
Abstract
Background:
Medullary thyroid cancer (MTC) can be associated with significant morbidity and mortality in advanced cases. Hence, we aimed to identify factors at the time of MTC surgery that predict overall survival (OS), disease-specific survival (DSS), locoregional recurrence/persistence (LR), and distant metastases (DM).
Methods:
We performed a retrospective study of clinicopathologic, radiological, and laboratory data in MTC patients who underwent thyroidectomy at Mayo Clinic from January 1995 to December 2015.
Results:
We identified 163 patients (mean age 48.4 years, 48% males), 102 with sporadic MTC and 61 with hereditary disease (n = 46 multiple endocrine neoplasia [MEN] 2A, n = 3 MEN 2B, n = 12 familial MTC) with a median follow-up time of 5.5 years. On univariate analysis, age >55 years, male sex, DM at the time of surgery (M1), lateral neck lymph node (LN) involvement (N1b), gross extrathyroidal extension (ETE), American Joint Committee on Cancer (AJCC) stage 3/4, tumor size (T) 3/4, tumor size, and postoperative calcitonin (Ctn) and carcinoembryonic antigen (CEA) were significant predictors of worse OS and DSS. On multivariable analysis, both gross ETE (hazard ratio [HR] 4.62, 6.58) and M1 (HR 5.11, 10.45) remained significant predictors of worse OS as well as DSS, while age >55 years (HR 3.21), male sex (HR 2.42), and postoperative Ctn (HR 1.002 for every 100 pg/mL increase) were significant only for worse OS. On univariate analysis, male sex, M1, N1b, gross ETE, stage 3/4, T 3/4, tumor size, number of LNs involved, and postoperative Ctn were significant predictors of LR and DM; age >55 years was additionally significant for DM. On multivariable analysis, gross ETE (HR 3.16, 5.93) and N1b (HR 4.31, 4.64) remained significant predictors of LR and DM; ratio of resected/involved LN (HR 10.91) was additionally predictive for LR and postoperative Ctn (HR 1.003 for every 100 pg/mL increase) for DM.
Conclusions:
Disease burden at initial surgery, especially gross ETE, lateral neck LN involvement, and DM, as well as the biochemical response to surgery appear to be more important than demographic factors in terms of MTC prognosis. These findings highlight the importance of rigorous perioperative assessment to better predict MTC outcomes.
Introduction
Medullary thyroid cancer (MTC) is a neuroendocrine tumor that accounts for up to 5% of all thyroid cancer cases in the United States (1). MTC is different from the other more common types of thyroid cancers (papillary and follicular) because it originates from the parafollicular C cells of the thyroid gland. MTC often spreads to lymph nodes (LNs) in the neck or metastasizes to other organs (1). In 25% of cases, this cancer is inherited, and in some of the inherited forms, it can be associated with other endocrine tumors, in syndromes called multiple endocrine neoplasia (MEN) 2A and MEN 2B (1). The primary curative treatment for MTC is total thyroidectomy, usually accompanied by at least central neck dissection. More extensive surgery and adjuvant therapies such as external-beam radiation therapy and tyrosine kinase inhibitors are generally reserved for more advanced disease.
Unfortunately, 70% of patients with MTC who present with a palpable thyroid nodule have cervical nodal metastases and 10% have distant metastases (DM) (1). Classically, older age and higher stage of disease at the time of diagnosis have been shown to be the strongest predictors for poor prognosis in MTC (2 –4). The risk designation based on the tumor (T), node (N), and metastases (M) staging system has recently been updated by the American Joint Committee on Cancer (AJCC) from the seventh to the eighth edition (5). Our institution previously reported on 65 MTC patients from 1946 to 1970, supporting higher stage as a strong predictor for worse survival (6). However, many of the reported studies did not evaluate the significance of tumor markers as predictors for outcomes.
