
Abstract
Background:
Thyroid hormones are important metabolic regulators exerting effects in multiple systemic functions including muscular and cardiorespiratory function. Thyroid hormones may influence physical activity levels. However, there are currently no studies evaluating the association between thyroid function and physical activity levels in the general population.
Methods:
In a population-based cohort study between 2006 and 2013, we assessed the cross-sectional and longitudinal (with a mean follow-up time of 5 years) association of serum thyrotropin (TSH) and free thyroxine (fT4) with physical activity (metabolic equivalent task [MET] hours per week). Information on physical activity was collected using a validated questionnaire (Longitudinal Aging Study Amsterdam, median 22.50 MET hours per week). The association of TSH and fT4 with physical activity was examined using linear regression models in the cross-sectional and longitudinal analyses, adjusted for age, sex, lifestyle factors, and cardiovascular disease. In sensitivity analyses, we examined the association between thyroid function and physical activity including only participants within the reference range of thyroid function. We additionally examined moderate and vigorous physical activity separately as outcomes.
Results:
We included 2470 participants for the cross-sectional analysis (mean age 57.3 years, 58% women) and 1907 participants for the longitudinal analysis (mean age 56.9 years). There was no association between TSH (mIU/L) or fT4 (ng/dL) and physical activity (β = 0.65, 95% confidence interval [CI, −1.67 to 2.98] and β = 2.76, [CI −7.15 to 12.66], respectively) on cross-sectional analysis. Similarly, in the longitudinal analyses, we observed no association of TSH (β = 1.16, [CI −1.31 to 3.63]) or fT4 (β = −6.63, [CI −17.06 to 3.80]) with physical activity.
Conclusions:
We did not observe an association between the endogenous thyroid hormone level and total physical activity. Further studies need to be performed to evaluate whether thyroid hormone replacement therapy is associated with physical activity.
Introduction
Thyroid hormones are important regulators of the metabolic system (1). During exercise as well as rest, the thyroid hormones affect the muscular and cardiorespiratory function (2). Patients with hypothyroidism can present with profound musculoskeletal weakness, and severe thyroid hormone excess is related to myopathy (3,4). Hypothyroidism, in the clinical and subclinical range, is characterized by chronotropic incompetence, including low heart rate and conduction abnormalities (5,6). Upon treatment with levothyroxine (LT4), hypothyroid patients show improved cardiovascular parameters such as heart rate and cardiac output (7). When thyroid hormones increase, the muscle responds vigorously (5). Previous studies have reported thyroid hormone abuse by professional athletes and strength-training individuals with the aim of enhancing their physical performance (8 –10). Potential benefits are unclear but may be related to cardiac stimulation, muscle performance, and/or fat reducing effects (11).
Thyroid function affects several systems that can change the physical activity and the physical capacity (5). Physical capacity includes factors such as strength, balance, and range of movement (12). These are closely related with the skeletal muscle system (5). Thyroid hormone stimulates the Na/K-ATPase in the skeletal muscle, increasing the transmembrane resting potential (13), and also promotes the expression of myosin heavy chain, a protein characteristic of fast-twitch fibers, the number of mitochondria and the frequency of contraction and relaxation (14). Thyroid hormone may, therefore, very well affect physical capacity through skeletal muscles. Physical activity is related to the movement of skeletal muscles and the resulting energy expenditure (15). Thyroid hormones have a well-known effect on energy metabolism as well (16), generating changes in the demand and synthesis of ATP (16). This may explain a possible link between thyroid function and physical activity.
On the other hand, thyroid function can also negatively impact physical activity through diseases that may hamper a person's general physical performance. For example, thyroid function variations, even within the reference range, have been related to cardiovascular disease (CVD), stroke, and frailty in middle-aged and elderly populations (17 –19). Vice versa, physical activity can also affect thyroid function. For example, physically active people generally have a beneficial cardiometabolic profile including a favorable fat distribution (20). Higher body mass index (BMI) and obesity are known factors influencing thyroid function through production of leptin, which influences the hypothalamic-pituitary-thyroid axis (21).
Altogether, this suggests that thyroid function may be related to physical activity in the general population. The aim of this study was to investigate the association of thyroid function, defined by serum thyrotropin (TSH) and free thyroxine (fT4) and physical activity in a large population-based cohort study.
