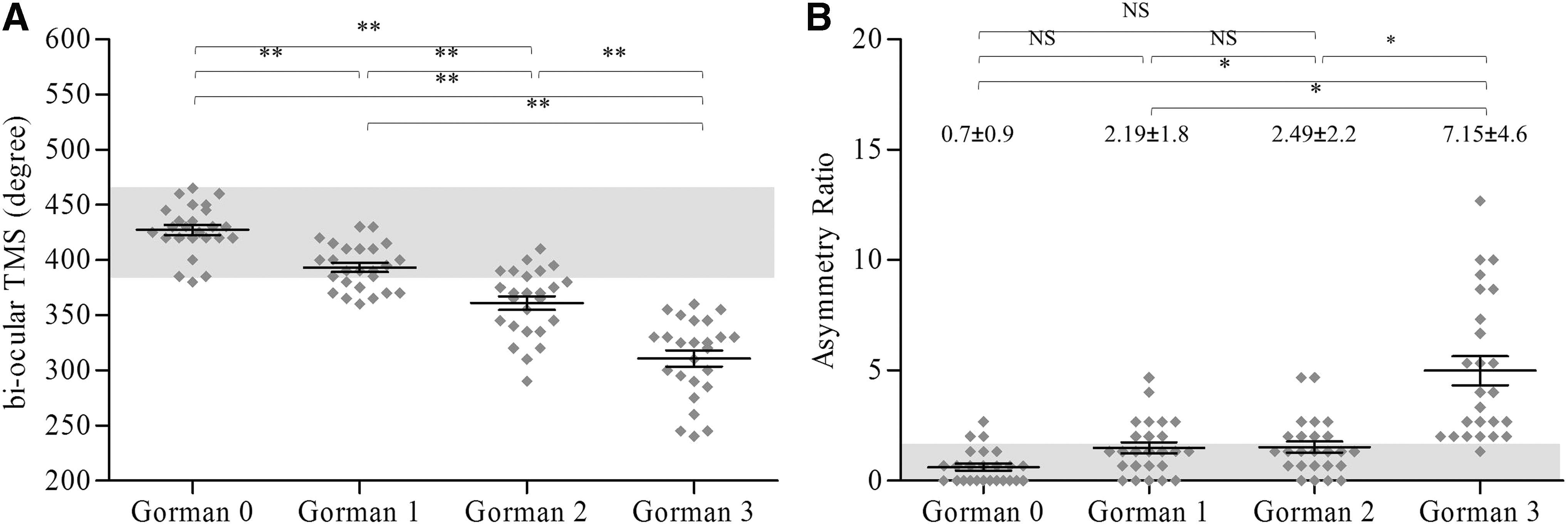
Relationship between the Gorman score and motility parameters of quality of life in 100 patients with Graves' orbitopathy (Group 1). (
The AR was significantly higher in patients with constant diplopia (Gorman score = 3) when compared with controls (Table 2) or patients with lower grades of diplopia (Fig. 1B; p < 0.001).
The mean b-TMS was negatively correlated with the Gorman score (Spearman R = −0.86, p < 0.001; data not shown) and, as expected, the AR positively correlated with the Gorman score (Spearman R = 0.65, p < 0.001; data not shown).
In GO patients, a high diplopia score was significantly associated with a lower score of visual functioning on the GO-QoL (Fig. 2A) and the two parameters were negatively correlated (Spearman R = −0.67; p < 0.001, not shown). As shown in Figure 2, the b-TMS was positively correlated (Fig. 2B) and AR negatively correlated (Fig. 2C) with the visual function score of the GO-QoL.