The Revised American Thyroid Association (ATA) Guidelines for the Management of Medullary Thyroid Carcinoma recommend measuring serum calcitonin (Ctn) level 3 months after surgery to determine the need for further workup of persistent disease (1). A recent study (7) reported on Ctn levels postoperatively within 1 week of surgery, but long-term follow-up was not provided to determine whether early postoperative Ctn normalization correlates with long-term biochemical and structural cure. The prognostic value of tumor marker doubling time has also been reported (1), with doubling time of <6 months demonstrating the highest and >2 years showing the lowest rate of persistent or recurrent disease. However, in most cases, the disease has already progressed or recurred concomitant to the elevation of tumor markers. Hence, it is essential to analyze factors at the time of MTC diagnosis and initial surgery that could predict the disease course and outcomes. A few studies have evaluated these predictors (7 –11), while other studies have evaluated factors that influence postoperative biochemical cure and found that higher stage, higher preoperative Ctn level, larger primary tumor size, gross extrathyroidal extension (ETE), and cervical LN metastases were associated with a lower rate of biochemical cure (12 –16). However, most of these studies did not stratify sporadic and familial MTC patients, and some included patients with C cell hyperplasia who underwent prophylactic thyroidectomy. These observations underlie the importance of investigating a large MTC cohort managed and followed closely to further identify perioperative factors that affect long-term outcomes.
Materials and Methods
Study population
After obtaining approval from our institutional review board (IRB), we performed a retrospective analysis of all patients with a diagnosis of MTC who underwent thyroid surgery at Mayo Clinic, Rochester, from January 1, 1995, through December 31, 2015. A total of 172 patients were identified from a comprehensive database of MTC at our institution. After excluding those with a diagnosis of C cell hyperplasia without MTC (n = 4) and those without research authorization (n = 4) or any follow-up after surgery (n = 1), we included 163 patients for analysis in this study.
Management and monitoring protocols
Preoperatively, all patients had a comprehensive neck ultrasound and 152 had serum Ctn level measured. In patients with preoperative Ctn >500 pg/mL, additional imaging was obtained before surgery, which in most cases included computed tomography (CT) scan of the chest and abdomen, and in some cases, 18-fluorodeoxyglucose (18FDG)-positron emission tomography (PET) scan was performed as well. All included patients had thyroidectomy performed at our institution. Those with suspicious lymphadenopathy had preoperative fine needle aspiration (FNA) of any suspicious LN. Most patients (95%) had central neck dissection, but lateral neck dissection was performed selectively only in those patients with documented lateral neck nodal involvement preoperatively. All patients received replacement doses of levothyroxine postoperatively and were regularly followed with physical examination and thyroid function testing. The postoperative serum Ctn and/or carcinoembryonic antigen (CEA) levels were also measured every 6–12 months. Neck ultrasound was performed during the first 6–12 months after initial surgery and repeated thereafter at 12–24 months of intervals. If postoperative serum Ctn levels were elevated or demonstrated rising patterns, which were discordant with neck ultrasound, additional diagnostic imaging studies were performed, including neck/chest CT scan, magnetic resonance imaging of the liver, pelvis, and axial skeleton, bone scintigraphy, and/or whole-body 18FDG-PET/CT.
Study measures
Demographic and clinical data including information regarding the perioperative evaluation, surgical procedure, histopathology, tumor (T) size, LN involvement, presence of central neck LN metastases (N1a), lateral neck LN metastases (N1b), DM at the time of thyroidectomy (M1), surgical outcome and subsequent follow-up (including need for reoperations), recurrence/persistence status, and disease-specific and all-cause mortality as of last visit were recorded. Multifocal disease was defined as more than one MTC focus in a single thyroid lobe, while bilateral disease was defined as the presence of at least one MTC focus in both lobes. Laboratory data for tumor markers were also collected. All laboratory testing was performed at the Mayo Medical Laboratory, Rochester, Minnesota. The main outcome measures were overall survival (OS), disease-specific survival (DSS), locoregional recurrence/persistence (LR), and occurrence of DM. OS and DSS were analyzed by evaluating time from thyroidectomy until the most recent follow-up or death.