Materials and Methods
Study population
The analyses were performed using data from the Rotterdam Study, a large prospective population-based cohort study. The rationale, design, and aims have been previously described (22). The Rotterdam Study was initiated in 1989 in the city of Rotterdam, The Netherlands, and included 7983 participants 55 years or older. In 2000, a second cohort of 3011 participants of age 55 years old were added. In 2006, the study was extended with a third cohort of 3932 participants 45 years or older that were not invited before. For this study, we included participants from the Rotterdam Study who had information on thyroid function parameters and measurement on physical activity for the cross-sectional analyses and repeated measurements of physical activity for the longitudinal analyses, as measured by the Longitudinal Aging Study Amsterdam (LASA) questionnaire (Fig. 1). Baseline data were collected from 2006 to 2008 and repeated measures were conducted from 2008 to 2013.
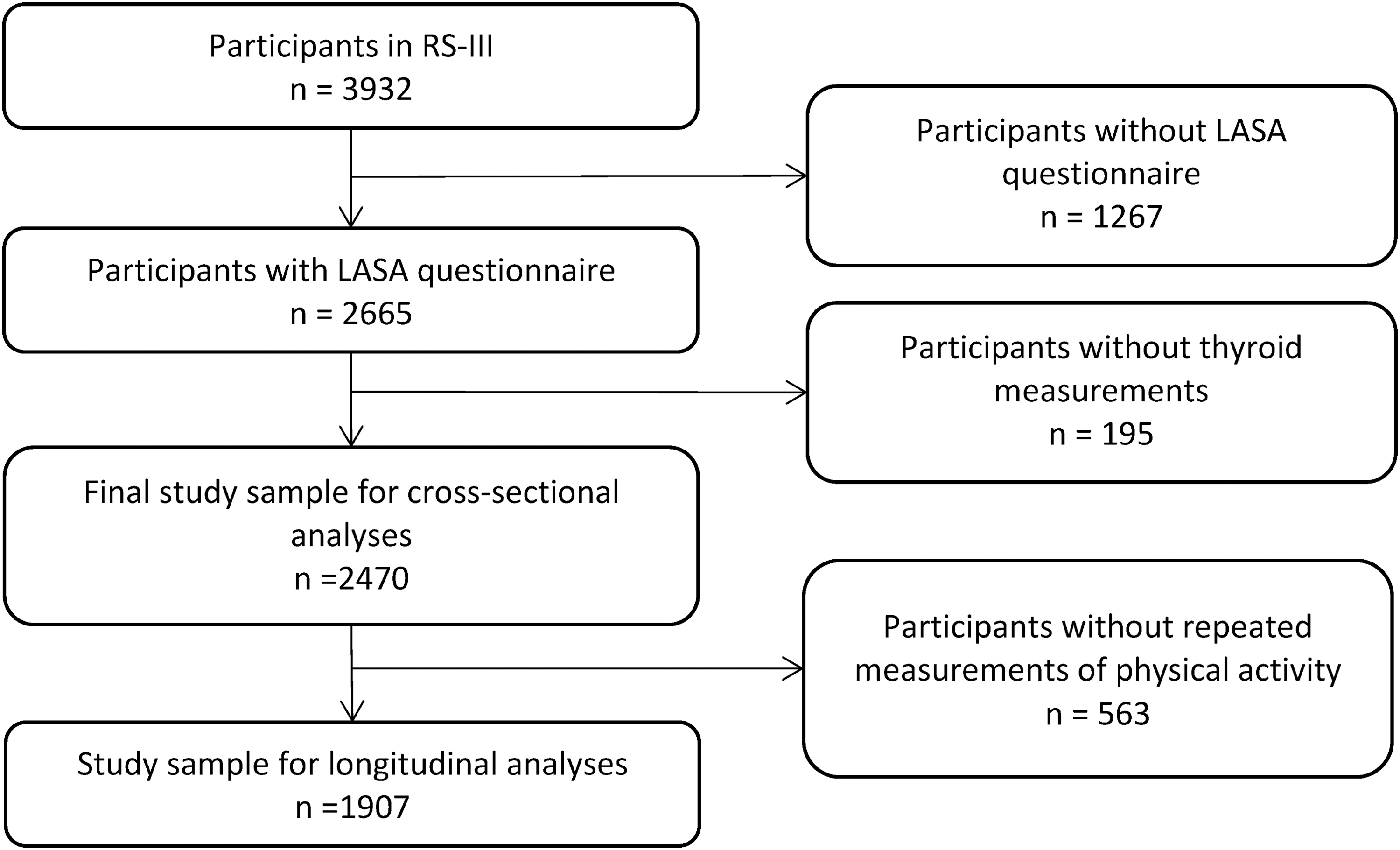
Flowchart of the study sample. RS-III, Rotterdam Study third cohort.