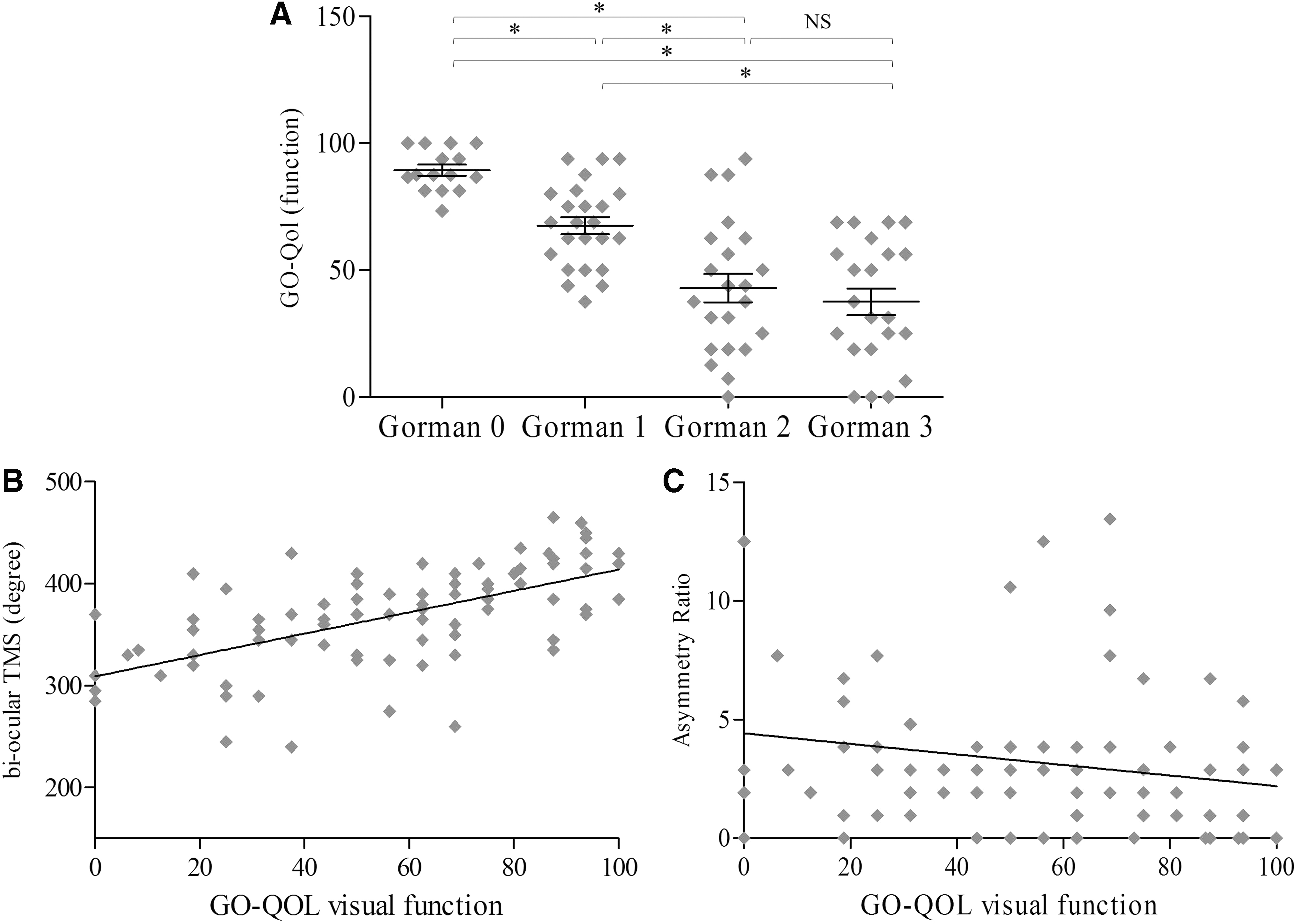
Correlation between motility parameters and the visual functioning score of the GO-QoL in 100 patients with Graves' orbitopathy (Group 1). (
Changes of TMS, b-TMS, and AR in response to immunosuppressive therapy
After having found a relationship between the motility parameters (TMS, b-TMS, and AR) and degrees of diplopia, we studied the usefulness of these parameters in assessing the outcomes of steroid immunosuppressive therapy on extraocular motility and that of strabismus surgery.