Statistical analyses
Categorical variables are described as number and percentage, and continuous variables are described as median and range or mean and standard deviation depending on their distribution.
Univariate and multivariable Cox proportional hazard models were used to examine predictors of OS, DSS, LR, and DM. We included variables from the univariate analysis that were highly statistically significant (p < 0.001) due to the limited number of outcome events. Highly overlapping or collinear predictors were entered into the models in order, based on clinical decision and magnitude of effect or hazard ratio (HR) for categorical variables. Statistical analyses were conducted using SAS (version 9.4; Cary, NC).
Results
Demographics and disease characteristics
The study included 163 patients (mean age 48.4 ± 18.8 years, 47.9% males), of whom 61 (37.4%) had a hereditary form of MTC, and 46 (75.4%) of them were diagnosed by family screening. The median follow-up duration after initial surgery was 5.5 years (range 0.002–20.6), 6.3 years in sporadic, 5.3 years in hereditary diagnosed by screening, and 4.5 years in hereditary diagnosed by clinical or radiographic findings. Among those with hereditary MTC, 37 had moderate risk, 14 had high risk, and 3 had highest risk REarranged during Transfection (RET) germline mutations according to the ATA classification in the revised MTC guidelines (1). Among hereditary MTC patients, RET mutation was not identified in 5 patients and not tested in 1 patient, but these were classified as familial on the basis of very strong family history (>2 family members, most often first-degree relatives with proven MTC). On initial presentation, 71 (43.6%) patients had a palpable neck mass. Surgical pathology revealed that the mean largest tumor size was 1.9 ± 1.7 cm. MTC was bilateral and/or multifocal in 28.2% of the patients. Patients with hereditary MTC had more multifocal (50.8% vs. 15.7%; p < 0.001) and bilateral (59% vs. 9.8%; p < 0.001) disease compared with those with sporadic MTC. Total thyroidectomy with at least central neck dissection was performed in 95% of our cohort. We used both AJCC seventh and eighth editions of TNM staging for our study and found that the stage of MTC in our cohort did not differ between the two. Pheochromocytoma was diagnosed in 13 patients and primary hyperparathyroidism in 5 patients, all with hereditary MTC. Patient characteristics separated by sporadic, hereditary diagnosed by screening, and hereditary diagnosed by clinical or radiographic findings are presented in Table 1.
Baseline Characteristics of Medullary Thyroid Cancer Patients at the Time of Initial Presentation and Surgery
Categorized by both AJCC seventh and eighth editions.
Available for 152 patients.
AJCC, American Joint Committee on Cancer; CEA, carcinoembryonic antigen; Ctn, calcitonin; FMTC, familial medullary thyroid cancer; LN, lymph node; MEN, multiple endocrine neoplasia; RET, REarranged during Transfection; SD, standard deviation.
Predictors of OS and DSS
The 5- and 10-year OS were 89.8% [confidence interval, CI, 84.8–95.0] and 81.2% [CI 74.0–89.2], respectively. On univariate analysis (Table 2), age >55 years (HR 3.72), male sex (HR 3.45), M1 (HR 9.22), gross ETE (HR 5.51), AJCC tumor stages 3 and 4 versus 1 and 2 (HR 5.39) (Fig. 1a), T category 3 and 4 versus 1 and 2 (HR 5.01), N1b (HR 3.74), tumor size (HR 1.36 for every centimeter increase in tumor size), 5 or more LN involvement (HR 2.50), ratio of involved/resected LN (HR 3.84), and Ctn (HR 8.63 for value >500 pg/mL) (Fig. 2) and CEA levels measured 3–6 months postoperatively were significantly associated with worse OS. On multivariable analysis (Table 2), age >55 years, gross ETE, M1 status, and every 100 unit increase in postoperative nadir Ctn level were associated with worse OS. Male sex and N1b status were not predictors of OS in multivariable analysis.