The Rotterdam Study was approved by the Erasmus University Medical Ethics Committee and the Ministry of Health, Welfare, and Sport of the Netherlands, according to the Population Studies Act: Rotterdam Study. In accordance with the Declaration of Helsinki, all participants in this analysis provided written informed consent.
Assessment of thyroid function
TSH, fT4, and thyroid peroxidase antibodies (TPOAb) were measured in serum samples stored at −80°C (electrochemiluminescence immunoassay; Roche). The normal range values were defined for TSH as 0.40–4.0 mIU/L and fT4 as 0.85–1.95 ng/dL, consistent with guidelines and previous studies (17,23). TPOAb levels with a value >35 kU/mL were regarded as positive according to the recommendations of the manufacturer.
Physical activity assessment
Physical activity was evaluated through an adapted version of the LASA Physical Activity Questionnaire (LAPAQ) (24). This questionnaire was validated in the LASA, in which 439 participants aged 69–92 years used a pedometer for 7 days and completed the LAPAQ twice and a 7-day activity diary (24). The LAPAQ had a reasonably good repeatability (0.65–0.75) and the correlations between this questionnaire with the pedometer and the diary were 0.56 and 0.68, respectively (24). LAPAQ has questions concerning the physical activity duration expressed in hours per week and frequency of walking, cycling, sports, gardening, and housework during the previous two weeks (25). Also, the questionnaire has two extra questions to get information about sports that were not asked in previous questions (25).
The intensity of each physical activity was assessed with the metabolic equivalent task (MET). One MET is defined as 1 kcal/(kg·hour) (26). The MET-hours per week for each participant were calculated by multiplying the MET value by time (in hours) spent on the specific activity for each activity and summing all activities per week (26). MET values were assigned to all activities based on the Compendium of Physical Activity of 2011 (27). Sports that were not in this compendium were not included in the analyses (28).
Covariates
We adjusted for potential confounders based on previous research, data availability, and biological plausibility (29,30). Alcohol consumption was assessed with a questionnaire and addressed as number of glasses of alcohol per day. Smoking was assessed with a questionnaire and categorized as never, past, and current smoking. CVD was defined as the presence of heart failure, stroke, atrial fibrillation, or coronary heart disease. The prevalence of CVD was assessed through interview and verified in medical records (22,31). Diet was assessed by a food-frequency questionnaire, and a diet quality score was calculated as described previously (32). Height and weight were measured at the research center and BMI was defined as weight per height2, with weight in kilograms and height in meters.
Statistical analyses
We studied the association of TSH or fT4 with physical activity expressed as MET × hours per week by cross-sectional analysis. Also, we prospectively investigated the association between thyroid function and physical activity as the outcome variable in the longitudinal analyses adjusting for physical activity at baseline. The first model was adjusted for sex and age. The second model additionally included smoking, alcohol, and diet and was regarded as our main model. In a third model, we additionally adjusted for BMI and prevalent CVD, which can be confounders a well as mediators. Furthermore, to explore whether thyroid autoimmunity has a role on physical activity levels, we studied the cross-sectional and prospective association between TPOAb and physical activity, additionally adjusting for TSH or fT4. TSH was logarithmically transformed to approach a normal distribution.