Twenty-four of 30 patients (80%) with active GO responded to iv-MP therapy, with a significant reduction of CAS compared with baseline (p < 0.001) (Table 3). Despite disease inactivation, at 24 weeks, their diplopia did not improve when assessed with the Gorman score or with the AR (Table 3). In contrast, the TMS and b-TMS calculated at 24 weeks increased significantly (p < 0.001) compared with baseline values. We also observed a significant improvement in the GO-QoL score. In the six patients unresponsive to iv-MP (20%), the TMS and b-TMS did not change, nor did their GO-QoL scores (Table 3). At baseline, the AR was higher in patients not responding to steroids and although it improved at 24 weeks after therapy, its mean value was still more than twice the upper limit of normal (Table 3). Interestingly, 14 of 30 patients (46.6%), in whom b-TMS normalized after iv-MP treatment, did not require additional medical or surgical treatment (data not shown).
Changes in Motility Parameters (in Degrees) and in the Clinical Activity Score in Patients Responding or Not Responding to Intravenous Steroid Therapy
Values are presented as mean ± SD, unless otherwise noted.
Repeated measures ANOVA.
0 vs. 12 and 24 weeks.
Friedman test.
Wilcoxon signed rank.
12 vs. 24.
CAS, clinical activity score; GO-QoL, Graves' orbitopathy quality of life questionnaire.
Eye motility changes in response to squint surgery
Sixty-six GO patients who underwent rehabilitative surgery for constant diplopia (Group 4) were assessed at baseline and 12 weeks after surgery. Thirty-six patients (54.5%) responded to surgery and had no diplopia in straight gaze and downgaze at 12 weeks. In these patients, the Gorman score, TMS, b-TMS, AR, and GO-QoL score significantly improved after surgery (Table 4). The 30 patients (45.5%) not responding to squint surgery had constant diplopia after surgery and despite improvement in the TMS and b-TMS (p < 0.001), their AR and GO-QoL score did not improve (Table 4). Ten nonresponders were satisfactorily corrected with low-power prismatic lenses, while the remaining 20 were scheduled for additional surgery.
Clinical Outcomes of Squint Surgery: Gorman Diplopia Score, Total Motility Score and Biocular Total Motility Score (in Degrees), Asymmetry Ratio, and Graves' Orbitopathy Quality of Life Questionnaire at Baseline and 3 Months After Strabismus Surgery in 66 Graves' Orbitopathy Patients Affected with Constant Diplopia (Group 4)
Values are shown as mean ± SD, unless otherwise noted. Test: Wilcoxon signed rank.
Mean of the eyes submitted to surgery.
Discussion
In this study, we calculated three parameters of extraocular motility (TMS, b-TMS, and AR) based on the measurement of ocular ductions. Ductions recorded in patients and controls were found to be consistent with those reported by Gerling et al. (7) and Haggerty et al. (6), suggesting that these parameters can be accurate and reproducible measurements when applied to different cohorts of patients affected with different grades of severity of GO.
The TMS, calculated as the sum of the values of ocular ductions, is an index of motility impairment of each eye of a given patient. Accordingly, the b-TMS (the sum of values of the TMS of the two fellow eyes) is an index of the patient's global motility involvement (both eyes). We have also tried to study and quantify the degree of diplopia, being aware of its impact on patients' quality of life, by calculating the AR, an objective index of the asymmetry between the extraocular motility measurements of the two eyes.
The study of ocular ductions is usually performed by observation and grading during the routine orthoptic examination (11). More precise measurements can be obtained by several objective techniques, such as the corneal reflex method (12), the limbus test of Kestenbaum (13), the use of perimetry (Goldmann perimeter or Förster perimeter arc) (7,12), the Harms tangent screen (14), the Maddox tangent scale (15), or the cervical range of motion (16,17). These instruments can be ideally used to calculate TMS, b-TMS, and AR, as long as the same tool is used for patient's follow-up. To date, changes of ductions over time and in response to treatment have been determined by measuring the ductions recorded in each different direction of gaze, eye by eye (7,12,18,19). Unfortunately, this approach may lead to a standstill when judging the effects of medical treatments on ocular motility, particularly when the improvement in one or more directions is accompanied by simultaneous deterioration in other directions of gaze. In this prospect, calculation of TMS and b-TMS may help provide a global measure of ocular motility. Furthermore, when treating GO patients with deterioration of ocular motility, the measurement of changes of TMS and b-TMS may help assess the effects of therapy.