(

Overall survival comparing MTC patients with postoperative Ctn >1000 pg/mL vs. 10–5000 pg/mL vs. 0–10 pg/mL (p = 0.008). Ctn, calcitonin.
Predictors of Overall and Disease-Specific Survival in Medullary Thyroid Cancer
The effect of male sex was not statistically significant when this was added to the multivariable model. When we added M1, N1b, and Ctn/CEA into the multivariate model, M1 but not N1b or Ctn/CEA was a significant predictor for worse overall survival.
Categorized by both AJCC seventh and eighth editions.
For every 1 unit increase in ratio.
For every 100 pg/mL increase in Ctn.
CI, confidence interval; DSS, disease-specific survival; HR, hazard ratio; OS, overall survival.
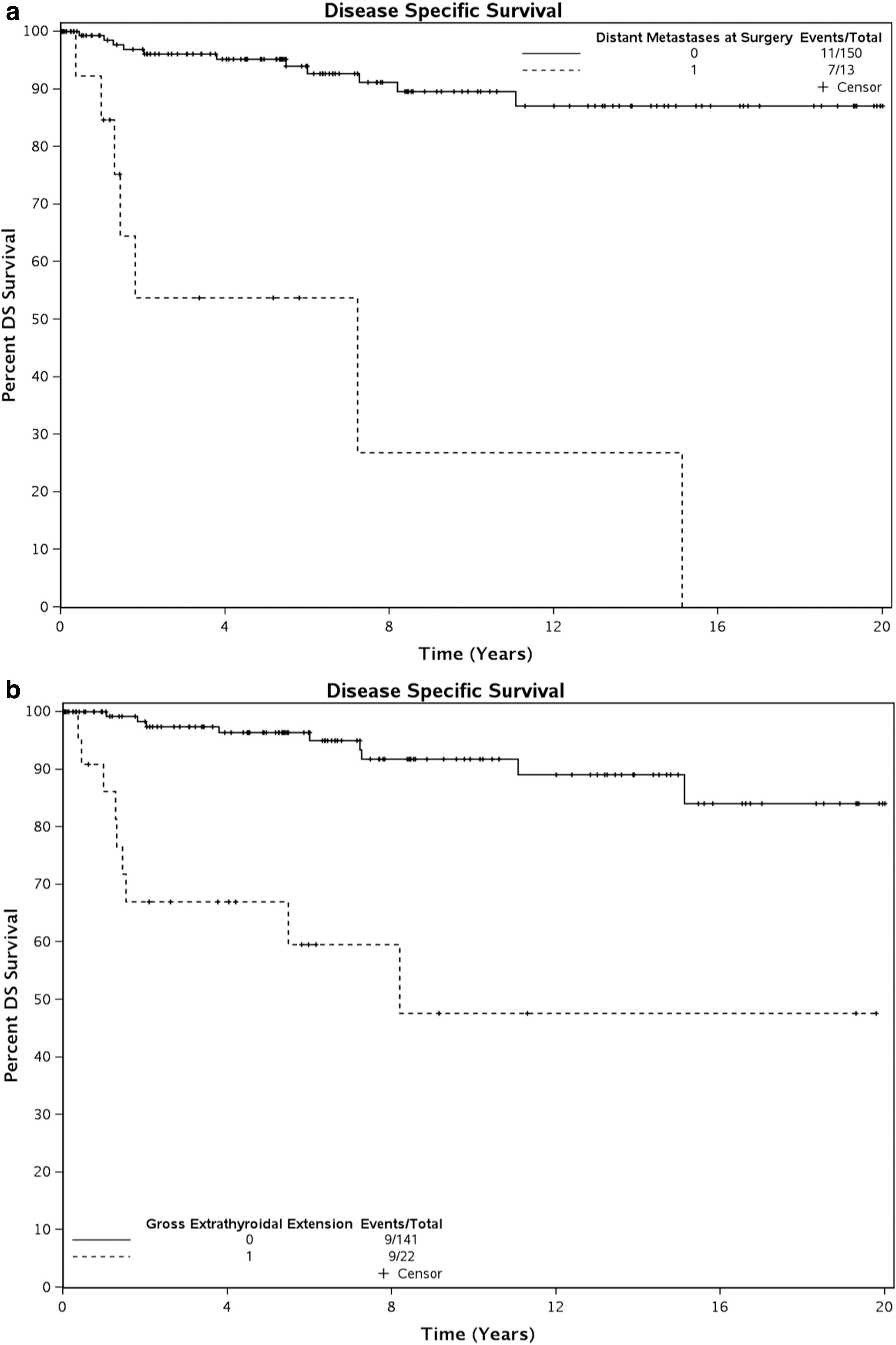
The 5- and 10-year DSS were 91.9% [CI 87.5–96.6] and 85.2% [CI 78.4–92.7], respectively. On univariate analysis (Table 2), age >55 years, male sex, M1 (Fig. 3a), N1b, gross ETE (Fig. 3b), tumor stages 3 and 4 (Fig. 1b), T category 3 and 4, tumor size, 5 or more LN involvement, ratio of involved/resected LN, Ctn at diagnosis, and Ctn and CEA levels measured 3–6 months postoperatively were associated with worse DSS. On multivariable analysis (Table 2), only gross ETE and M1 status were associated with worse DSS. To determine whether outcomes have changed over time, we compared 10-year survival rates in MTC patients who underwent thyroidectomy between 1995 and 2005 (OS 80.6% [CI 70.8–91.7] and DSS 84.0% [CI 74.7–94.3], respectively) with those who had surgery in the second decade of our study, from 2006 to 2015 (OS 82.2% [CI 71.8–94.2] and DSS 86.7% [CI 76.9–97.8], respectively), and found that there was no statistically significant difference in 10-year OS (p = 0.71) or DSS (p = 0.60).