We also performed several sensitivity analyses: (i) in participants with TSH within the reference range (between 0.4 and 4 mIU/L), (ii) additionally by restricting the analysis to participants with fT4 within the reference range (between 0.85–1.95 ng/dL), and (iii) we cross-sectionally and longitudinally performed our analyses in moderate (defined as 3–6 METs) and vigorous (defined as higher than 6 METs) physical activity, measured with LASA questionnaire and expressed in MET × hours per week. In addition, we checked for nonlinearity, but we did not find evidence for that. We checked for interaction between several variables (sex, age, BMI, prevalent CVD, and diet) and thyroid function and planned a stratified analysis if the p-value for interaction was <0.1.
Multiple imputation was performed for covariates with missing data (the rate of missingness for all variables was <1%, except for CVD, BMI, and diet, which were missing in 8%, 9%, and 31%, respectively) (33). Statistical analyses were performed using R statistical software [rms package, R version 3.2.2 (34)].
Results
We included a total of 2470 subjects and their baseline characteristics are summarized in Table 1. Of those, 1907 also had repeated measurement of physical activity. The mean age was 57.3 years and 58% were women. The median TSH was 2.04 mIU/L, with an interquartile range of 1.4–2.79. The mean fT4 was 1.21 ng/dL with a standard deviation of 0.17. The median physical activity was 22.50 MET with an interquartile range of 11.56–40.67 (Table 1). The median TSH and mean fT4 concentrations at baseline were very similar between participants in the cross-sectional analyses and longitudinal analyses (Table 1), with an average follow-up time of 5 years, range 2–8 years.
Baseline Characteristics
Values are in mean and SD unless otherwise specified.
The cutoff for TPOAb positivity was 35 kU/mL.
SD, standard deviation; BMI, body mass index; TSH, thyrotropin; IQR, interquartile range; fT4, free thyroxin; TPOAb, thyroid peroxidase antibodies; CVD, cardiovascular disease; MET, metabolic equivalent task.
Thyroid function and physical activity
In the cross-sectional analyses, there was no association in TSH (adjusted mean difference [β] = 0.65, 95% confidence interval [CI −1.67 to 2.98]) and FT4 (β = 2.76, [CI −7.15 to 12.66]) levels with the baseline LASA physical activity score in model 2 (Table 2). Similarly, there was no association between TPOAb and physical activity (β = −1.51, [CI −6.49 to 3.47]) in model 2 (Supplementary Table S1). Furthermore, our results in the longitudinal analyses also showed no association of thyroid function with physical activity (TSH β = 1.16, [CI −1.31 to 3.63]; and fT4 β = −6.63, [CI −17.06 to 3.80]) in model 2 (Table 3). Also, there was no association between TPOAb and physical activity (β = 2.63, [CI −2.58 to 7.84]) in model 2 (Supplementary Table S2). We did not perform stratification analyses as all p-values for interaction terms for sex, age, BMI, prevalent CVD, and diet were >0.1.
Cross-Sectional Associations Between Thyroid Function and Physical Activity (Metabolic Equivalent Task × Hours per Week)
Model I: Adjusted for sex and age.
Model II: Model I + smoking, alcohol consumption, and diet.
Model III: Model I + BMI and CVD.
N, number; [CI], 95% confidence interval; TSH, log-transformed thyrotropin; β, adjusted mean difference per unit increase.
Longitudinal Associations Between Thyroid Function and Physical Activity (Metabolic Equivalent Task × Hours per Week)
Model I: Adjusted for baseline physical activity, sex, and age.
Model II: Model I + smoking, alcohol consumption, and diet.
Model III: Model II + BMI and CVD.
Sensitivity analyses
After performing our analyses restricting to participants with TSH and fT4 in the reference range, the lack of association of thyroid function with physical activity persisted in both the cross-sectional and longitudinal analyses (Supplementary Tables S3 and S4). After repeating our analyses in participants with hypo- and hyperthyroidism defined by TSH, the lack of association remained (Supplementary Table S5). Also, there was no association of TSH, fT4, or TPOAb with moderate or vigorous physical activity on cross-sectional or longitudinal analysis after adjusting for multiple testing (data not shown).
Discussion
In this large population-based cohort study, there was no association between thyroid function and physical activity levels as assessed by the LAPAQ questionnaire on physical activity.