The assessment of diplopia can be based on either subjective or objective methods (20,21). Subjective methods are still the most commonly used methods in both clinical practice and clinical trials. These methods classify diplopia as reported by the patient, according to discrete ordinal scores. Among them, the Gorman score (7) and VISA diplopia score (8) have been the most frequently used scores.
Among methods that objectively assess diplopia, the field of diplopia is currently considered the gold standard (21). It is more frequently plotted using a Goldman perimeter (22), although other technical devices have been proposed (23,24). Within the binocular field of vision, the field of diplopia delimits the area of diplopia from that of single vision. Unfortunately, the results of this examination are commonly assessed as improved or worsened, while the area of diplopia is rarely measured due to the complexity of the calculation. Other scoring systems for quantification of the field of diplopia have been proposed (24), but they are particularly time-consuming.
As shown in the present work, both b-TMS and AR are significantly related to subjective diplopia. The fact that (in patients with GO) diplopia is usually related to progressive restriction of ocular motility explains why the b-TMS decreases and the AR increases with the increase of the diplopia score grading. Our data show that the likelihood to have diplopia increases with worsening of the overall ocular motility, although the b-TMS does not allow distinguishing between symmetrical and asymmetrical eye muscle involvement. Impairment of eye muscles in a cohort of patients with GO is generally asymmetrical, but patients with a low b-TMS and no diplopia may have a symmetrical limitation of ocular motility. The increase of AR was shown to be significant only in patients with the highest grade of the Gorman score (constant diplopia). These findings are strengthened by the observation that in patients undergoing strabismus surgery, the AR improved significantly only in those who successfully responded to surgical correction of diplopia (no diplopia in the primary position and downgaze), but did not in patients with residual constant diplopia after surgery, even when ductions improved. By ROC curve analysis, we were able to determine the cutoff value for AR at 2.64 with 100% specificity when comparing GO patients of Group 1 with controls. The low sensitivity of the test (44%) may be explained by the presence of GO patients without diplopia as the AR of these patients does not differ from that of controls (Table 2). By excluding GO patients with a Gorman score of 0 (no diplopia), the test increases sensitivity to 54% with a better area under the curve (0.77) (data not shown).
Since diplopia is among the major causes of decreased quality of life in patients with GO, we also studied the relationship between b-TMS, AR, and patients' quality of life, as assessed by the GO-QoL (9). As expected, we have found a decrease in the quality of life of patients with a higher degree of diplopia, as measured by the Gorman score grading. Specifically, the visual functioning score of the GO-QoL (which measures the impact of double vision on daily life activities), but not the appearance score (which mainly relates to cosmetic changes), decreased with a higher score of diplopia in patients in Group 1. Such inverse correlation was observed also with the AR, while the b-TMS was positively correlated with the visual function score of the GO-QoL. This suggests that patients' quality of life is not only associated with subjective diplopia, as expected, but can also be related to objective quantitative parameters of extraocular motility.
A limitation of the study is that a comparison between the AR and the field of diplopia was not performed in the training group of patients, who were studied retrospectively. In addition, although a perimeter arc and a Goldman bowl are very simple and widespread instruments, they are currently not easily available as they have been replaced by more modern automated perimeters used in the assessment of the visual field. However, any instrument capable of measuring ductions can adequately calculate TMS, b-TMS, and AR as long as ductions are measured with the same device over time.
In conclusion, the measurement of ductions provides a global assessment of eye muscle function in GO. The TMS, b-TMS, and AR are quantitative parameters that can be used as outcomes of clinical trials, allowing a more gradual and objective measure of the changes of ocular motility, compared with the categorical variables currently in use.
Footnotes
Acknowledgments
The authors thank Sabina di Benedetto, Alessandra Bottari de Castello, Barbara Calonghi, Paola Acanti, and Valeria Minorini for their assistance in the orthoptic assessment of the patients and controls included in the present study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Fondazione IRCCS Cà Granda (Milan, Italy).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1