(
Predictors of LR and DM
LR occurred in 16 (9.8%) patients, of whom 13 had sporadic MTC, 2 had hereditary MTC diagnosed by clinical or radiographic findings, and 1 had hereditary MTC diagnosed by screening. DM occurred in 25 (15.3%) patients including 23 (22.5%) with sporadic MTC, 1 (7.0%) with hereditary MTC diagnosed by clinical or radiographic findings, and 1 (2.2%) with hereditary MTC diagnosed by screening. Among those with LR (n = 16) or DM (n = 25) during follow-up, only two had postoperative nadir Ctn <10 pg/mL suggesting that most of these patients had persistent locoregional or distant disease. The median time to LR was 4.2 years (range 0.1–15.5) and the median time to diagnosis of DM was 2.8 years (range 0.3–17.8). On univariate analysis (Table 3), male sex, M1, N1b, gross ETE, AJCC stages 3 and 4 versus 1 and 2, T category 3 and 4 versus 1 and 2, tumor size, involvement of 5 or more LN, ratio of involved/resected LN, and postoperative Ctn were significant predictors of LR and DM; age >55 years was additionally significant for DM. On multivariable analysis (Table 3), gross ETE (HR 3.16, 5.93) and N1b (HR 4.31, 4.64) remained significant predictors of both LR and DM; ratio of involved/resected LN was additionally significant for LR, while postoperative Ctn (HR 1.003 for every 100 pg/mL increase) was additionally significant for DM.
Predictors of Locoregional and Distant Metastases or Recurrence in Medullary Thyroid Cancer
Categorized by both AJCC seventh and eighth editions.
For every 1 unit increase in ratio.
For every 100 pg/mL increase in Ctn.
DM, distant metastases; LR, locoregional recurrence/persistence.