Most of the studies so far have focused on the relationship between physical activity and thyroid hormones in athletes and military personal (35), while only very few articles have studied the association of thyroid function and physical performance (defined as the disability or satisfactorly performing activities of daily living) in the general population (36). The studies that have investigated this association were conducted primarily in men (35 –37) with very few data on women or with a low sample size (n ≤ 50) (38 –40). Finally, there are no studies that have acquired longitudinal data studying this association. The latter is especially important to disentangle the effect of thyroid hormone on physical activity as opposed to vice versa (i.e., reverse causation). Nevertheless, our results in a large population-based cohort clearly suggest no relationship between thyroid function and physical activity levels in cross-sectional or longitudinal analyses.
One of the explanations for our negative findings could be that while thyroid hormones have clear effects on several components of physical capacity, physical activity entails other factors that are not captured by physical capacity. Physical capacity involves different bodily functions, such as skeleton–muscular and cardiovascular system (41). Thyroid hormones have profound effects on these systems (5). However, the link between physical capacity and physical activity is not completely clear (41). Therefore, better or worse physical capacity may not necessarily translate into differences in levels of physical activity (42).
To date, the association between thyroid autoimmunity and physical activity has not been investigated in a population-based setting. Autoimmune thyroid disease (AITD) is not an uncommon finding in patients with other autoimmune disorders (43,44) such as rheumatoid arthritis (44). In addition, a systematic review suggested that AITD may be associated with osteoarthritis and chronic widespread pain, implicating AITD as an important risk factor for these conditions (45), independent of thyroid function. Despite these possible mechanisms that could change physical activity patterns, our results showed that thyroid autoimmunity itself is not associated with physical activity levels either.
The major strengths of this study are the large number of participants from a population-based cohort. All data were collected irrespective of the baseline thyroid function of participants (i.e., collection was performed blinded). Furthermore, we had a reliable method of outcome ascertainment and were able to adjust for several factors, reducing the possibility of confounding factors.
There are some limitations to our study. The information on physical activity was collected through a self-report questionnaire, where misclassification could be caused by socially desirable answers (24). Furthermore, although the questionnaire showed reasonably good ranking in a previous validation study (24), the LAPAQ was developed and validated for older individuals (69-to-92-year olds) than our study population (45.5–89.4 years), and patterns of physical activity might differ across ages. In addition, we only had information on duration of physical activity. Unfortunately, we did not have information on the intensity of the physical activities. This might lead to nondifferential misclassification of physical activity in our population with higher or lower values than those that were assigned. This could contribute to our estimates being biased toward the null. Furthermore, since our study is observational, one could argue that reverse causation may have affected the results. However, this is unlikely as we have similar findings in the cross-sectional and longitudinal analyses. In addition, although we adjusted extensively for several confounders, residual confounding cannot be completely ruled out. Finally, the Rotterdam Study population is primarily Caucasian, which limits extrapolation to other ethnicities.
In conclusion, our large population-based study suggests that there is no detectable impact of thyroid function on physical activity levels in a sample of predominantly middle-age individuals (45.5–89.4 years) from the general population. We hypothesize that similar results pertain to exogenously determined thyroid function (i.e., in patients who received LT4 therapy). This is relevant in case thyroid hormone therapy is given with the intention to improve daily physical activity levels in adults, especially in individuals with subclinical hypothyroidism. Further studies are required to replicate our results, including other populations (i.e., race/ethnicity and age group) and with patients on LT4 therapy specifically.
Data Availability Statement
Data can be obtained upon request. Requests should be directed toward the management team of the Rotterdam Study (
Footnotes
Authors' Contributions
O.H.R.D. performed the analyses and drafted the article. O.H.F., R.P.P., and L.C. conceived the study and R.P.P. and L.C. supervised the analyses and drafting of the article. All authors and coauthors have taken part in writing the article, reviewing it, and revising its intellectual and technical content.
Acknowledgments
The Rotterdam Study is funded by Erasmus Medical Center and Erasmus University, Rotterdam, Netherlands Organization for the Health Research and Development (ZonMw), the Research Institute for Diseases in the Elderly (RIDE), the Ministry of Education, Culture and Science, the Ministry for Health, Welfare and Sports, the European Commission (DG XII), and the Municipality of Rotterdam. We are grateful to all study participants, the staff from the Rotterdam Study, and the participating general practitioners and pharmacists.
Authors Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5