Discussion
In this cohort study of 163 MTC patients treated at our institution with a median follow-up of 5.5 years (range 0.002–20.6), we evaluated demographic, clinicopathologic, and laboratory factors in the perioperative period to identify predictors of long-term outcomes. Our cohort was mostly similar to previously reported multicenter cohorts (4,10,17) and large institutional series (18) in terms of patient demographics. However, 38% of our cohort had a hereditary form of MTC, which is higher than 18–24% reported in some studies (10,17). This is likely because many MTC families are followed at our institution, leading to a higher frequency of screening and diagnosis of hereditary MTC. MEN 2A was the most frequently diagnosed hereditary MTC syndrome. Compared with patients with sporadic MTC, those with hereditary forms of MTC had more bilateral and multifocal disease on presentation and had moderate risk RET mutations similar to another study (17). Patients with hereditary MTC also underwent surgery at a younger age (36–38 years) compared with those with sporadic MTC (56 years). Patients with hereditary MTC diagnosed by screening presented with stage 1 or 2 disease in 85% of cases compared with 36% of patients with sporadic MTC. In the entire cohort, 8% of patients presented with M1 and about one-third with N1b, findings that were more frequent in sporadic than in hereditary MTC. Also, more patients with sporadic MTC had postoperative nadir Ctn levels >150 pg/mL and higher CEA levels compared with patients with the hereditary forms of MTC. These differences could account for favorable long-term outcomes in most patients with hereditary disease in our cohort, similar to those in other studies (3,10,19). Overall, most patients had stage 1 (38%) or stage 4 (36.2%) disease, which is similar to the distribution observed in other large cohort studies (10,17,18).
The favorable survival rates in our study are in line with other reports of favorable long-term outcomes in most MTC patients reported recently (10,11,16 –18). Jung et al. reported improved 5-year recurrence rate but no difference in 5 year OS in 2006–2012 compared with 1982–2005 (11). In our study, comparison between 1995–2005 and 2006–2015 did not show any statistically significant differences in OS or DSS; however, even though statistical analysis was not possible, our cohort did demonstrate an improvement in survival rates compared with the 10-year OS (81.2% vs. 63%) and DSS (85.2% vs. 69%) observed in the historical Mayo cohort from 1946 to 1970 (6). Some possible reasons for this improved trend in survival rates may be the performance of more extensive surgery with routine central neck LN dissection, availability of tumor markers, and higher resolution imaging modalities in recent years. In another study, 10-year OS rates for patients with stages 1, 2, 3, and 4 MTC have been reported to be ∼100%, 93%, 71%, and 21%, respectively (3). In our study, demographic characteristics such as age >55 years and male sex predicted reduced survival, but the effect of sex on survival was not present when adjusted for other variables. There have been conflicting results in the literature regarding the effect of sex on MTC outcomes, with only two studies reporting male sex as a significant predictor of worse DSS at a population level (16,19). Younger age has been associated with better MTC survival, which may be conceived as a surrogate of early diagnosis especially in hereditary MTC; however, in our study, even after accounting for MTC type, age >55 years was a predictor of worse OS. Similar to other large series (3,11,16 –18), including the postoperative nomogram suggested by Ho et al. (8), we found classically described MTC characteristics, including higher Ctn and CEA at diagnosis, N1b, M1, gross ETE, higher AJCC stages (3 and 4), and larger primary tumor size to be associated with worse OS and DSS. Additionally, we found that higher Ctn levels evaluated 3–6 months post-thyroidectomy were associated with worse survival, a finding similar to some other studies (3,18). Older age and higher stage of disease have been reported in other studies to be significant predictors for worse survival (2 –4). Twito et al. recently reported that presence of DM and gross ETE are associated with worse DSS (17). On multivariable analysis in our study, the effect of N1b status on OS and DSS was not statistically significant after accounting for M1 status, likely because all patients with M1 also had N1b disease. We did find that age >55 years, male sex, gross ETE, M1, and high postoperative Ctn predicted worse OS, while gross ETE and M1 were the only factors that significantly predicted worse DSS. Hence, these factors would be most important when prognosticating MTC outcomes, of which M1 status portends the highest risk for worse survival. The effect of sex on survival lost significance after adjusting for postoperative Ctn, suggesting that a part of the influence of sex on MTC survival may be related to the higher burden of disease in men who might present at a more advanced stage.
The overall frequencies of LR and DM in our study were higher than previously reported at our institution (6). Factors accounting for this difference could be the increasingly sensitive diagnostic tools such as high-resolution ultrasonography and higher quality CT scanners, and the fact that tumor markers such as Ctn and CEA were not routinely available at the time of analysis of the previous study. In our study, there was a trend toward lower rate of LR and DM in hereditary MTC diagnosed by screening compared with hereditary MTC diagnosed by the presence of clinical or radiographic findings and sporadic MTC; however, due to limited number of events, we could not perform statistical comparisons. This trend is likely the result of earlier diagnosis with less disease burden at the time of initial surgery in patients with hereditary forms of MTC, especially in those diagnosed by screening, underpinning the importance of genetic counseling and proactive screening of patients. Age >55 years at the time of initial surgery and male sex were associated with higher risk of DM, while only male sex was associated with risk of LR. We found classically described MTC characteristics including N1b, M1, gross ETE, higher AJCC stages (3 and 4), and larger primary tumor size to be predictive of both LR and DM. In addition to these, ratio of involved/resected neck LN predicted DM and higher postoperative Ctn predicted both LR and DM. The results of biochemical factors are similar to those reported by others where high postoperative Ctn (absence of postoperative biochemical cure) predicted persistent disease and structural recurrence on long-term follow-up (9,11). Multivariable analyses by Twito et al. demonstrated that gross ETE and presence of DM at the time of diagnosis were predictors of disease persistence or recurrence (17). In our study, multivariable analysis was limited by the small number of events, thus limiting the power, but revealed that gross ETE and N1b predicted LR as well as DM, while high postoperative Ctn was additionally predictive of DM. This highlights the importance of a comprehensive preoperative neck ultrasound, routine central neck dissection, and additional lateral neck dissection when suspicious lymphadenopathy is identified in the lateral compartment, preferably after FNA confirmation. The predictive nature of postoperative Ctn level for DM underlies the importance of incorporating 3–6 months postoperative biochemical data to the initial tumor burden assessment when aiming to predict the long-term risk of disease spread.
Our study has several strengths and limitations. The main strength is that the management and close follow-up of patients occurred at a tertiary care center by a highly specialized team of thyroidologists, oncologists, and thyroid surgeons. The completeness of data in terms of MTC characteristics, genetic status, postoperative Ctn testing, and fairly long follow-up are also strengths of this study. The sample size was large enough to evaluate predictors for survival and disease recurrence/persistence; however, a limitation is that the number of outcome events was not large enough to separately evaluate these predictors within different MTC types or to perform more extensive multivariable analyses. In our study, multivariable analysis after adjusting for factors significant on univariate analysis was limited by the small number of events. Hence, the results of our multivariable analyses need to be validated in a larger cohort with more outcome events. Moreover, the collection of data from a referral center could lead to selection bias toward more aggressive cancer. Another limitation is the retrospective nature of the study based on chart review.
In summary, gross ETE of the tumor and presence of DM at the time of thyroidectomy were the strongest predictors of worse DSS. Demographic factors such as age and sex were not predictive of DSS, LR, and DM when adjusted for other variables. Lateral neck LN involvement, gross ETE, and high postoperative Ctn were the strongest predictors of both LR and DM. Hence, disease burden at the time of initial surgery as well as the biochemical response to surgery appear to be more important than demographic factors for MTC prognosis. These findings highlight the importance of rigorous perioperative assessment so as to better predict MTC outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.